
Abstract
Objective:
To assess differences in congenital anomalies, infant mortality, and obstetrical complications as well as risk factors associated with an adverse pregnancy outcome in women with type 1 (T1DM) and type 2 diabetes mellitus (T2DM).
Methods:
This observational study was performed at a university clinic and included a total of 200 singleton pregnancies between January 1995 and December 2006. Outcome measures comprise the prevalence of major congenital malformations, fetal losses, stillbirths, and neonatal deaths as well as the combined end point, adverse pregnancy outcome, and obstetrical complications.
Results:
Despite changes in prevailing risk factors, the rate of congenital anomalies and embryonic as well as perinatal death was comparable in type 1 diabetic women over time as well as between women with T1DM and T2DM. Outcome measures and risk factor profile were similar in women with preconception and newly diagnosed T2DM. Glycemic control and increased body mass index (BMI) during the first trimester were the strongest predictors of an adverse pregnancy outcome. Hemoglobin A1c (HbA1c) was higher in T1DM than in T2DM but similar in women with T1DM over time. BMI was highest in women with T2DM, followed by T1DM women of the most recent time period.
Conclusions:
In addition to HbA1c, other risk factors, especially high BMI, strongly influence pregnancy outcome. The higher prevalence of these risk factors in T2DM might compensate for the better glycemic control, resulting in a pregnancy outcome comparable to that of T1DM. Pregnancy outcome in T1DM remained unchanged over time, possibly because of the missing amelioration of HbA1c levels and the increasing BMI.
Introduction
One of the 5-
The objective of the present study was to assess differences in character and frequency of congenital birth defects, fetal losses, neonatal deaths, and obstetrical complications in women with T1DM or T2DM in January 2001 through December 2006 and to evaluate potential changes in pregnancy outcome of T1DM women after the introduction of standardized operating procedures (SOP; January 1995–December 2000 vs. January 2001–December 2006). Further, we aimed at identifying risk factors associated with an adverse pregnancy outcome.
Material and Methods
The study population included 200 consecutive singleton pregnancies in women with T1DM or T2DM who attended the diabetes outpatient department of the Medical University of Vienna between January 1995 and December 2006. Clinical management of diabetes and hypertension in pregnancy was performed according to international guidelines 12 –14 and included bimonthly visits at the diabetes outpatient department and the obstetrical clinic, with regular monitoring of hemoglobin A1c (HbA1c), weight gain, and blood pressure. According to local standards, nonpregnant diabetic women of childbearing potential were asked about their prospective reproductive plans at each visit. If a desire to become pregnant was stated, folic acid supplementation was introduced, and therapy with oral antihyperglycemic drugs (OADs) was terminated. Women with overt diabetes were advised to use contraceptives until reaching HbA1c levels <7.0% because of the elevated risk of an adverse pregnancy outcome. 12,15 In women with unplanned pregnancy, OADs were terminated and folic acid was started immediately at diagnosis of pregnancy. Although management protocols did not change during the study period of 12 years, pregnancy counseling became more structured in 2001 because of the introduction of SOP. In the context of quality management, these SOP contain written instructions for clinical care of pregnant women with overt diabetes based on international guidelines 14 and resulted in stricter surveillance of pregnancy and interdisciplinary meetings involving diabetologists, obstetricians, and neonatologists.
All subjects were identified using a prospectively compiled name register. Exclusion criteria were multiple pregnancies (n = 3), terminations of pregnancy due to social indications (n = 1), and secondary causes of diabetes (n = 1, cortisone-induced diabetes). 14 Secondary diabetes was excluded because of the low number of cases and scant information about its effect on pregnancy outcome. Data assessment was performed using medical records and covered the last visit within 6 months before conception, the period of pregnancy, and a follow up-period of 14 months after delivery. The study protocol was approved by the Ethics Committee of the Medical University of Vienna (No. EK168/2006).
