
Abstract
Background:
Violence against women (VAW), including intimate partner violence (IPV) in its various forms (sexual, physical, or stalking), and childhood violence (sexual or physical) are common and are associated with depressive symptoms. We examined the association between these violence exposures and self-reported history of postpartum depression (PPD).
Methods:
Women from the Kentucky Women's Health Registry (KWHR) who reported at least one live birth were included in this study. Individual IPV and child abuse histories were examined for association with self-reported history of PPD. Multivariate regression analysis estimated adjusted risk ratios (aRR) and 95% confidence intervals (95% CI), controlling for age, obstetrical history, and substance abuse history.
Results:
The 5380 women in the KWHR reporting at least one live birth were included in this study. Of these women, 2508 (46.6%) reported a history of any VAW. A history of adult VAW was associated with a history of PPD (aRR 1.48, 95% CI 1.12–1.95). Physical IPV (aRR 1.48, 95% CI 1.12–1.95) and stalking IPV (aRR 1.39, 95% CI 1.03–1.87) were individually associated with PPD. Other types of violence were not individually associated with a history of PPD. The strength of association increased with each additional type of violence experienced (aRR 1.17, 95% CI 1.06–1.30).
Conclusions:
Adult VAW is associated with self-reported history of PPD. With an increase in the number of types of abuse experienced, this association became stronger. Our findings highlight the need for thorough VAW screening in obstetrical populations.
Introduction
Violence against women (VAW), including intimate partner violence (IPV), is a prevalent problem, with 25%–50% of women experiencing some form of abuse in their lifetime. 1 Characteristically, this type of abuse is chronic and recurrent and involves multiple forms of violence. 1 Physical, sexual, and psychological abuse have been linked to development of chronic physical and mental illness, including depressive symptoms. 2 –5 Depressive symptoms are associated with increasing severity of abuse. 3 Both recent and remote IPV events have been associated with depression. 4 Stalking has been examined as a unique form of abuse and can be considered in the spectrum of IPV, as those perpetrating the stalking frequently are former intimate partners and because of the incumbent risk of physical and psychological abuse victimization. 6,7
Most studies of VAW and pregnancy have focused on fetal and neonatal death, infectious morbidity, birthweight, preterm birth, 8 –16 and maternal trauma. 12,17 Physical abuse before or during pregnancy is associated with a prevalence of self-reported postpartum depression (PPD) symptoms in both epidemiological and clinical studies. 18 –20 These studies have found associations with partner violence during pregnancy, 18 in the year before delivery, 19 and 2 years before delivery. 20 Given the chronic nature of VAW and that remote exposures have been associated with depression, 4 lifetime history of VAW is potentially an important risk factor for PPD.
The epidemiology of adverse childhood events (including physical, emotional, and sexual abuse; living with parents who were separated or divorced; or living with parents with problems with substance abuse or mental illness) suggests an association between these forms of abuse and depressed affect later in life. 21,22 The greater the number of types of abuse experienced, the more likely women are to report depressive symptoms. 21 –23 The different types of abuse are associated individually with depressive disorders later in life. 22 A history of childhood physical or sexual abuse has been associated with an increase in depression and hospitalization for mental illness in women. 24 –26 Both childhood and adult abuse histories, both current and past, are important risk factors for depressive symptoms. 26
To better understand the complex associations between VAW in its multiple forms and PPD, we examined these associations in a large sample of women in Kentucky. We hypothesized that women with a lifetime history of VAW, when compared to women with no lifetime history of VAW, would be more likely to report a history of PPD. We investigated the association between specific types of violence, individually and as an aggregate, and their association with PPD.
Materials and Methods
Data source
We analyzed data from the Kentucky Women's Health Registry (KWHR). The KWHR has been described in detail previously. 27 Briefly, this registry is a comprehensive survey open to all women, aged ≥18 years, living in Kentucky. The purpose of the registry is to improve healthcare for Kentucky women by understanding how behavioral factors may differentially affect women's health. Consent and the Health Insurance Portability and Accountability Act (HIPAA) waivers were obtained from all participants upon enrollment in the registry. The KWHR granted approval for use of the registry data for this study. Our study was granted IRB review exemption by the University of Kentucky.
Women are asked to complete the survey annually, and approximately one third of women have completed multiple questionnaires. From the time of beginning our analysis (August 2009), 7932 women aged ≥18 years had enrolled in the registry and had completed at least one survey. The majority of women (82.3%) have completed the survey using a secured website; the remaining women completed a paper version of the same questionnaire. All data are de-identified, self-reported, and not verified by medical records as per the registry consent. We restricted our analysis to data from each woman's initial questionnaire. Additionally, we included only parous women (women reporting at least one childbirth) so as to identify those at risk for PPD.
