
Abstract
Background:
The present study aims to determine the predictive power of activin A levels in the prognosis of first trimester pregnancies conceived by in vitro fertilization (IVF).
Methods:
The study cohort included 23 biochemical, and 23 normal ongoing pregnancies conceived via IVF. Serum β-human chorionic gonadotropin (β-hCG), progesterone, and activin A levels were assessed 14 days after embryo transfer.
Results:
Serum activin A levels were significantly lower in biochemical pregnancies compared to normal ongoing pregnancies (0.57 vs. 0.81 ng/mL, p<0.001). The ability of activin A to predict normal ongoing pregnancies at a cutoff level of 0.695 ng/mL gave a sensitivity of 91.3%, a specificity of 100%, a positive predictive value of 100%, and a negative predictive value of 92%. Significant correlation was found between β-hCG and progesterone, β-hCG and activin A, and progesterone and activin A. Activin A, β-hCG, and progesterone were all found to be efficacious in prediction of early IVF pregnancies.
Conclusions:
The present study indicates that single measurement of activin A can be suggested as a marker for the progress and outcome of early pregnancies conceived via IVF. However, further large-scale studies are required to determine the efficacy and reliability of activin A in prediction of early pregnancies achieved by assisted reproductive techniques (ART).
Introduction
An in vitro fertilization (IVF) program is a stressful process that can be associated with adverse obstetrical outcomes. That is why early prediction of pregnancy outcome is important for both practitioners and couples participating in IVF programs. 1
To date, several biochemical markers have been used to predict the clinical course of early pregnancies. 2 –7 Serial β-human chorionic gonadotropin (β-hCG) and progesterone measurements of serum have been used to predict the pregnancy outcome. A serum progesterone level of <20 nmol/L has been shown to be predictive of failing pregnancy. 2 Other markers include creatine kinase, cancer antigen-125 (CA-125), and inhibin A. 5 –7
Activin A is a dimeric glycoprotein belonging to the transforming growth factor-β (TGF-β) superfamily, which is a group of functionally diverse growth factors involved in cellular proliferation and differentiation. 8 It is secreted by the fetomaternal unit, and it is thought to be a marker of trophoblastic invasion, with the potential to identify patients at risk of miscarriage and ectopic pregnancy. During pregnancy, the placenta is the main source of activin A, so that activin A levels increase throughout pregnancy until delivery. 9 Activin A may stimulate the release of prostaglandin from fetal membranes in the mechanisms of labor and potentiates the release of hCG in primary cultures of human placental cells, supporting the hypothesis that activin A plays a pivotal role in the endocrine physiology of human pregnancy. 8,9
Florio et al. 9 reported that activin A levels in gestational fluids may help early diagnosis of placental tumors and miscarriages and also facilitate the follow-up of hypertensive disorders of pregnancy, fetal hypoxia, and intrauterine growth retardation (IUGR). They also stated that measurement of activin A during the first trimester of pregnancy could be useful in the diagnosis of trophoblast dysfunction and, therefore, be helpful in management of early pregnancy problems and to predict the first trimester pregnancy outcome in patients with early pregnancy vaginal bleeding due to threatened abortion. Lockwood et al. 10 found that higher levels of activin A were associated with multiple gestations, whereas rapidly falling levels heralded embryonic demise. The fetoplacental unit is thus confirmed as the major source of the glycoprotein.
There are limited data on activin A measurements in patients undergoing IVF, evaluating the follicular development and fertilization rate. 11,12 The aim of the present study was to determine the predictive power of single serum activin A measurements in the prognosis of first trimester pregnancies conceived by IVF and, thus, to evaluate its usefulness in the implantation success of IVF pregnancies.
Materials and Methods
The present prospective study was approved by the Institutional Review Board and Ethical Committee of Zekai Tahir Burak Women's Health Care Education and Research Hospital, where the study was conducted. Written informed consent was obtained from all subjects.
