
Abstract
Background:
Increasing cardiovascular fitness through exercise participation among sedentary people is important for decreasing all-cause mortality. From an intervention perspective, identifying modifiable factors that maximize the successful initiation of exercise is of utmost importance. For women, cyclic hormonal variations can influence aspects of health and health behaviors, from smoking cessation efficacy to physiological responses to exercise. The purpose of this study was to examine the influence of menstrual cycle phase and hormonal contraceptive (HC) use on subjective response to an initial bout of moderate intensity exercise among previously sedentary women (n = 117).
Methods:
Women completed a treadmill exercise challenge session at 65% of their previously determined maximum oxygen consumption (V
Results:
There was a significant menstrual phase × birth control interaction on change in RPE [F(2, 111) = 3.75, p < 0.05] and change in perceived pain [F(2, 110) = 3.31, p < 0.05]. Women in the early follicular phase who were not using HCs had significantly greater increases in RPE and increases in pain compared with women in the late follicular and luteal phases.
Conclusions:
Our results indicate that the use of HC and cycle phase influence sedentary women's subjective response to exercise. These results have important implications for the timing of exercise interventions aimed at increasing exercise among sedentary women.
Introduction
Cardiovascular fitness is consistently and significantly inversely related to cardiovascular events as well as all-cause mortality in men and women. 1 Exercise has undeniable physiological and mental health benefits, 2,3 but these benefits are far removed from the behavior required to attain them. The long-term health risks of physical inactivity are startling; however, knowing about these risks is, as with many health behaviors, inadequate motivation to change sedentary behavior. Understanding the more proximate mechanisms that lead to initiation and maintenance of exercise is therefore crucial to designing more effective intervention programs. Although some of these factors may not be modifiable, identifying those that are will allow us to target those variables in designing interventions and thereby maximize the likelihood that an individual has a more positive experience when initiating an exercise program.
There is evidence that the hormone fluctuations that characterize the female menstrual cycle indirectly affect other domains of health and health behaviors. Cyclic variation is shown to influence migraines, epilepsy, rheumatoid arthritis, irritable bowel syndrome, and even glycemic control in diabetic women. 4 Researchers have found that women trying to quit smoking have greater withdrawal symptoms during the luteal phase of their cycle. 5,6 In a smoking cessation intervention, women who quit smoking during the luteal phase were twice as likely to have relapsed at 9 weeks compared with women who quit during the follicular phase. 7 Given that physical inactivity is second only to smoking as a modifiable lifestyle risk factor that causes morbidity and mortality, 8 understanding the influence of menstrual cycle on exercise behavior may provide insight into a crucial area of women's health. Furthermore, evidence has shown that aspects of physiological response to exercise, such as thermoregulation, ventilation, and cardiovascular strain, are influenced by hormonal fluctuations across the cycle. 9 –12 These fluctuations may also be associated with differences in psychological or subjective responses to physical activity (e.g., perceived exertion and pain) across the cycle. From a health promotion perspective, a more positive psychological response to exercise is an important proximate mechanism that can lead to the initiation and maintenance of exercise. 13
A comprehensive review of the extant literature on reproductive hormones and the physiological response to exercise is beyond the scope of this article (see references 11 and 12). In general, although several studies report increases in heart rate (HR) and cardiovascular strain and decreases in thermoregulation during the midluteal phase compared to the midfollicular phase, a consensus on changes in athletic performance across the cycle remains elusive.