Variables
Violence/abuse exposures
Women may experience gender-based violence in either adulthood or childhood. The perpetrator could be a family member, an intimate partner, or a stranger. The KWHR questionnaire includes items to ascertain violence and abuse exposures based on the questions in the Behavioral Risk Factor Surveillance System (BRFSS). 28 Three items ask about IPV: For physical IPV: Has an intimate partner hit, kicked, punched, or otherwise hurt you? For sexual IPV: Has an intimate partner used force (like hitting, holding down, or using a weapon) to make you have sex? For stalking: Has an intimate partner ever repeatedly followed you, spied on you, made unsolicited phone calls to your place of work or at home, damaged your property, or stalked you in any way? One item asks about nonintimate partner forced sexual experiences: Has anyone other than an intimate partner or anyone else used force (like hitting, holding down, or using a weapon) to make you have sex?
Two items ask about childhood abuse. For physical abuse: When you were a child, did any parent, stepparent, or guardian ever hit, kick, punch, or otherwise hurt you? For sexual abuse: When you were a child, did any parent, stepparent, or guardian or any other person make you have sex (any sex act, not just intercourse) by using force or threatening to harm you or someone close to you?
From these six questionnaire items, eight dichotomous variables were created to characterize a lifetime history of victimization. Six dichotomous variables were created for each of the six specific types of violence. Additionally, two summary variables were created. Any violence exposure: a history of ever experiencing any of the forms of violence. Any adult VAW exposure: a history of ever experiencing physical IPV, sexual IPV, stalking, or a forced sexual encounter with a nonintimate partner. Women who gave a negative response to all six of the abuse history questions represent our unexposed group. We examined lifetime history of violence, as the KWHR questionnaire does not contain the information needed to construct a timeline of events. Consequently, we were able to ascertain neither the timing nor duration of each individual violence exposure.
Postpartum depression
Women were asked to provide details of pregnancy history, including a self-reported history of PPD. The KWHR uses a check-box yes/no item to capture history of PPD with the following operationalized definition: Significant symptoms of depression which women experience within a few days of giving birth and may continue to experience for weeks or months following delivery. The KWHR does not link these symptoms to a specific pregnancy.
Potential confounders
Self-reported demographic and obstetrical factors were considered in assessment for confounding. Demographic factors include age, race/ethnicity, highest educational status attained, and current marital status. Race and ethnicity were dichotomized to white, non-Hispanic and other, as the registry participants, like the general Kentucky population, are predominantly white, non-Hispanic.
Substance abuse, in multiple forms, was also considered. Smoking status was characterized as current, former, and never smoked. Alcohol abuse was evaluated with self-reports of being a problem drinker, having difficulty quitting alcohol use in the 12 months before completion of the survey, and history of difficulty with alcohol use cessation. Prescription drug abuse (pain pills, sleeping pills, nerve pills, diet pills) and history of illegal drug abuse (marijuana, cocaine, heroin, methamphetamines, and ecstasy) were also evaluated.
The questionnaire assesses a self-report history of preterm labor, third trimester bleeding, preeclampsia, and gestational diabetes. These obstetrical factors were first evaluated individually and then in the aggregate using a dichotomous variable for history of a complicated pregnancy. We also examined a history of breastfeeding after any pregnancy in our analysis of confounding.
Statistical analysis
We performed an analysis of questionnaire data from the KWHR using STATA/IC10 (StataCorp, College Station, TX). Demographic characteristics were tabulated for women with VAW histories and for women reporting no history. Unadjusted odds ratios (uOR) and 95% confidence intervals (95% CI) were used in bivariate analysis to evaluate the differences between the two groups of women using a binary regression model with the logit link function, assuming a binomial distribution for each demographic factor. For each violence exposure, unadjusted rate ratios (uRR), adjusted rate ratios (aRR), and 95% CI were calculated using a binary regression model with the log link function, assuming a binomial distribution, with PPD as the dichotomous outcome. The reference group for all models was women who experienced none of the forms of VAW. Coviariates were evaluated in a forward-stepwise manner and included in the multivariate model if they changed the rate ratio by >10%, as described by Greenland and Rothman. 29 Two multivariate models examining the relationship between each of the two forms of childhood abuse and PPD were constructed. One model included the variable, any adult trauma, as a covariate; the other did not include this variable. This was done to assess the possibility that childhood abuse history and adult abuse history may be in the same pathway leading to an increased risk of PPD.
