
Abstract
Background:
Of patients exposed to contrast medium (CM), 10% will develop contrast medium-induced nephropathy (CIN). Many studies have assessed potential risk factors for CIN. There are limited date concerning the influence of gender on frequency of CIN.
Methods:
From January 2001 to July 2004, a prospective trial was performed to compare different treatments for CIN prevention. Creatinine levels (72 hours) were assessed, as well as in-hospital and long-term outcome. CIN was defined as in an increase of ≥25% or >0.5 mg/dL compared with baseline creatinine. The frequency of CIN in women and men was determined retrospectively.
Results:
Four hundred twelve patients (67.1 ± 10.2 years, 68 women) were randomized for different treatment strategies. Univariate analyses identified higher age (p = 0.031), diabetes (p = 0.03), decreased estimated glomerular filtration rate (eGFR) (p < 0.001), lower hemoglobin levels (p = 0.001), use of angiotensin-converting enzyme inhibitors (ACEI) (p = 0.004) and loop diuretics (p = 0.011), the amount of CM given (p < 0.001), and female gender to be associated with the occurrence of CIN within 72 hours. The frequency of CIN within 72 hours after CM administration was significantly higher in women than in men (p = 0.016). When CIN-associated factors were compared between women and men, women were older (69.8 vs. 66.5 years, p = 0.014) and had lower hemoglobin levels (12.6 vs. 13.8 g/dL, p < 0.001) and eGFR (35 vs. 49 mL/min, p < 0.001), suffered more often from diabetes (37% vs. 29%, p = 0.09), and had medication more frequently with loop diuretics (50% vs. 36%, p = 0.036) but not ACEI (56% vs. 57%, ns). The amount of CM given was identical (189 vs. 189 mL, ns). Multivariate analysis found female gender not to be an independent predictor of CIN (odds ratio [OR] 1.48, 95% confidence interval [CI] 0.72–3.02).
Conclusions:
Women are significantly more likely than men to suffer from CIN. This higher rate of CIN was confounded by unfavorable comorbidities, as found by univariate and multivariate analyses.
Introduction
Contrast medium-induced nephropathy (CIN) is an important cause of iatrogenic-induced renal failure associated with significant morbidity and mortality. According to the guidelines of the European Society of Urogenital Radiology, CIN is defined as an absolute increase in serum creatinine levels of ≥0.5 mg/dL or as a relative increase by ≥25% from baseline within 3 days after contrast medium (CM) exposure. 1 CIN is known to be the third leading cause of acute renal failure in hospitalized patients within the United States and Europe, accounting for nearly 10% of all cases of hospital-acquired renal failure. 2
About 10% of patients requiring CM will develop CIN. 3 –7 CIN might range from transient renal dysfunction (nonoliguric, asymptomatic) to severe renal failure (oliguric) with patients who need dialysis or even kidney transplantation. Thus, patients with CIN suffer from a 20-fold increased mortality during their in-hospital stay. 4,5,8 –10 Long-term mortality of patients with CIN might be up to 4-fold higher, ranging from 30% to 40% at 2 years for those not requiring dialysis and from 45% at 1 year to 80% at 2 years for those who develop dialysis-dependent CIN. 4,5,9,10
A large number of studies have focused on CIN prevention, and many studies tried to identify patient-related risk factors predisposing to CIN development. 7,11 –15 For example, Mehran et al. 16 created a risk score to identify high-risk patients who might develop CIN after exposure to CM for percutaneous coronary intervention. The incidence of CIN is exquisitely dependent on the individual clinical characteristics of each patient. Higher age, preexisting renal insufficiency, diabetic nephropathy, congestive heart failure (CHF), reduced left ventricular ejection fraction, hypovolemia and nephrotoxic drugs (e.g., sulfonamides, aminoglycosides) are well-known risk factors that augment the frequency of CIN. Few rare and nonuniform studies are concerned with the significance of gender in increasing risk for CIN. Some studies indicate a higher risk in men, and some indicate a higher risk in women. 17 –21 Therefore, we analyzed retrospectively the influence of gender on the frequency of CIN in a study population taking part in the randomized, controlled Dialysis Versus Diuresis (DVD) trial, which is currently the largest prospective study. 11
Patients and Methods
Study design and objectives
The DVD trial was a randomized, controlled single-center study, performed to test the hypothesis that a combined treatment of hydration plus N-acetylcysteine (NAC) or hydration plus singular hemodialysis would be better than hydration only to prevent CIN. In accordance with the Consolidated Standards of Reporting Trials (CONSORT), the study design is shown in Figure 1. The frequency of CIN in relation to to gender was collected retrospectively.