Even less is known about the influence of hormonal fluctuations on the more subjective or psychological response to exercise, particularly in sedentary women. Although Pivarnik et al. 14 reported higher ratings of perceived exertion (RPE) during the luteal compared to the midfollicular phase, when both progesterone and estrogen are high, participants in another study had greater RPE during the ovulatory phase (days 14–16) compared to the midfollicular (days 7–8) and midluteal (days 22–23), when only estradiol is high. 13 Other studies have found no conclusive evidence for changes in RPE across the cycle. 9,10,15 –17 The inconclusive findings could be a result of the use of small samples of highly active women (typically 8–10 women), which are limited in their power to detect psychological effects. Only one study used a sample of “low to moderately” trained participants, but this study still had only 9 particpants. 18 Further, although RPE is theoretically and empirically linked to HR among active individuals, sedentary and low-fit individuals have been shown to perceive greater exertion than HR measures indicate. 19,20 If RPE is indeed more indicative of the psychological response to exercise than physiological variables, larger sample sizes will be necessary to detect meaningful differences in psychological response across the cycle. In addition, using only active samples to examine menstrual cycle differences is problematic because active women often have reduced hormone fluctuations across the cycle, even when eumenorrheic. 21 Thus, they may not experience the same physiological or psychological responses to exercise as those who are new to physical activity. For example, Schoene et al. 12 found that both trained and untrained women had increased respiratory drive in the midluteal compared to midfollicular phase, but this increase was significantly greater in untrained women. Untrained women also had significantly better exercise performance in the midfollicular phase compared to the midluteal phase, with no differences in performance between menstrual phases in eumenorrheic athletes. No differences in any of the variables were observed between the two exercise sessions among amenorrheic athletes, suggesting a key role of hormonal fluctuations and a protective effect of training. Furthermore, cyclic fluctuations in other psychological variables, such as mood, pain, and concentration, are attenuated by sustained exercise participation. 22,23
Perceived pain in response to exercise across the menstrual cycle has, to our knowledge, only been examined in two recent studies. The first found no differences in exercise-induced analgesia between the follicular (5–7 days postmenses) and luteal (6–8 days postovulation) phases, with both groups experiencing increased pain threshold and decreased pain ratings directly after isometric exercise. 24 In another recent study, women experiencing dysmenorrhea during the early follicular phase had decreased exercise performance compared to the midfollicular phase. 25 Outside the context of exercise, women seem to have increased clinical and experimental pain during the late luteal and early follicular phases, associated with declining or low levels of estrogen and progesterone, 26 although the precise hormonal cause has not been elucidated. Estrogen is known to modulate pain in women, ameliorating some types of pain (e.g., migraines, arthritis) but exacerbating others. 27 Hellström and Anderberg 28 demonstrated that women with chronic pain experience more pain during the menstrual phase when hormone levels are low, supporting the hypothesis that estrogen may have a protective effect on chronic pain. Further, when pain is induced experimentally in healthy subjects, a lower pain threshold has been found in women during the early follicular phase compared to the luteal phase. 26,29,30 However, Choi et al. 31 reported higher ratings of pain in the luteal compared to the follicular phase.
The use of various forms of hormonal contraceptives (HCs) is also important to consider. 10 The influence of HCs on physiological response to exercise remains unclear, but their use has shown benefits for exercisers in reducing dysmenorrhea and premenstrual syndrome (PMS) and increasing cycle regularity and control and is postulated to protect bone density. 10 In one study, Nicolay et al. 32 found significantly lower grip strength endurance during the luteal phase among women who were not using HCs but no difference among women who were using HCs. HCs also appear to minimize cyclical changes in psychological variables across the menstrual cycle, with women using HCs reporting less variability in mood and affect throughout the cycle, 33 although contrary results have also been reported. 34 We therefore included a sample of women who were using HCs to serve as a control group.
The current study aimed to extend previous research on cyclical variation in responses to exercise by focusing on intervention-relevant outcomes in three ways. First, we directly measured psychological responses to exercise, as a positive psychological response to exercise is important for the successful initiation of exercise. Second, we measured perceived exertion and pain during exercise among currently sedentary women—the appropriate target population for exercise interventions—during an initial bout of laboratory-controlled, moderate intensity exercise. Finally, we included women using HCs as a control group in order to compare the effect of cycle phase on exercise response between the naturally cycling and HC groups. We hypothesized that increases in perceived exertion and pain during exercise would differ between cycle phases among women not using HCs but that these differences would not be observed among the control group. Specifically, given the mixed findings in previous studies, we tentatively hypothesized that women in the luteal phase (not using HCs) would report greater increases in exertion. Finally, based on the evidence that estrogen may have a protective effect on pain, we hypothesized that increases in ratings of pain would be highest among women in the early follicular phase.