The study cohort included 23 biochemical and 23 normal ongoing singleton pregnancies conceived by IVF. Biochemical pregnancies and normal ongoing pregnancies up to 12 weeks were conceived by IVF programs in the department of reproductive endocrinology between June 2008 and December 2008. Diagnoses of normal ongoing and biochemical pregnancies were based on clinical assessment and evaluation by transvaginal ultrasonography, using a 7.5-MHz transvaginal probe with an SSD-1000 ultrasound scanner (Aloka), and serial serum β-hCG assays. A live intrauterine pregnancy was excluded when serum β-hCG levels increased <66%, plateaued, or decreased over 48 hours. Diagnosis of a normal ongoing pregnancy was made by the presence of a live embryo on ultrasonography. Biochemical pregnancy was defined as a decrease in β-hCG level to <5 mIU/mL. Duration of pregnancy was determined as the period 14 days before embryo transfer to the day of the testing.
Indications for IVF treatment were tubal factor, male factor, and unexplained infertility. Patients included in the study had regular spontaneous menstrual cycles (22–35 days) and were aged <40 years. All patients had acceptable follicular phase serum concentrations of follicle-stimulating hormone (FSH) (≤10 IU/L), luteinizing hormone (LH) (<10 IU/L), and estradiol (<60 pg/mL), body mass index (BMI) ≤30 kg/m2, the presence of both ovaries and normal uterine cavity, and no assisted reproductive technique (ART) attempts for at least two full menstrual cycles. Patients were excluded from the study if they had any clinically significant systemic disease, polycystic ovary syndrome (PCOS), a previous history of severe ovarian hyperstimulation syndrome (OHSS), abnormal gynecological bleeding of unknown origin, or a previous history of intolerance to any of the agents used in the study. The patients with PCOS, endometriosis, or other diseases causing infertility were not included because these pathologic conditions may influence the levels of activin A.
All women were treated with a long stimulation protocol in which gonadotropin-releasing hormone (GnRH) analogue (leuprolide acetate) was given as a pretreatment and recombinant FSH (rFSH) administration was started when pituitary desensitization was confirmed by the presence of small antral follicles (diameter 2–6 mm), an endometrial thickness <5 mm, and serum estradiol level <50 pg/mL. From day 7 of stimulation, daily monitoring of follicle size by ultrasound was performed, and plasma levels of estradiol were measured. The dose of rFSH was adjusted according to the individual response of each patient. Ovulation was triggered with hCG when plasma estradiol levels reached 1000–4500 pg/mL and at least four follicles >16 mm diameter were visualized on ultrasonography. Ovulation triggering was performed by an intramuscular injection of 10,000 IU highly purified preparation of hCG.
Oocyte retrieval was performed under ultrasound guidance by the transvaginal route 34–37 hours after hCG administration. Intracytoplasmic sperm injection (ICSI) was performed in all patients, as ICSI is the standard practice for all IVF procedures at the study center. Embryos were transferred 48–72 hours after insemination with an embryo transfer catheter. All transfers were performed by the same physician in order to avoid interoperator variability. All pregnancies were confirmed by a rising titer of serum β-hCG from 14 days after embryo transfer. Progesterone and activin A levels were assessed in participants with a positive serum β-hCG using the same serum sample. Although serial measurements of serum β-hCG were used to determine the certain diagnosis, the first assays (14 days after embryo transfer) were used in analyses. The luteal phase was supplemented only with micronized progesterone once daily vaginally (Crinone 8% vaginal gel, Merck Serono). None of the patients have taken exogenous systemic progestogens.
Serum β-hCG concentrations were measured by Micro-ELISA Test Kit (Leinco Technologies Inc.), which had a sensitivity of 0.8 mIU/mL, and serum progesterone levels were measured by the AutoDelfia Progesterone Kit (Perkin Elmer) with an analytical sensitivity of >0.25 ng/mL. Serum activin A concentrations were determined by Activin A assay (Oxford Bio-Innovation Ltd.), with interplate and intraplate coefficients of variation (CV) <10% and an analytical sensitivity of >0.05 ng/mL.