HbA1c was measured by high-performance liquid chromatography (HPLC) (reference range 4.0%–6.0%). The mean arterial blood pressure (MAP) was calculated as:
Definitions
Classification of diabetes was according to the guidelines of the American Diabetes Association (ADA). 15 In addition, women who met the ADA criteria for overt diabetes 14 at the screening 2-hour, 75-g oral glucose tolerance test (OGTT) early in pregnancy (before gestational week [GW] 20 + 0) and 3 months after delivery and, thus, were likely to have had undiagnosed diabetes before conception 8 –11 were included in the present study. Severe maternal hypoglycemia was defined as hypoglycemia requiring help from another person. Preconception care was assumed if control visits were documented at least biannually and counseling about diabetes-associated risks during pregnancy was provided before conception. In contrast, a pregnancy was considered as being planned if the woman stated her desire before conception to become pregnant and, therefore, attempted to achieve optimal glycemic control (HbA1c≤6.5%).
In women with newly diagnosed diabetes, it was assumed that neither information on the impact of glucose tolerance on perinatal outcome (preconception care) nor optimization of glycemic control (pregnancy planning) had been provided because of the missing diagnosis before gestation. Duration of OAD intake was defined as the period from inception to the cessation of OAD and includes the time of embryogenesis. Congenital malformations were categorized according to the European Surveillance of Congenital Anomalies (EUROCAT) criteria. 16 Early pregnancy loss was defined as fetal loss before GW 12 + 0, stillbirth as fetal loss between GW 20 + 0 and delivery, and neonatal death as death within 28 days of birth. Fetal losses before GW 20 + 0 were included only when clinically significant and followed by curettage; that is, pregnancies diagnosed only biochemically, with spontaneous loss of the embryo and without obstetrical intervention, were excluded. 17 As composite outcome parameters, fatal outcome was defined as fetal loss <GW 20 + 0, stillbirth, or neonatal death, and adverse pregnancy outcome was defined as fatal outcome or presence of major congenital malformations. Birth weight below the 10th or above the 90th percentile, both adjusted for age and gender of the Austrian population, was defined as being small-for-gestational-age (SGA) or large-for-gestational-age (LGA), respectively. Neonatal jaundice was defined as hyperbilirubinemia requiring phototherapy, and neonatal hypoglycemia was defined as glucose levels <30 mg/dL (<1.67 mmol/L).
Statistical analysis
Categorical variables were analyzed using Fisher's exact test or Pearson chi-square test as appropriate. For continuous variables, mean values were calculated for every trimester and for the first 14 months after delivery. Comparison between groups was performed using one-way analysis of variance (ANOVA), followed by Tukey's studentized range test (HSD). Pearson's correlation coefficient was determined to evaluate the association between continuous variables. Odd ratios (OR) with 95% confidence intervals (CI) were calculated by multiple logistic regression analyses for adverse pregnancy outcome, fatal outcome, and major congenital malformations as dependent variables. The independent variables were selected based on the level of significance in the univariate analysis. Statistical analysis was performed using SAS Enterprise Guide 4.1 (SAS Institute Inc., Cary, NC). Data are expressed as mean ± standard deviation (SD) or n(%) unless otherwise indicated. p ≤ 0.05 was considered significant.
Results
Risk factor profile
According to White's classification, the distribution of subjects with T2DM and T1DM of the old and the new cohort were as follows: class B, 40.68%, 34.67%, and 93.55%; class C, 33.90%, 42.67%, and 4.84%; class D, 25.42%, 22.67%, and 1.61%; class F, 16.13%, 25.0%, and 29.17%; class R, 0.0%, 1.54%, and 0.0%; class RF, 0.0%, 1.54%, and 0.0%.