Materials and Methods
The data were collected as part of a randomized controlled trial (RCT) of an exercise promotion intervention. 35 All data presented in this article were collected before randomization and, thus, are unaffected by condition assignment in the larger trial.
Participants and recruitment
Participants in the full trial were nonactive but otherwise healthy men and women between the ages of 18 and 45. All participants were recruited from the Denver metro area and the University of Colorado community. Participants were primarily recruited through electronic ads placed on campus bulletins, Craig's list, Facebook, and flyers posted at various locations. Individuals were excluded if they smoked, were on a restricted diet, were taking psychotropic medications, were receiving treatment for any psychiatric disorder, were diabetic, had a history of cardiovascular or respiratory disease, had an illness in the previous month, or were pregnant. During the recruitment process, nonactive was defined as engaging in <90 minutes of voluntary moderate intensity physical activity per week for the past 3 months. All participants were required to have a body mass index (BMI, kg/m2) between 18 and 37.5, be physically capable of moderate intensity physical activity, pass an eligibility evaluation by a study physician, be willing to be randomly chosen for one of the two interventions (exercise or health and wellness), and have a regular menstrual cycle (if female). All participants gave informed consent. A total of 238 individuals (189 female and 49 male) completed an initial fitness assessment (maximum oxygen consumption [V
From the sample of women who completed the exercise session (n = 189), we included all who provided the onset of their previous menstrual cycle (76%). We estimated the cycle phase of the women by conservatively dividing the menstrual cycle into three phases using published procedures 36 –41 : early follicular (i.e., menses: days 1–5), late follicular (days 9–15), and luteal (days 18–34). All women in days 6, 7, 8, 16, or 17 or who had > 35 days since their last menstrual period were excluded from analyses. This yielded a sample of n = 117 women. Of this sample, 73 (62%) were not using any hormonal birth control, and the remaining 44 (38%) served as controls. Although it is not technically correct to refer to phases of the cycle as follicular and luteal among our control group, for clarity and consistency, we refer to days 9–15 and 18–34 as the late follicular and luteal phases, respectively, for both groups. Means and standard deviations (SD) for the primary demographic study variables are shown in Table 1. Examinations of skew and kurtosis for all continuous variables revealed no problematic deviations from normality. The groups using and not using HCs did not significantly differ on BMI, activity level, race, or cycle phase. There was a significant difference in mean age between the groups. Controlling for age in the analyses did not alter the significance of the results; therefore, we present the results not controlling for age for parsimony.
BMI, body mass index; HC, hormonal contraceptive; SD, standard deviation.
Measures assessed at baseline prior to activity
Body composition and demographics
BMI was computed using a ratio of measured body mass (kg) to height squared (m2). Self-reported age and ethnicity were also collected. Women were presented with a calendar and asked to report the date of onset of their most recent period. From this, we used a forward method to calculate their menstrual cycle day on the day of the challenge session.
Physical activity
Overall physical activity per week was measured using the interviewer-administered Stanford Seven-Day Physical Activity Recall 42,43 to calculate minutes of voluntary physical activity of at least moderate intensity (min/week).
Procedures
In an initial session, cardiorespiratory fitness was assessed by measuring V
Approximately 1 week after the fitness session, participants completed a submaximal exercise session consisting of a 30-minute bout of physical activity on the treadmill at 65% of their previously estimated V
Measures assessed during submaximal exercise
A number of measures were taken at three time points during the submaximal exercise session: 10, 20, and 30 minutes into the activity. Borg's RPE 46 was used to assess subjective exertion. It is a single-item, 15-point subjective measure of exertion ranging from 6 to 20. It has adequate reliability and validity 47 and is used frequently in laboratory studies of exercise. 13 Participants estimated perceived pain using a one-item, 12-point Borg CR10 scale 46 ranging from 0=no pain to 10=extremely intense (almost unbearable) pain, with gradual intermediate verbal cues at 0.5=very faint pain, 1=weak pain, 2=mild pain, 3=moderate pain, 4=somewhat strong pain, 5=strong pain, and 7=very strong pain.