Results
Of the 7932 women in the registry, 5443 (68.6%) reported having at least one live birth on their initial questionnaire and, therefore, were included in this analysis. There were 63 (1.2%) women not answering questions on violence history who were excluded from subsequent analysis.
In our remaining sample of 5380 women, those reporting a history of any VAW (n = 2508, 46.6%) were more likely than those never experiencing VAW to be a nonwhite race (uOR 1.80, 95% CI 1.40–2.31), to be separated from their spouse (uOR 4.73, 95% CI 2.92–7.65), or to be currently divorced (uOR 2.86, 95% CI 2.46–3.34), not to have completed a baccalaureate or graduate degree (uOR 1.61, 95% CI 1.44–1.80) to be a current (uOR 3.35, 95% CI 2.83–3.93) or former (uOR 1.79, 95% CI 1.58–2.03) smoker, to report being a problem drinker (uOR 3.00, 95% CI 2.29–3.93), to have had difficulty quitting alcohol use in the year before completing the questionnaire (uOR 5.17, 95% CI 2.90–9.23) or ever during their life (uOR 3.24, 95% CI 2.03–5.16), and to report a history of illegal drug (uOR 4.67, 95% CI 3.12–6.99) or prescription drug (uOR 2.40, 95% CI 1.05–2.80) abuse (Table 1).
CI, confidence interval; OR, odds ratio; VAW, violence against women, including childhood abuse.
In bivariate analysis, all the adult violence exposures were associated with PPD (Table 2). After controlling for age, current marital status, smoking status, history of problem drinking, history of illegal drug use, history of prescription drug abuse, history of complicated pregnancy, and breastfeeding history, it was found that women with a history of VAW exposures were approximately 40% more likely to report a history of PPD (aRR 1.37, 95% CI 1.04–1.81). The strength of association was similar for a history of PPD and a history of physical IPV (aRR 1.48, 95% CI 1.10–1.99), sexual IPV (aRR 1.34, 95% CI 0.89–2.02), and stalking IPV (aRR 1.39, 95% CI 1.03–1.87).
History of any of the following: physical intimate partner violence (IPV), sexual IPV, stalking IPV, non-IPV forced sex, childhood physical abuse, or childhood sexual abuse.
Controlling for age (continuous), current marital status, smoking status (current, former, never), history of problem alcohol use, history of illegal drug use, history of prescription drug abuse, history of complicated pregnancy (history of preterm labor, gestational diabetes, preeclampsia, or third trimester bleeding), and history of breastfeeding.
Models for childhood abuse exposures are presented in Table 3. In univariate analysis, both childhood physical abuse (uRR 1.39, 95% CI 1. 22–1.58) and childhood sexual abuse (uRR 1.48, 95% CI 1.26–1.74) were associated with PPD. After controlling for age, current marital status, smoking status, history of problem drinking, history of illegal drug use, history of prescription drug abuse, history of complicated pregnancy, and breastfeeding history, childhood physical abuse (aRR 1.47, 95% CI 1.04–2.07), but not childhood sexual abuse (aRR 1.22, 95% CI 0.80–1.88), was associated with PPD. After adding an additional variable for any adult violence exposure, we did not observe significant changes in the point estimates for either childhood physical abuse (aRR 1.34, 95% CI 0.94–1.90) or childhood sexual abuse (aRR 1.16, 95% CI 0.75–1.78).
Controlling for age (continuous), current marital status, smoking status (current, former, never), history of problem alcohol use, history of illegal drug use, history of prescription drug abuse, history of complicated pregnancy (history of preterm labor, gestational diabetes, preeclampsia, or third trimester bleeding), and history of breastfeeding.
An obvious trend was seen for increasing risk of PPD with increasing number of types of abuse experienced (Fig. 1). When number of types of violence experienced is modeled as a ordinal variable (range 0–6), for each incremental increase in number of types of violence reported, there is a significant increase in the likelihood of reporting PPD (aRR 1.17, 95% CI 1.06–1.30) when controlling for age, current marital status, smoking status, history of problem drinking, history of illegal drug use, history of prescription drug abuse, history of complicated pregnancy, and breastfeeding history.