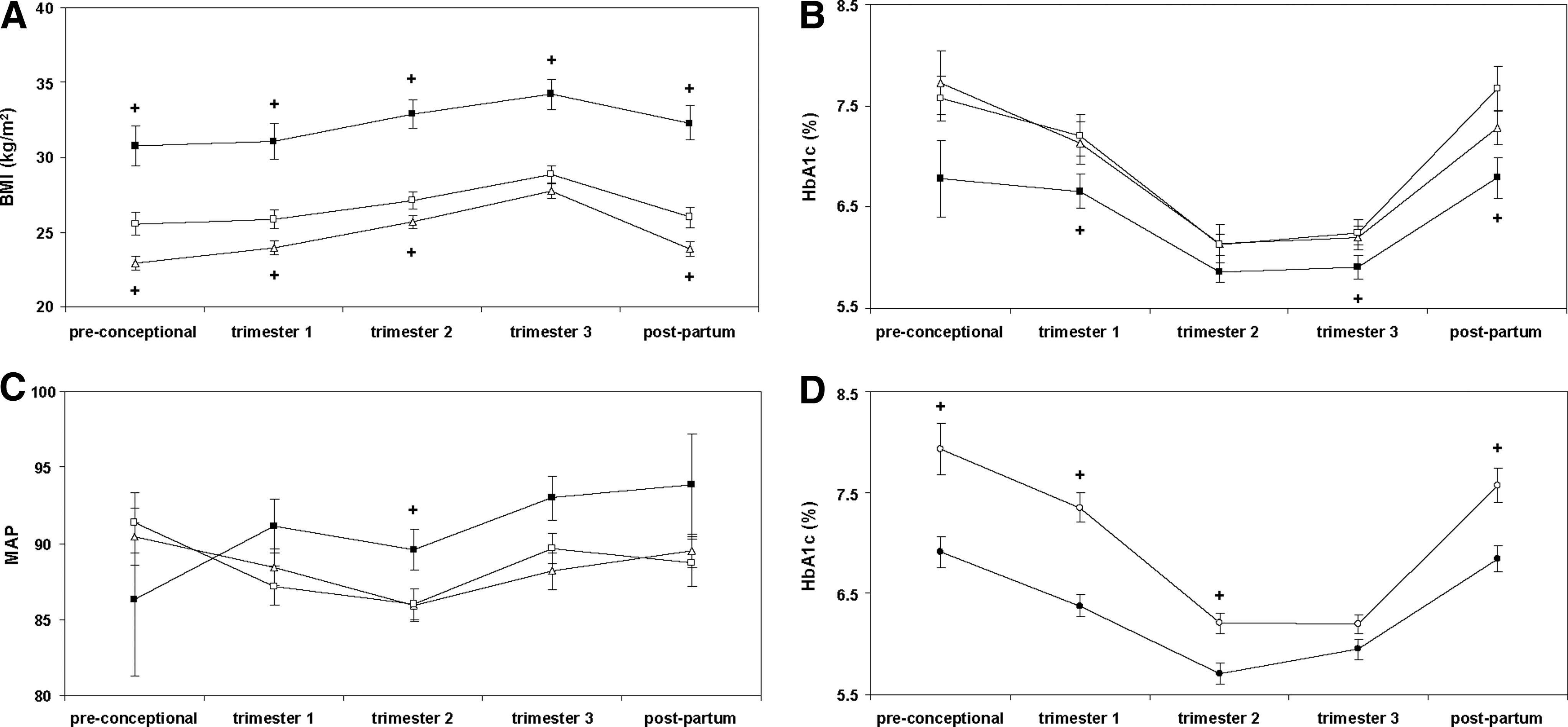
T2DM subjects showed distinct differences in baseline characteristics at admission (Table 1), as well as in HbA1c, body mass index (BMI), and MAP throughout pregnancy (Fig. 1A, B, C), compared to women with T1DM during the same period. Further, a tendency toward lower preconception HbA1c levels (p = 0.059) and higher MAP during the first (p = 0.067) and third trimesters (p = 0.061) was observed in T2DM subjects. No differences in baseline characteristics (Table 1) or BMI, HbA1c, and MAP throughout pregnancy were observed between women with newly and preconception diagnosed T2DM (data not shown), apart from HbA1c levels during the second trimester (6.24 ± 0.91 vs. 5.75 ± 0.71, p = 0.045).
NA, not available; SD, standard deviation; T1DM, type 1 diabetes; T2DM, type 2 diabetes.
In women with T1DM, BMI was significantly higher in the most recent time period (Table 1 and Fig. 1A), whereas no improvement in glycemic control (Fig. 1B) or MAP (Fig. 1C) was observed.
There were no differences in the three cohorts with regard to previous abortions (p > 0.05, respectively). In women who reported smoking during pregnancy (Table 1), the number of cigarettes per day was similar in the three groups (T1DM 1995–2000: median 10, range 0–24; T1DM 2001–2006: median 6.5, range 0–17.5; T2DM 2001–2006; median 10, range 0–38.5).