Analysis plan
Random coefficient regression (RCR) was used to model within-subject linear changes in RPE and pain during exercise (SAS version 9.2, Cary, NC) and to determine if there was variability in those linear changes. By treating time as both a fixed and a random effect, RCR gives results about the average change over time as well as the degree to which there is variability between participants in changes in a particular variable over time.
Within-subject slopes for linear time trends in each of the in-task variables were calculated for each participant and used as dependent variables. We examined the slope rather than mean because we aimed to assess the relationship of menstrual phase to individual responses to exercise, and the slope represents a response in terms of individual change over time during the bout. To test between-group effects, we conducted two 3 (cycle phase: early follicular, late follicular, or luteal) × 2 (birth control: yes or no) analyses of variance (ANOVA). Simple effects were tested for significant interactions. Finally, as we did not validate cycle phase with hormonal or body temperature measures to conclusively distinguish between the late follicular and luteal phases, we also compared the between-groups effects with the more confidently verifiable cycle differences by conducting 2 (cycle phase: early follicular/menses or nonmenses) × 2 (birth control: yes or no) ANOVAs.
Results
Descriptive statistics on ratings of perceived exertion and pain
Ratings of RPE and pain averaged across the time points by cycle phase and HC use are shown in Table 2. Changes in mean RPE and pain across time by cycle phase for non-HC users and controls are illustrated in Figures 1 (RPE) and 2 (pain).
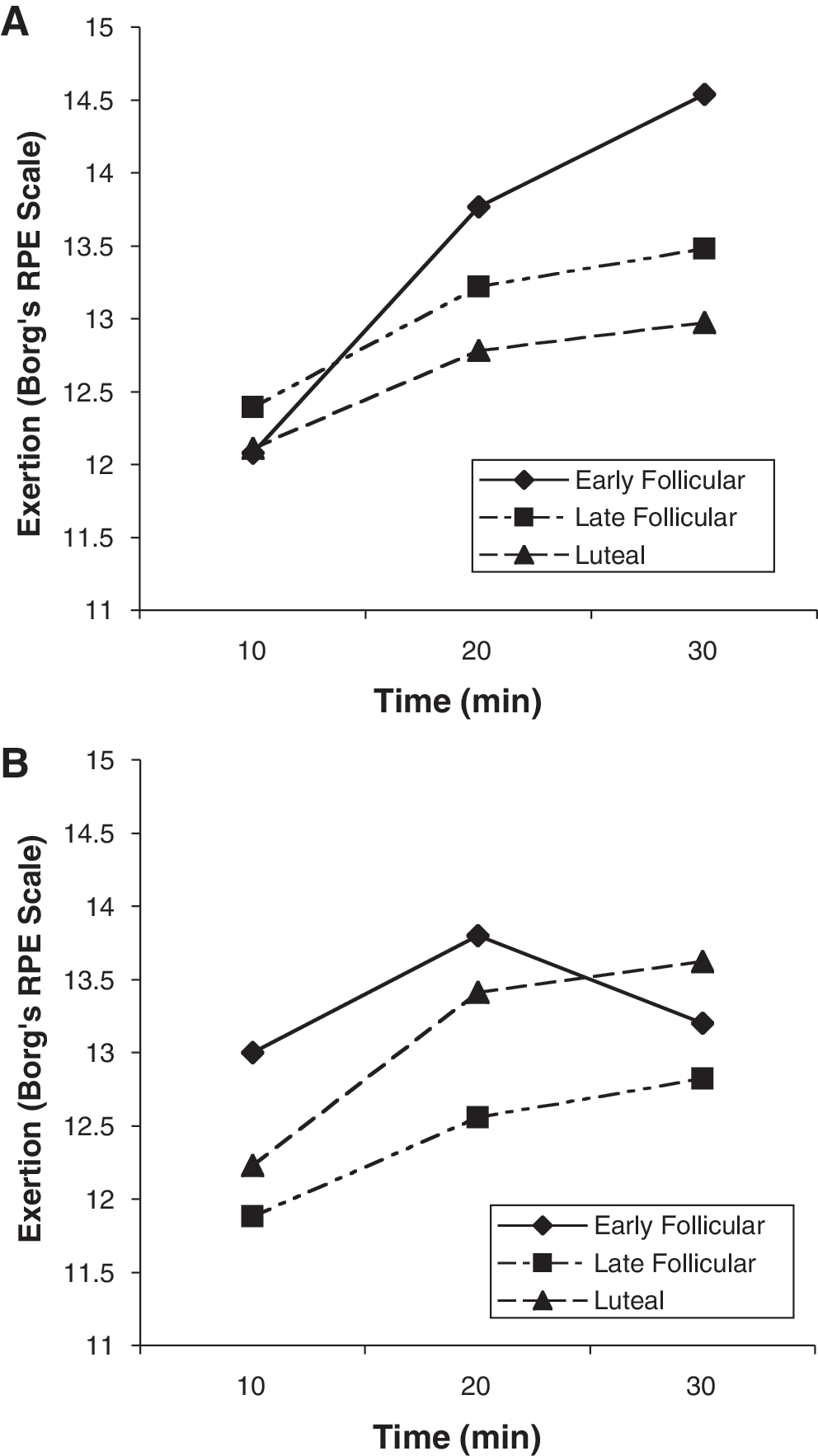
Changes in ratings of perceived exertion (RPE) over time by cycle phase among women not using hormonal contraceptives (HCs) (
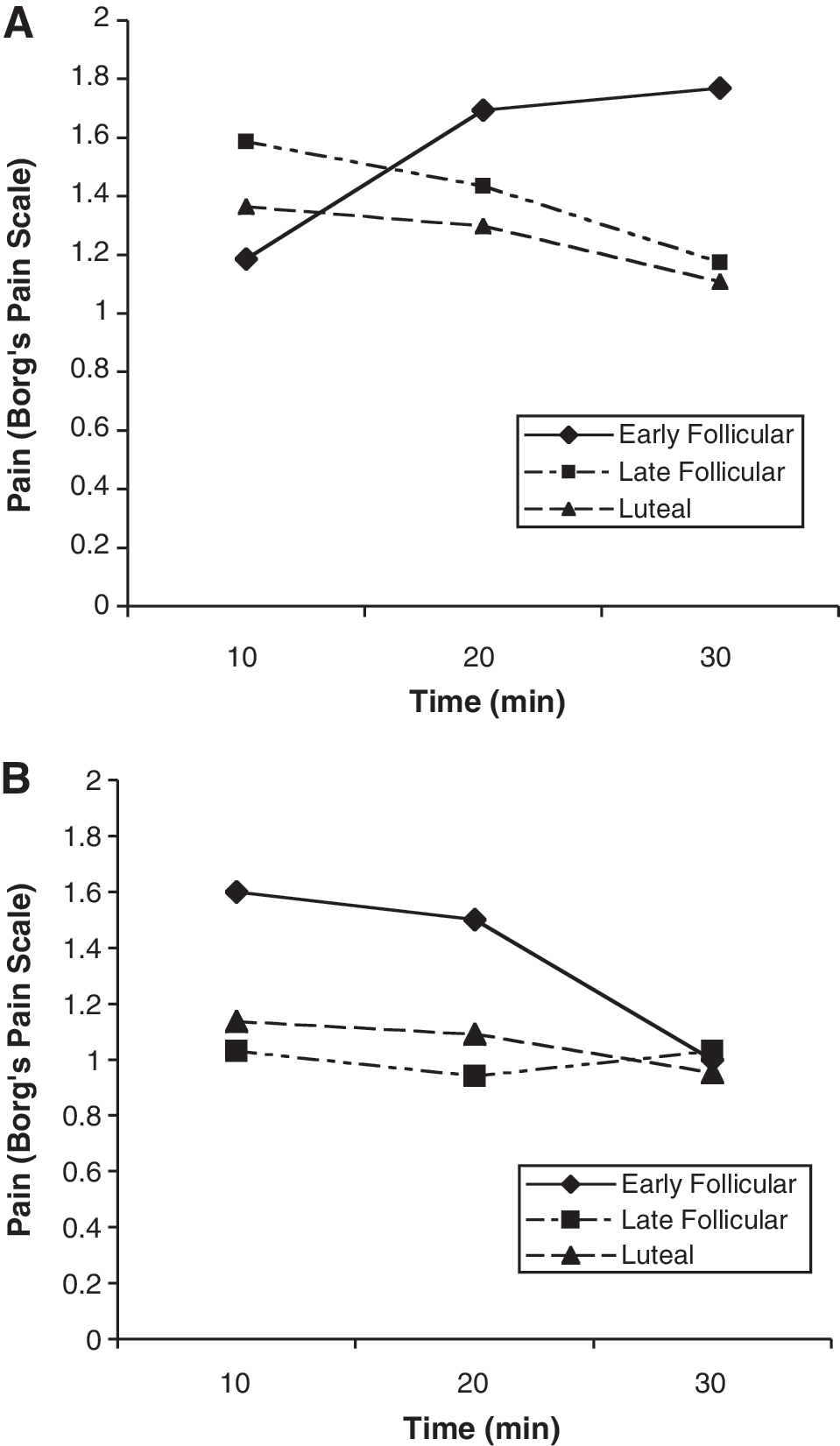
Changes in pain over time by cycle phase among women not using HCs (
RPE, ratings of perceived exertion.
Overall in-task subjective response to exercise
In the full sample of women, there was a significant linear effect of time on RPE, β = 0.61, standard error (SE) = 0.076, p < 0.001, indicating that, on average, RPE increased substantially during the bout. ANOVA components indicated significant variability across individuals in both the intercept and slope (p < 0.0001), but there was no relationship between the intercept and slope (p = 0.15). Thus, not all participants started at the same level of RPE, and not all experienced the same degree of change in RPE across the exercise bout, but the degree of change did not vary as a function of initial RPE. There was a marginal linear effect of time on perceived pain, β = −0.09, SE = 0.049, p = 0.06, indicating that, on average, perceived pain decreased slightly during the bout. ANOVA components indicated significant variability in both the intercept and slope of change in perceived pain (p < 0.0001), but again, there was no relationship between the intercept and slope (p = 0.14). Thus, participants varied significantly in their initial rating of pain and in the pattern of ratings of pain over time, but participant's initial rating of pain was not related to change in pain over time.
Exercise response and menstrual phase (early follicular, late follicular, and luteal)
There was a significant menstrual phase × HC interaction on change in RPE, F(2, 111) = 3.75, p < 0.05 (Fig. 3). Simple effects tests indicated that the effect of menstrual phase was significant among women not using HCs (p < 0.05) but was not significant among controls (p = 0.30). For women not using HCs, those in the early follicular phase experienced a significantly steeper increase in RPE across the bout than did those in the late follicular or luteal phase.