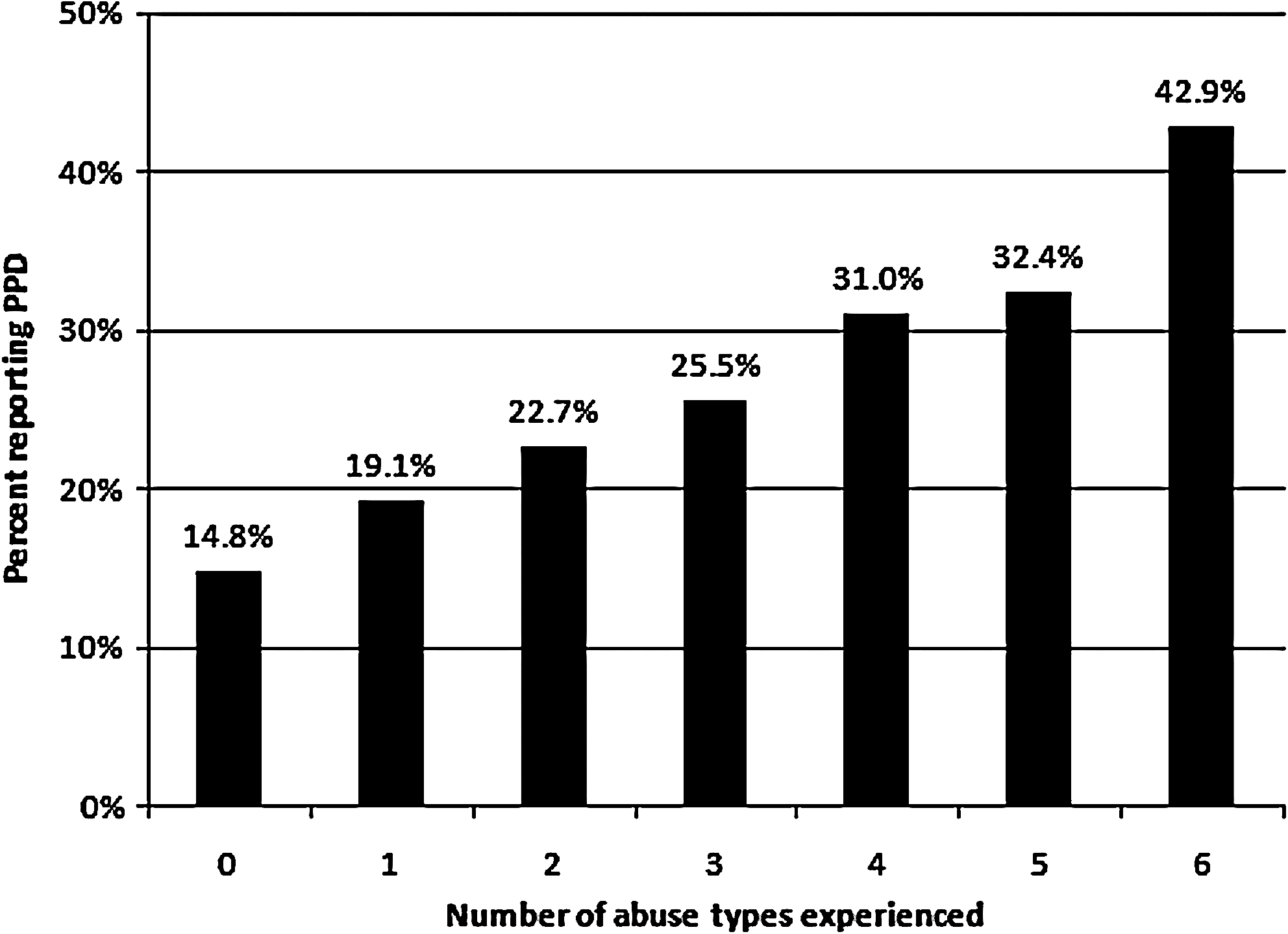
Abuse history and history of postpartum depression (PPD).
Discussion
Consistent with prior reports, 1 we found that 46% of 5443 parous women in the KWHR report a lifetime history of VAW. In bivariate analysis, all violence exposures were associated with PPD. After controlling for age, current marital status, substance abuse, pregnancy complications, and history of breastfeeding, we found that the more types of violence experienced, the stronger the association with reported history of PPD. When examining specific exposure types, a history of physical abuse and partner stalking was statistically significantly associated with reporting a history of PPD. A history of either adult sexual abuse or nonintimate partner-forced sexual encounters was not significantly associated with a history of PPD. The effect size, however, was consistent with those seen with other adult abuse exposures. The lack of statistical association may be a reflection of fewer women reporting a history of adult sexual abuse. Alternatively, this may reflect different associations between the individual exposures and PPD.