Women who planned their pregnancies (Table 1) received folic acid supplementation (83.1% vs. 55.4%, p < 0.0001) as well as in vitro fertilization (IVF) (13.3% vs. 3.7%, p = 0.024) more frequently and displayed lower HbA1c values (Fig. 1D) but no differences in BMI or MAP throughout pregnancy (data not shown). The percentage of women with HbA1c>7.0% at admission was significantly higher among women who did not plan their pregnancy (55.6% vs. 38.6%, p = 0.04).
Pregnancy outcome
Of 200 pregnancies, 168 resulted in the birth of a liveborn infant. Terminations of pregnancy had to be performed because of major congenital malformations (n = 1) or high HbA1c at admission (n = 2, 11.7% and 15.9%). Of 11 fetuses with major congenital anomalies, death occured in utero (n = 1), a few days after delivery (n = 1), or after termination of the pregnancy (n = 1). Fetal loss was observed in 8 women with IVF (<GW 12 + 0: n = 5; GW 12–20: n = 2, GW 29: n = 1). The rate of pregnancy loss < GW 20 + 0 was comparable to that reported previously for a western background population. 18,19 Infantile outcome parameters, oligohydramnios, polyhydramnios, and the rate of elective sections and of instrumental deliveries (p > 0.05, respectively) were similar in the three groups (Table 2). Hypothyroidism tended to be more frequent in the old T1DM cohort than in new T1DM cohort (p = 0.055), whereas no differences were observed between T1DM and T2DM women during the same period.
GW, gestational week; NICU, neonatal intensive care unit.
Women with T1DM experienced significantly more episodes of severe hypoglycemia (0.49 ± 1.35 vs. 0.00 ± 0.00 episodes, p = 0.004) than T2DM women during the same period, whereas no differences were observed between the two T1DM cohorts (0.49 ± 1.35 vs. 0.30 ± 0.74, p = 0.33). Birth weight ≥4000 g was positively associated with maternal BMI at admission (29.96 ± 5.84 vs. 26.53 ± 6.00, p = 0.01) and tended to be lowest in the new T1DM cohort (Table 2). In T2DM women, birth weight ≥4000 g tended to be higher in offspring of women with newly as compared with preconception diagnosed T2DM, whereas no differences were observed in any other outcome parameter (Table 2). Offspring of women with T2DM suffered hypoglycemic episodes right after delivery less frequently than neonates born to T1DM mothers (8.9% vs. 23.6%, p = 0.042). Planning of pregnancy did not improve perinatal outcome, including major congenital malformations, fatal outcome, or adverse pregnancy outcome (Table 3).
OAD, oral antihyperglycemic drugs.
In the univariate analysis, pregnancy outcome was significantly associated with glycemic control, folic acid supplementation, IVF, and MAP (Table 3). Multiple logistic regression analysis identified IVF (OR 0.07, 95% CI 0.01-0.41), HbA1c (OR 0.41, 95% CI 0.26-0.64), and BMI (OR 0.90, 95% CI 0.83-0.98) during the first trimester but not folic acid supplementation or MAP during the first trimester as independent predictors of an adverse pregnancy outcome. HbA1c (OR 0.38, 95% CI 0.22-0.64) and BMI (OR 0.85, 95% CI 0.76-0.94) during the first trimester as well as diabetes duration (OR 0.92, 95% CI 0.86-0.99) and IVF (OR 0.03, 95% CI 0.003-0.269) remained predictive for a fatal outcome but not MAP during the first trimester, folic acid intake, or cigarette smoking. Finally, only HbA1c during the first trimester (OR 0.48, 95% CI 0.25-0.91) but not smoking habits, BMI, or MAP during the first trimester was a predictor of major congenital malformations.
Discussion
The present study shows that apart from prolonged neonatal hypoglycemia, the pregnancy outcome of type 1 diabetic women did not improve significantly after the introduction of SOP during the last decade and that T2DM is associated with a risk for congenital malformations and stillbirths comparable to that of T1DM. Of note, the pregnancy outcome in women with preconception and newly diagnosed T2DM was similar, although the latter demonstrated an insignificant trend toward a higher rate of birth weight ≥4000 g in a small sample of subjects.