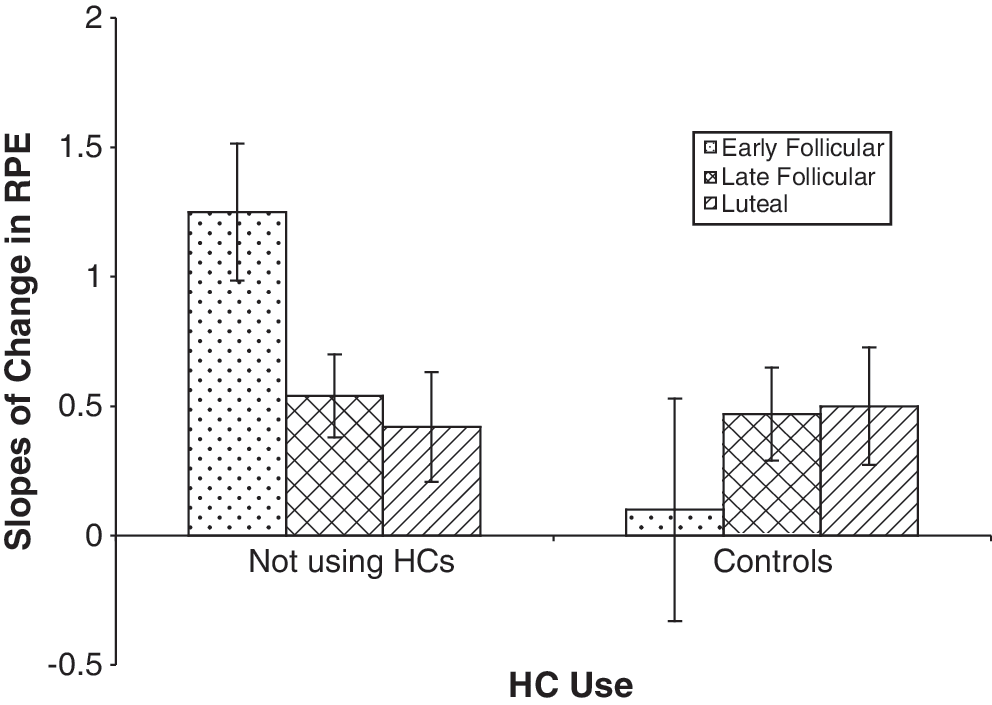
Significant interaction (p < 0.05) of HC use and menstrual cycle phase on slopes of change in ratings of RPE over the course of a 30-minute bout of aerobic exercise at 65% of maximum oxygen consumption (V
There was also a significant menstrual phase × HC interaction on change in perceived pain, F(2, 110) = 3.31, p < 0.05 (Fig. 4). Simple effects tests indicated that the effect of menstrual phase was again significant among women not using HCs (p = 0.01) but was not significant among controls (p = 0.59). Women not using HCs in the early follicular phase experienced an increase in pain across the bout, whereas every other group experienced no change or a decrease in pain. It should be noted that restricting the sample such that the luteal phase included only women who were in days 18–25 did not significantly alter the results for changes in RPE or pain.

Significant interaction (p < 0.05) of HC use and menstrual cycle phase on slopes of change in ratings of perceived pain over the course of a 30-minute bout of aerobic exercise at 65% of V
Exercise response and menstrual phase (early follicular/menses and non-menses)
There was a significant menstrual phase × HC interaction on change in RPE, F(1, 112) = 6.45, p < 0.05. Simple effects tests indicated that those women not using HCs and experiencing menses had significantly steeper increases in RPE than those not in menses (mean = 0.475, SD = 0.89, p < 0.01). Again, this difference was not significant among controls (p = 0.22). There was also a significant menstrual phase × HC interaction on change in perceived pain, F(1, 112) = 6.49, p < 0.05. Simple effects tests indicated that the effect of menstrual phase was again significant among women not using HCs (menses: mean = 0.4, SD = 0.84; nonmenses: mean = −0.16, SD = 0.54, p < 0.01) but was not significant among controls (p = 0.31).
Discussion
Consistent with our hypothesis, our results suggest that cycle phase influenced sedentary women's subjective psychological response to a bout of moderate intensity exercise, but only among those not using HCs.