Data analysis was performed using SPSS for Windows, version 11.5 (SPSS Inc.). The distributions of continuous variables were determined using the Shapiro Wilk test. Data were shown as mean±standard deviation (SD) or median (minimum-maximum) where applicable. Nominal data were expressed as number of cases and percent. The mean differences between groups were compared by Student's t test. Mann Whitney U test was applied for comparisons of the median values. Nominal data were analyzed by Pearson chi-square or Fisher's exact test where appropriate. Precorrelation between clinical markers was evaluated by Pearson's correlation test. Logarithmic transformations were applied for all clinical markers in correlation analyses because of the not normally distributed. Area under the curve (AUC) and 95% confidence interval (CI) for clinical marker (activin A, β-hCG, and progesterone) discrimination of normal ongoing pregnancies from biochemical pregnancies was evaluated by receiver operator characteristics (ROC) analysis. The best cutoff points, sensitivity, specificity, and positive and negative predictive values were also calculated. A p value <0.05 was considered statistically significant.
Results
The study cohort consists of 23 normal ongoing and 23 biochemical pregnancies conceived via IVF. Table 1 summarizes demographic characteristics and previous pregnancies. The mean age of the women with normal ongoing pregnancy was significantly younger than that of women with biochemical pregnancies. Table 2 shows that the group with biochemical pregnancies and the group with ongoing pregnancies did not differ statistically significantly in indications for IVF, the number of trials, the number of oocytes collected or embryos transferred, the duration of amenorrhea, or estradiol levels at the hCG day. Serum β-hCG, progesterone, and activin A levels and progesterone/activin A and β-hCG/activin A ratios were significantly higher in the normal ongoing pregnancy group (p<0.001). The ROC curves for activin A, β-hCG, and progesterone are shown in Figure 1. According to the ROC analyses, activin A, progesterone, and β-hCG were efficacious in predicting normal ongoing pregnancies (p<0.001).
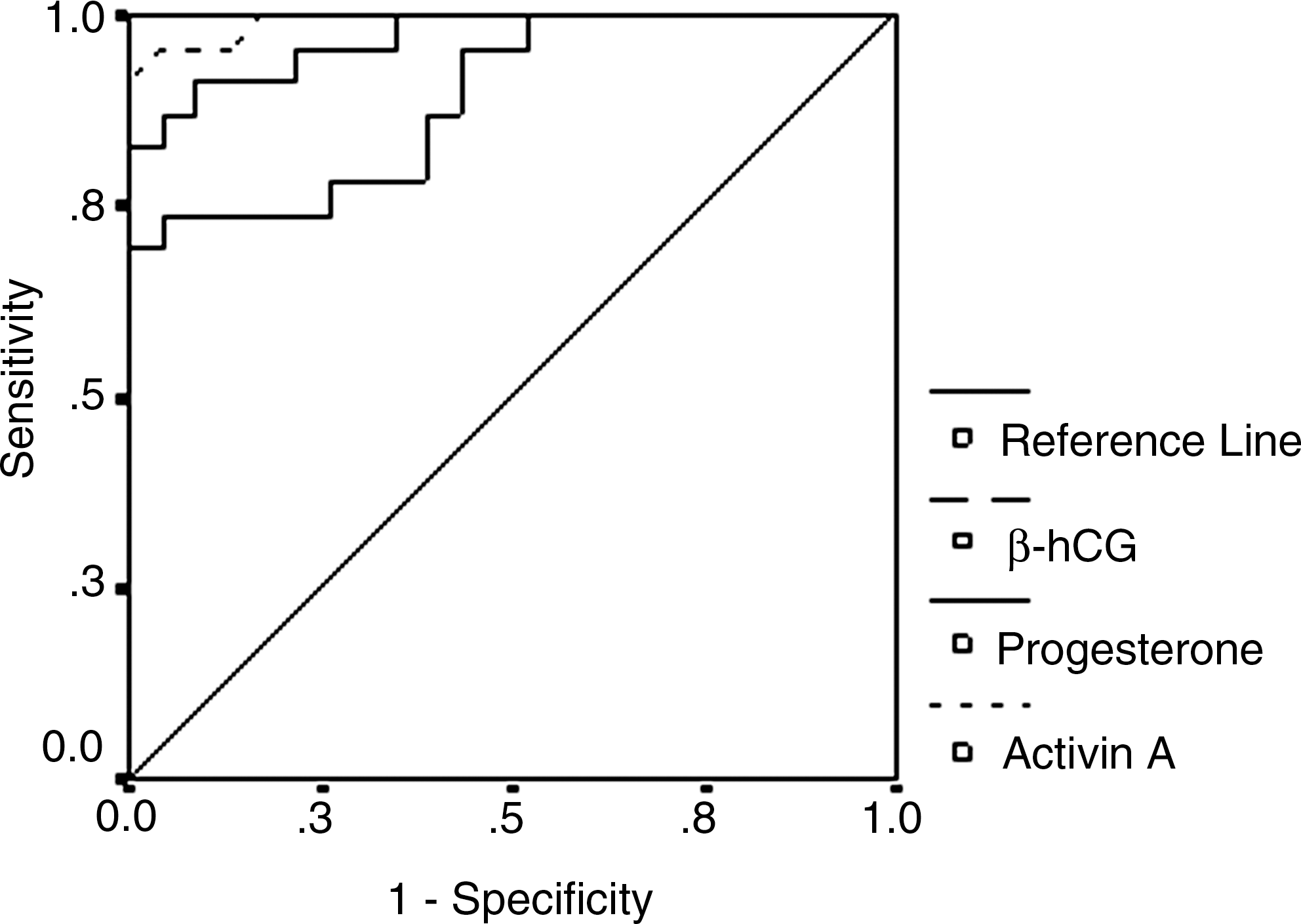
The receiver operator characteristics (ROC) curves for activin A, β-human chorionic gonadotropin (β-hCG), and progesterone.
Student's t test.
Mann-Whitney U test.
Fisher's exact test.
Pearson chi-square test.
Mann-Whitney U test.
β-hCG, β-human chorionic gonadotropin.
Table 3 shows the estimated cutoff, sensitivity, specificity, and positive and negative predictive values for activin A, progesterone, and β-hCG in prediction of normal ongoing pregnancies. No statistically significant relation was found among activin A, β-hCG, and progesterone within both groups. When the entire sample of all subjects is evaluated, however, a statistically significant correlation was found between β-hCG and progesterone, β-hCG and activin A, and progesterone and activin A (p<0.001) (Table 4).
Upper limit of area under the curve (AUC) was >1.
CI, confidence interval; NPV, negative predictive value; PPV, positive predictive value.
Discussion