Strength and limitations
A strength of our study is that it presents Central European data collected by a single tertiary care center over a long period of time. Furthermore, it includes pregnancies of women with newly diagnosed T2DM. This appears to be of great relevance, as clinical experience has shown that these women have an elevated or at least equal risk for an adverse pregnancy outcome compared with those with T2DM diagnosed before conception. Limitations of this study are the small sample size of 200 women and, consequently, the limited power, the descriptive nature, and that some evaluated parameters are solely based on self-reported information by the patients, for example, smoking and drinking habits and severe hypoglycemia.
Determinants of pregnancy outcome
Glycemic control, as evaluated by HbA1c levels, was shown to be the best predictor for an adverse pregnancy outcome in women with overt diabetes. 5 Consistently elevated periconception HbA1c levels in our study were associated with both a fatal outcome and the presence of major congenital malformations. The significantly increased prevalence of an adverse pregnancy outcome in subjects with HbA1c >7.0% at admission is consistent with previous results. 5 In addition to glycemic control, we found fatal outcome to relate to other risk factors, including high BMI and prolonged diabetes duration. The latter, which is associated with diabetic microangiopathy, affects placental circulation via alterations in vascular reactivity 20 and, consequently, might also negatively influence pregnancy outcome. Further, our data indicate that missing folic acid supplementation might promote an attenuated rate of liveborn infants. This suggestion is corroborated by George et al., who found low folate levels not only to relate to congenital malformations as was shown previously 21 but also to spontaneous abortions. 22,23 Furthermore, our data support previous findings of a potentially teratogenic effect of smoking. 24 In the univariate analysis, MAP throughout pregnancy but not hypertension or preeclampsia was predictive of the presence of birth defects in our study collective. This implies that subjects with borderline hypertension who are not treated or insufficiently treated are at increased risk to deliver a child with congenital malformations, suggesting that these patients may benefit from a stricter surveillance and that achieving lower blood pressure targets might be necessary.
Our results, although limited by small sample size, indicate that OADs might negatively influence pregnancy outcome. The majority of studies 25 –28 show no differences in perinatal mortality and the rate of congenital anomalies; still, the literature remains inconclusive about the impact of OADs during pregnancy. 29 –31 Scant evidence has been provided to date about the effects of OADs during fetal organogenesis in women with overt diabetes, with most of the studies having been performed in women with either polycystic ovaries syndrome (PCOS) or GDM. 26 –28 Thus, OADs are currently not indicated for the treatment of glucose intolerance during pregnancy in Austria and many other European countries.
In contrast to other studies, 2 –4 planning of pregnancy irrespective of the diabetes type, time period, or glycemic control did not result in an improved pregnancy outcome in the total study population (Table 3), although these women had significantly lower periconception HbA1c levels and a higher rate of folic acid supplementation. The reason for this observation is unknown but might be partly attributable to the high number of women who wanted to plan their pregnancy but became pregnant before glycemic control could be optimized (Table 1). Thus, it is important to emphasize the need of contraception until HbA1c ≤7.0% when pregnancy is desired.
Pregnancy outcome in T1DM vs. T2DM in 2001–2006
Previously, it was suggested that T2DM confers a higher risk for stillbirths and birth defects than T1DM. 4 Differences in character and frequency of risk factors for an adverse pregnancy outcome might reflect a social disadvantage of many pregnant women with T2DM 2,32 and compensate for their better glycemic control. In our study, T2DM subjects were characterized by a more advanced maternal and gestational age at admission, 33 higher prepregnancy BMI, 34 increased MAP, lower folic acid intake, 21,22 less frequent planning of pregnancy, and a higher prevalence of language barriers but better glycemic control than women with T1DM.