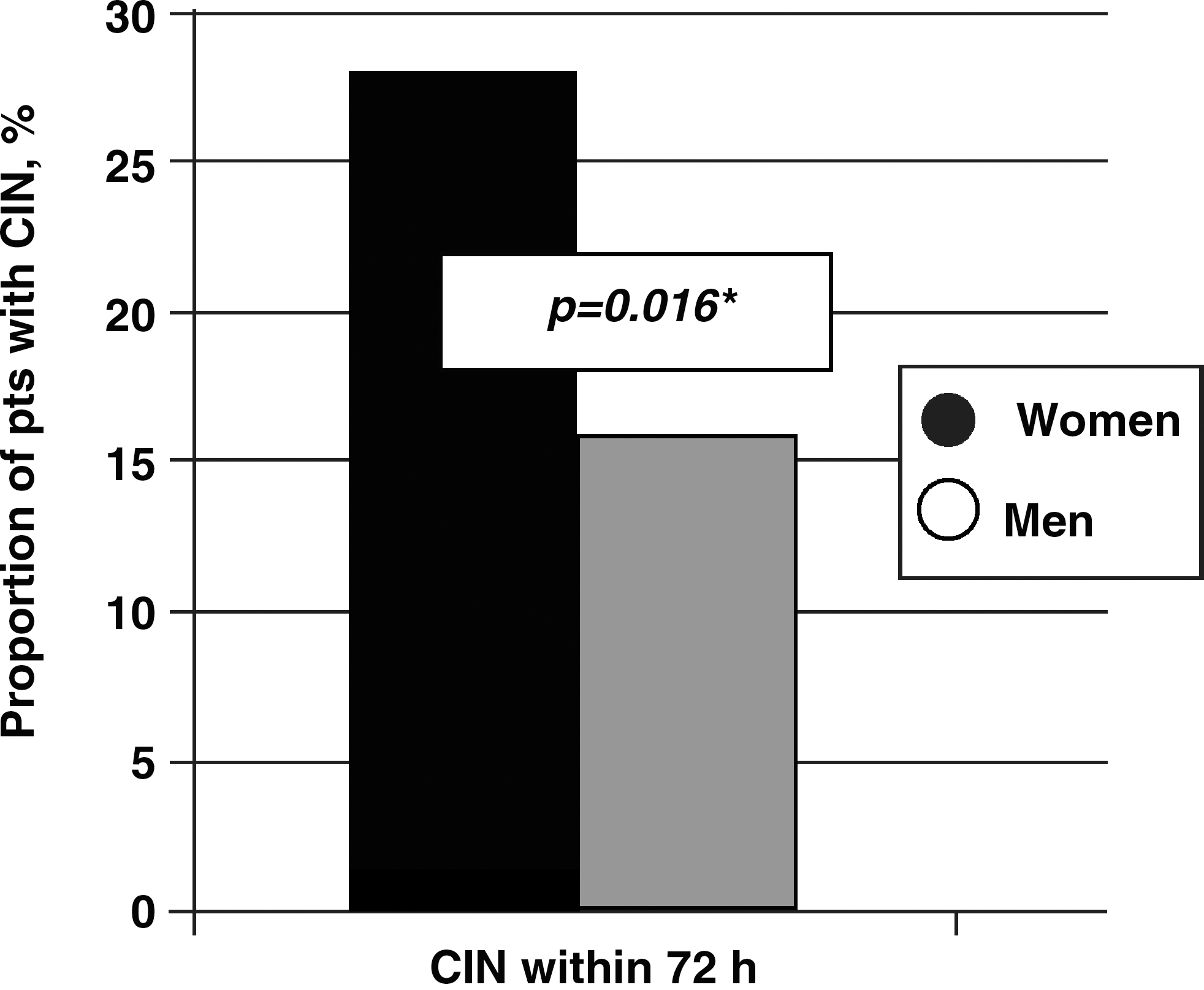
Gender-specific proportion of patients (%) with CIN within 72 hours and 30 days after CM application. CIN, contrast medium-induced nephropathy.