To date, several biochemical markers have been used to predict the clinical course of early pregnancies. 2 –7 Although much of the work on the prediction of outcome of early pregnancies conceived via IVF has centered on the use of serum β-hCG and progesterone levels, some other markers have been studied. In the last decade, a dimeric placental glycoprotein, activin A, has been used widely as a marker. Serum levels of activin A are higher than those in nongravid patients and increase as the pregnancy progresses. 8,9 Activin A modulates placental hormonogenesis, 13 uterotonin secretion, 14,15 and cytotrophoblast proliferation and differentiation. 16 The present study investigated whether activin A can be used as a marker for prediction of the prognosis in early pregnancies conceived using IVF. In addition, progesterone/activin A and β-hCG/activin A ratios are evaluated.
When demographic characteristics of the study population were evaluated, the mean maternal age of the normal ongoing pregnancy group was found to be statistically lower than that of women with biochemical pregnancies. This finding coincides with the fact that younger age is associated with higher success rate of ART. 17 Hull et al. 18 also stated that embryo implanting ability and survival decline gradually after 30 years of age. Condous et al. 4 tested three multicategorical logistic regression models for predicting the outcome of pregnancies of unknown localization. They indicated that the model, which was based on patient's age, was the best model among the other two models, which were based on β-hCG ratio (rate of change in β-hCG over 48 hours) and average progesterone level (the mean of the progesterone level at 0 and 48 hours). In a normal pregnancy, serum β-hCG concentrations increase at least 66% in 48 hours up to 10,000 mIU/mL. In contrast to normal pregnancies, serum β-hCG levels are lower or increase slowly in cases of miscarriages or ectopic pregnancies. 19,20 As expected, we found serum β-hCG concentrations to be significantly higher in normal ongoing pregnancies compared to biochemical pregnancies. It has been reported previously that β-hCG levels were significantly lower in abnormal pregnancies compared to normal ongoing pregnancies. 21
Because serum progesterone levels occur within a wide spectrum, the diagnostic value of progesterone is limited. However, serum progesterone levels of abortive pregnancies are usually lower than those of viable intrauterine pregnancies. 22 Also, it has been reported that a single serum progesterone measurement could be a useful predictor of pregnancy outcome in women undergoing IVF or ICSI treatment. 1 The findings of the present study are compatible with the fact that progesterone levels of normal ongoing pregnancies are significantly higher than those of biochemical pregnancies. Moreover, the present study has revealed significant statistically relevant correlations between β-hCG and progesterone, β-hCG and activin A, and progesterone and activin A. Ioannidis et al. 1 evaluated the association between the day 14 level of progesterone and pregnancy outcome. When 32.3 ng/mL is determined as the cutoff point for progesterone in prediction of viable pregnancies, the sensitivity and specificity were computed to be 88.2% and 84%, respectively. In the present study, a sensitivity of 69.6% and a specificity of 100% were found for prediction of normal ongoing pregnancies with 40.58 ng/mL as the cutoff point for progesterone. Thus, a single serum progesterone measurement is considered to be an effective way of predicting pregnancy outcome in women treated by IVF-ICSI treatment.