The individual types of violence frequently co-occur with other types. In one study of women reporting a history of physical abuse, approximately 80% of these women reported two or more forms of abuse. 1 In our dataset, of the women who reported a history of VAW, 55% reported two or more specific types of abuse. In examining women reporting only one type of abuse vs. women with no abuse history, our analysis suffered from small numbers in the exposed groups and, consequently, insufficient power to detect differences (data not shown).
Although girls are not uniquely the victims of childhood physical abuse, we included this exposure in our spectrum of possible VAW exposures, as the perpetrator is frequently a person in the position of being a caregiver, and this abuse is a violation of trust, similar to that frequently found with IPV. After controlling for a history of any adult abuse exposures in multivariate analysis, there were no statistically significant associations between childhood abuse exposures and reported history of PPD. Addition of the term for adult abuse in the childhood abuse models likely overcontrolled for the abuse exposure. We suggest that the association between childhood events and PPD may be mediated through a common pathway of childhood abuse leading to an increased risk of adult abuse among survivors of childhood abuse. Alternatively, this may reflect the influence of bias, with those reporting both childhood and adult exposures being more likely to report a history of depressive symptoms.
There are some limitations to our analysis that should be recognized. We are unable to evaluate the temporal relationships from the cross-sectional data from the KWHR, which does not ask women to create a timeline for life events. Depressive symptoms may have preceded abuse exposures. Depressive symptoms are known to increase the risk of subsequent IPV, 30 and, therefore, one must recognize that these observed associations may be bidirectional.
Our operationalized definition of PPD was not verified against the medical record. We are unable to discern if respondents correctly differentiated between true PPD and postpartum blues or other affective disorders in the postpartum period. Although assessment of self-reported PPD symptoms has been shown to overestimate the prevalence from structured interviews (14% vs. 12% in one meta-analysis), 31 we did find a prevalence of reported PPD of 14.8% among women who did not report a history of any violence exposures, consistent with the reported prevalence of PPD. 31 –34 Additionally, this convenience sample of self-report questionnaires is not representative of the Kentucky population. Women who participate in the KWHR are older and more highly educated that most women in Kentucky. Despite these differences, we found a 28.7% lifetime prevalence of physical or sexual IPV in the KWHR, which is greater than that reported in the National Violence Against Women report of 22.1% lifetime IPV. 35 According to Kentucky BRFSS data, 28.0% of Kentucky women are current smokers, more than the 20.3% of women in our study. 36 Our sample is composed of women more highly educated than expected for Kentucky, with 44.4% having at least a college education, compared to <30% of women in the Kentucky BRFSS.
Individuals in abusive relationships might not be comfortable with disclosure of their situation. Women may not be willing to disclose a history of IPV or child abuse, or if disclosed, the full extent of such abuse might not be revealed. Partners may be controlling and not allow participation in the registry, may monitor computer use, or may threaten further abuse with disclosure of the situation. This would lead to an under reporting of violence history. We anticipate that this would tend to minimize the strength of association and bias our findings toward the null hypothesis. Additionally, the magnitude, duration of exposure, and psychological trauma incurred through victimization are also not fully characterized in our data. Thus, we may be unable to investigate the true relationship of each type of violence exposure with depressive symptoms.
Conclusions
Adult VAW is associated with self-reported history of PPD. Further research is needed to better understand this association and to clarify implications for clinical practice. Although we cannot establish causality, our data suggest that women reporting the most cumulative exposure to violence are most likely to report PPD. This strengthens the argument for comprehensive screening for the psychosocial risk factors of PPD and suggests a role for active screening and intervention to potentially reduce the burden of PPD.
The American College of Obstetricians and Gynecologists and the American Academy of Pediatrics recommend screening for VAW and depressive symptoms. 37 –39 Screening for depression can be accomplished with a simple two-question screen, leading to increased recognition of depression. 40 Physicians have identified many barriers to screening, 41 but it has been demonstrated that screening for partner violence can be reasonably accomplished in the office. 42 Furthermore, home visitation in the postpartum period may be an effective strategy for reducing child maltreatment as a consequence of partner violence, 43 as well as partner violence itself. 44 We believe all providers involved in perinatal care should be cognizant of the consequences of VAW and must screen for VAW and PPD so as to increase recognition and to facilitate referral, counseling, and treatment of affected women.
Footnotes
Acknowledgments
We acknowledge Mary Johnson, Dongying Zhong, Ashley McCorkle, and Tyson France for their work on the KWHR project. We also acknowledge the contributions of the KWHR statistician, Heather Bush, Ph.D. The KWHR is funded by the University of Kentucky.
Disclosure Statement
No competing financial interests exist.