Patients
Patients who were accredited for left heart catheterization between January 1, 2001, and July 6, 2004, were screened for inclusion in the DVD trial. A serum creatinine level of ≥1.3 mg/dL and ≤3.5 mg/dL measured by the method of Jaffé was the major inclusion criterion. Acute or recent (within 30 days) myocardial infarction (MI), CHF (New York Heart Association class IV), transplanted organs, monoclonal gammopathy, and CM application within 7 days prior to the procedure were exclusion selected according to other studies related to this topic. 15,22 –26
Treatment strategies
All patients received hydration therapy of 500 mL 5% glucose and 500 mL isotonic sodium chloride 12 hours before and 12 hours after coronary angiography. 27 One treatment group maintained hydration using the hydration only protocol. The second study group received hydration and a single hemodialysis within 20 minutes after left heart catheterization. The last treatment group received hydration therapy and, additionally, four oral doses of 600 mg NAC. One 600-mg dose of NAC was given the evening before catheterization, the second was given in the morning before catheterization, the third was given in the evening after catheterization, and the last dose was given in the morning the day after CM exposure. 15
Determination of renal function
Serum creatinine determined by the method of Jaffé was used to assess baseline renal function. In each patient, baseline creatinine was additionally determined using the more reliable enzymatic method. Enzymatically determined creatinine concentrations were found within 72 hours after left heart catheterization and were used to calculate the estimated glomerular filtration rate (eGFR) by the simplified modification of diet in renal disease (MDRD) formula:
Corresponding to the classification of the National Kidney Foundation for subgroup analyses, patients were categorized into one of five stages of chronic kidney disease (CKD) according to their eGFR. 10
Outcome measures
The outcome measures were CIN, defined as an increase in enzymatically determined serum creatinine levels of ≥0.5 mg/dL within 72 hours after catheterization, in accordance to other studies. 13,15,28
Heart catheterization
Coronary angiography and percutaneous coronary interventions were performed using arterial access from femoral or brachial arteries. Left ventricular ejection fraction and the number of diseased coronary arteries were categorized in accordance with the revised classification of the American Heart Association and the American College of Cardiology. 29 Angiography was conducted with the nonionic, iso-osmolar CM iopromide (Ultravist 370™, Schering AG, Berlin, Germany).
Hemodialysis
For vascular access, an arterial and venous femoral sheath was inserted. Hemodialysis was conducted for at least 120 minutes with a volumetrically controlled system (MTS 4008C, Fresenius Medical Care, Bad Homburg, Germany). Blood flow rate was 180 mL/min, with a net ultrafiltration rate of zero. First-use, low-flux polysulfone membranes (F8, 1.6 m2, Fresenius Medical Care) were used. The dialysis solution had a flow rate of 500 mL/min, and it was bicarbonate based. Each patient received 2,000 IU of unfractionated heparin for anticoagulation.
Cardiovascular risk factors
Cardiovascular risk factors were evaluated at first date of contact. Hypertension was a documented blood pressure >140/90 mm Hg. If the patient had smoked within the last 10 years, a history of smoking was assumed. A positive family history of cardiovascular disease (CVD) was proposed if a first-degree relative had a history of stroke, MI, or any coronary intervention because of stenosis or occlusion of coronary arteries. Diabetes mellitus existed if the patient was treated with oral antidiabetics or insulin.