Our data suggest that a single measurement of activin A can be used as a marker for the progress and outcome of early pregnancies conceived via IVF. Progesterone/activin A and β-hCG/activin A ratios may also be used as markers. Luisi et al. 23 compared the serum activin A and inhibin A levels of 65 women who had a live birth with those of 54 women who had an abortion (38 incomplete and 16 complete) between 5 and 12 weeks of gestation. Although their results indicated that inhibin A measurement is more sensitive than activin A determinations in signaling first trimester pregnancy problems, activin A levels were found to be significantly lower in women who had complete abortion compared with the healthy control group. Prakash et al. 24 detected serum concentrations of activin A to be lower in pregnancies resulting in abortion when compared with normal pregnancies. They concluded that activin A may be used as a marker to predict pregnancies that are likely to miscarry. In contrast, Wallace et al. 25 compared 98 miscarriages between 6 and 13 weeks of gestation with a total of 198 normal singleton pregnancies and showed that serum concentrations of activin A were statistically similar in both groups. Their results suggested that activin A levels may not be as useful in predicting the outcome of early pregnancies. Kirk et al. 26 evaluated the role of serum activin A in prediction of the outcome of women with failing pregnancies of unknown location, intrauterine pregnancies, and ectopic pregnancies. They found activin A levels were not significantly different among the three outcome groups and reported that serum activin A levels are not helpful in predicting the outcome of pregnancies of unknown localization.
These controversial results may be attributed to the design and sample size of the studies. Despite the varying opinions in the literature, the significantly higher serum activin A levels in the normal ongoing pregnancies in the present study suggest that this glycoprotein may play an important role in implantation and early embryo development. The lower concentrations of activin A in biochemical pregnancies suggest that impaired secretion of activin A occurs in the presence of problems related to trophoblast invasion and implantation. In any case, in the presence of implantation failure, a condition associated with trophoblast dismission, maternal serum levels of activin A are lower compared to those in normal ongoing pregnancies, indicating the failed trophoblast. The prospective design of the present study may provide advantages.
The normal ongoing and biochemical pregnancies were found to be statistically similar in estradiol level at hCG administration day, the number of IVF trials, and the number of oocytes retrieved and embryos transferred. This similarity provides an advantage for the present study in evaluating the relationship between activin A levels and early pregnancy outcome. Comparisons between normal ongoing and biochemical pregnancies can yield more data about the role of activin A in early gestational progress. However, the small sample in the present study limits its power.
Conclusions
Although the sensitivity and negative predictive value of activin A were calculated to be a little higher than those of β-hCG at the calculated cutoff values, we cannot state that activin A has advantages over β-hCG as a predictor because of the small sample size. Nevertheless, the findings of the present study indicate that a single measurement of activin A can be suggested as a marker for the progress and outcome of early pregnancies conceived via IVF. We have put forward a preliminary study of activin A to determine if the IVF procedure will terminate as a biochemical pregnancy (implantation fail) or the live embryo will successfully implant. However, further large-scale studies will be required to determine the efficacy and reliability of activin A in predicting early pregnancies achieved by ART.
Footnotes
Disclosure Statement
No competing financial interests exist.