A major issue in this context is the considerable rate of undiagnosed T2DM, accounting for approximately 25% in our study population, which is similar to that in previous reports. 8 Undiagnosed T2DM has been suggested to be of particular danger for fetal viability because of the hazard of first-trimester hyperglycemia on fetal organogenesis. 8 –11 Consistently, there is increasing evidence that preconception undiagnosed diabetes has the same rate of birth defects and perinatal mortality as T1DM and T2DM. 8 –11 Our own results corroborate these findings and have shown no differences in baseline characteristics and, in part, an even worse pregnancy outcome in newly diagnosed as compared to preconception T2DM. Nonetheless, the current GDM definition 35 does not differentiate between preconception undiagnosed T2DM and GDM, which usually becomes evident after GW 24 and which confers a lower risk for an adverse pregnancy outcome. 11,36,37 Omori and Jovanovic 11 recently proposed to reconsider the current definition of GDM and to return to the prior definition of O'Sullivan describing GDM as “a transient abnormality of glucose tolerance during pregnancy.” 38 Our data support suggestions for the implementation of a novel GDM definition considering hyperglycemia and increased HbA1c levels early in pregnancy as “diabetes diagnosed during pregnancy.”
In our study, women with T2DM experienced significantly less hypoglycemic episodes. This observation is consistent with previous reports and might be attributable to the higher insulin resistance. 4 Interestingly, we found a markedly lower rate of severe hypoglycemia in T1DM women compared to rates Scandinavian studies, 39 indicating that differences in glycemic goals and, subsequently, in the tolerability of severe hypoglycemic episodes are applied in the respective institutions. Offspring of T2DM mothers had fewer hypoglycemic episodes after delivery. This might be explained by the better glycemic control of T2DM women during the first and last trimesters, resulting in lower fetal hyperinsulinemia. Maternal hyperglycemia and subsequent fetal hyperinsulinemia, however, also represent an important causal factor for excessive fetal growth. 40 In our study, collective birth weight ≥4000 g tended to be more frequent among neonates born to T2DM mothers.
Evidence was found that high maternal BMI before conception as well as excessive weight gain during pregnancy promote a fetal growth spurt, resulting in an increased birth weight. 41,42 Consistently, women with T2DM in our study population were more obese and BMI at admission correlated positively with the rate of birth weight ≥4000 g. Taken together, these findings indicate that the impact of high maternal prepregnancy BMI might be greater than that of maternal hyperglycemia on infantile birth weight. 41,42
Pregnancy outcome in T1DM during 1995–2000 vs. 2001–2006
Consistent with studies from France 3,43 and Northern Ireland, 44 our data showed no improvement in the rate of congenital birth defects or perinatal death in T1DM women over time. However, the frequency of neonatal hypoglycemia within the first 24 hours after delivery and the rate of birth weight ≥4000 g decreased, although not statistically significantly. Causal factors for the constant rate of adverse pregnancy outcomes were not found in the present study but might involve the missing amelioration of glycemic control or the observed changes in the risk factor profile. Increased BMI, which has emerged as a prevalent risk factor in women with T1DM in our study collective, has been shown to be independently associated with an adverse pregnancy outcome. 34 It might be hypothesized that the additional promotion of pregnancy-induced insulin resistance by obesity might, in part, account for the continuously poor pregnancy outcome of T1DM women.
Although the percentage of planned pregnancies remained unchanged over time and despite the introduction of SOP containing prepregnancy management protocols, more women with planned pregnancies had HbA1c ≥7.5% at admission in the most recent period (Table 1). This finding corroborates the need for contraceptives until target HbA1c values are achieved, as adverse pregnancy outcome rates increase markedly with worse glycemic control.
Conclusions
In addition to HbA1c, other risk factors, especially high BMI, strongly influence pregnancy outcome. The higher prevalence of these risk factors in T2DM might compensate for the better glycemic control, resulting in a pregnancy outcome comparable to that of T1DM. The rates of fatal outcome and congenital birth defects in T1DM remained unchanged over time, possibly because of the lack of amelioration of HbA1c levels and the increasing BMI.
Footnotes
Acknowledgments
We thank Mrs. K. Hang and Mrs. M. Hatschka for helping with logistics. The study was supported in part by the Medical Scientific Fund of the Mayor of Vienna (No. 09063) to A.K.-W.
Disclosure Statement
The authors have no conflicts of interest to report.