Statistical analyses
Differences in the outcome measures for continuous variables were determined by the nonparametric Kruskal-Wallis test. The chi-square test was used for categorical variables. Long-term mortality per 100 patient-years was calculated for the time from entering the trial to September 1, 2004, which was the end of follow-up. The impact of the different treatments on CIN was assessed by bivariate logistic regression. Adjustment for baseline eGFR was made by multivariate models. To compare long-term survival adapted for potential covariates, multivariate Cox proportional hazard models were used. Simply, if covariates were found to be significant (p = 0.1) in univariate mortality analyses, they were included as covariates; each test was two-sided. p Values <0.05 are considered to be significant. All statistical analyses were performed with SPSS 16.0 for Windows.
Results
A total of 8653 patients admitted for elective left heart catheterization were screened for inclusion, and 424 patients gave informed consent to be enrolled in the DVD trial. Twelve patients dropped out because of missed creatinine levels, which left 412 patients remaining in the study.
The proportion of women in the hydration only group, the dialysis group, and the NAC group was 17.1%, 17.4%, and 17.1%, respectively. In the hydration only group and in the hydration plus single hemodialysis group, 24 patients were females (17.1%, 17.4%). In the hydration plus NAC group, 25 were women (17.1%). All together, 51.6% were females and were the center of interest of our retrospective analysis.
Baseline characteristics
Patient baseline characteristics are shown in Table 1. There were no significant differences between confounding factors, such as diabetes, left ventricular dysfunction, or the amount of CM given during the procedure.
CI, confidence interval; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; Lp (a), lipoprotein a; NAC, n-acetylcysteine; SD, standard deviation.
Table 2 shows factors already established as risk factors for CIN development, subdivided according to gender. Females had significantly lower hemoglobin levels (12.6 vs. 13.8%, p < 0.001) and eGFR (35 vs. 49 mL/min/1.73 m2, p < 0.001). Furthermore, females were older (69.8 vs. 66.5 years, p = 0.014), suffered more often from diabetes mellitus (37% vs. 29%, p = 0.09), and more often ingested loop diuretics (50% vs. 36%, p = 0.036). There was no significant difference in use of angiotensin-converting enzyme inhibitors (ACEI) medication (56% vs. 57%) or the amount of required CM for catheterization (189 mL).
Gender-specific distribution of age, hemoglobin levels, eGFR, diabetes mellitus, medication with loop diuretics or ACEI, or the amount of CM given for catheterization. All factors were significantly higher or deeper in females than in males, except the amount of CM given periprocedural or the standard medication with ACEI. The trend shows the difference in the female cohort compared with the male cohort.
eGFR, estimated glomerular filtration rate; ACEI, angiotensin-converting enzyme inhibitors; CM, contrast medium; DM, diabetes mellitus.
CIN within 72 hours after CM administration
Univariate analysis showed an association between CIN within 72 hours and higher age (p = 0.031), diabetes mellitus (p = 0.03), decreased eGFR (p < 0.001), lower hemoglobin levels (p = 0.001), ACEI (p = 0.004) or loop diuretic use (p = 0.011), and the amount of CM given (p < 0.001). CIN occurrence within 72 hours after CM depending on gender is shown in Figure 1. Within 72 hours, CIN occurred significantly more often in woman than in men (p = 0.016).
Multivariate analyses of CIN
To account for baseline eGFR, which theoretically might confound the association of the treatment strategies with the occurrence of CIN within 72 hours after catheterization, logistic regression analyses were performed. The hydration only group was defined as the reference group. Multivariate analyses determined female gender not to be an independent predictor of CIN (odds ratio [OR] 1.48, 95% confidence interval [CI] 0.72-3.02). We also showed that in-hospital death rates were similar between women and men (1.2% vs. 1.5%, ns), as was long-term survival (Kaplan-Meier, 83.6% vs. 82.0%, ns).
Discussion
The impact of female gender on the occurrence of CIN is unclear. In the literature, the impact of gender on frequency of CIN is discussed controversially. In our retrospective analysis of a prospective trial, significantly more women than men developed CIN within 72 hours after CM application. After elimination of confounding factors, multivariate analysis identified female gender not to be an independent predictor for CIN. There were no differences in long-term outcome.
With increasing numbers of examinations using CM and with people getting older and more often suffering from CKD and other risk factor for CIN development, there is a clinical need to predict the qualitative probability of CIN development, to support decisions about management, and, moreover, to search for preventive procedures for concerned patients. CIN incidence is highly dependent on individual clinical characteristics, CM, and the procedure itself. 5,9,10,16 –20,22 –26
Some recent studies identified female gender as a risk factor for CIN. Thus, Iakovou et al. 19 tested the impact of gender on the influence and outcome of CIN after percutaneous coronary intervention (PCI). They identified female gender as an independent predictor of CIN (OR 1.4, 95% CI 1.25-1.6, p < 0.0001). Mueller et al. 20 showed by univariate analysis in 1383 patients that 2.8% of woman developed CIN vs. 0.9% of men. After adjusting for confounders, female sex was no longer a significant independent predictor (OR 2.2, 95% CI 0.8–5.6, p = 0.12). In another retrospective study by Gill et al., 21 146 patients with CKD were analyzed. This study was primarily performed to judge the effect of hydration and NAC. The authors pointed out that gender may be a risk factor for CIN, with hydration offering less protection in woman, and NAC with hydration seemed to reduce the gender difference. Sidhu et al. 30 published a study following prospectively 21,489 consecutive patients undergoing coronary angiography. They showed that rates of CIN in 13,127 analyzed patients were higher for women compared with men in 65–79-year-olds (14.5% vs. 11.0%, p < 0.001) and in patients >80 years (18.7% vs. 15.1%, p = 0.048). No differences were seen in younger cohorts. In contrast, Rudnick et al. 17 published a study in 1995 about the nephrotoxicity of ionic and nonionic CM in 1196 patients in a randomized trial. By multivariate analysis, male gender was independently related to the risk of nephrotoxicity.
In summary, a majority of the studies supported our results that female gender is associated with increased rates of CIN. However, our trial is the only one providing data that this effect is not depending on gender itself but is confounded by other comorbidities, which were distributed unfavorably in women. The reason for higher CIN rates in woman is still unknown. Some assume that a gender-specific response to renal stimuli by the contrast agent may be a possible explanation. 19 Gill et al. 21 found that older women compared with younger women had lower intrarenal medullary oxygenation, which may be linked to lower intrarenal medullary vasodilatory prostaglandin production, a potential factor for increased susceptibility to acute tubular necrosis. Platelet response and reactivity, including greater sensitivity of women's platelets to aggregating stimuli, and perhaps the influence of ovarian hormones also have been implicated in the evolution of renal failure. 19,27,28
Finally, one has to consider, that CVD is the leading cause of death in woman, responsible for more deaths per year than all other causes combined. 29,31 Cardiovascular mortality in woman is higher than in men, most likely an effect of more underlying comorbidities. 32 Woman with coronary artery disease (CAD) are more often asymptomatic or suffer from atypical symptoms more than men. This leads to the so-called gender gap, that is, that the risk for CAD is underdiagnosed in woman. Thus, if women undergo invasive diagnosis, they suffer much more frequently from an advanced stage of disease and more comorbitides; this may be a reason for higher rates of CIN. To completely understand the influence of gender further, prospective studies are recommended.
Limitations
Our study has several limitations. First, our analysis has a single-center design. The second limitation is the small cohort of patients. We did not prospectively divide the participating patients into different groups according to their age, as Sidhu et al. did recently. 30 The third limitation is the retrospective design.
Footnotes
Acknowledgments
We are indebted to all technicians, nurses, and doctors in the catheterization laboratories, the hemodialysis unit, and on the wards for their ongoing support.
Disclosure Statement
The authors have no conflicts of interest to report.