Next, and consistent with previous research, 26,28,29 our hypothesis that sedentary women in the early follicular phase would experience steeper increases in pain during exercise was supported among women not using HCs, whereas all other groups had no change or a decrease in pain. This finding is consistent with the only other study that examined changes in pain related to exercise and did not observe differences in exercise-induced analgesia between the midluteal and midfollicular phases. 24 Interestingly, the early follicular phase is the time during the cycle when the endogenous hormone profiles of women using and not using HCs are the most similar, with low levels of both estrogen and progesterone. 48 One potential explanation for the observed difference in psychological response is that the more pronounced drop in endogenous hormones in women not using HCs may increase relative pain sensitivity, whereas the less severe decline due to exogenous hormones used in HCs results in lower variability across the cycle in women using HCs. 49 This is also consistent with research showing endogenous estrogen exerting a protective effect against pain, 28,29 as well as research on decreased mood fluctuations in women using HCs. 33
Finally, the hypothesis that women in the luteal phase would have greater increases in RPE was not supported. Instead, women not using HCs who were in the early follicular phase experienced a significantly steeper increase in RPE compared to those in the late follicular or luteal phases. This finding contrasts with previous findings demonstrating higher ratings of mean RPE among women in the ovulatory 11 and luteal 19 phases, as well as other studies that did not find differences in within-subject ratings of RPE across the cycle. 9,10,15 –17 This difference could be methodological, as we used a large sample of sedentary women responding to an initial bout of moderate intensity exercise, whereas the other studies used very small samples of active women. Another possible explanation is that the increases in RPE were related to the observed increases in ratings of pain across the exercise bout. To test this, we examined the bivariate correlation between increases in RPE and increases in pain and found they were indeed significantly correlated (r = 0.548, p < 0.001). Thus, sedentary individuals may express their discomfort in response to an extended session of moderate intensity exercise in ratings of perceived pain and exertion similarly.
Limitations
These results are preliminary and limited in important ways. First, we were limited by a cross-sectional, between-subjects design, not ideal for characterizing within-subject changes across the cycle. However, given that we were interested in sedentary women's subjective experience to an initial bout of moderate intensity exercise, a longitudinal design was not possible. In addition, these results cannot be generalized to active women.
We also used a published and conservative estimate of cycle phase. 36 –41 While only a crude estimate, this method has the advantage of simplifying optimal scheduling of an exercise intervention based on a brief screening interview rather than hormonal measurement, but future studies should measure hormones directly to ensure that women's self-reported cycle day and hormonally estimated cycle day result in similar phase designations. However, the differences observed in this study were between women experiencing menses and those not experiencing menses and are, therefore, not contingent on distinguishing between late follicular and luteal phases through hormonal verification. That said, future studies should measure hormones directly to more accurately elucidate the relationship between the specific hormones that characterize the different phases and identify the hormones (or lack of hormones) that are related to the differences observed. In addition, we grouped all women who were using HCs together, when different types of HCs (monophasic, biphasic, triphasic) can cause very different patterns of exogenous hormones across the cycle. A more comprehensive understanding of the influence of HCs on changes in exercise response across the cycle requires a more in-depth study comparing the specific types of HCs used by women.
Finally, we did not measure dysmenorrhea directly and, therefore, cannot rule out the possibility that the women in the early follicular phase were suffering from painful periods, which can influence performance. 25 We did measure baseline pain, however, and found it was unrelated to increases in pain among women not using HCs in the early follicular phase (r = −0.295, p = 0.379); our qualitative data, moreover, indicate that women in this category who reported the type of pain they were experiencing primarily described pain in their legs, feet, and ankles, not menstrual pain. Nonetheless, the current findings suggest the value of future work examining whether exercise-induced increases in pain and RPE are coincident with or independent of dysmenorrhea during the early follicular phase.
Despite these limitations, this study contributes to the literature in three fundamental ways: (1) we used a sedentary sample to measure responses to an initial bout of moderate intensity exercise, (2) we used a substantially larger sample size adequately powered to detect changes in psychological response, and (3) we calculated within-subject slopes in order to measure individual change in RPE and pain in response to exercise rather than simply averaging across time points or using only one rating of RPE and pain.
Conclusions
The observed pattern of change in subjective response to exercise across the cycle provides preliminary evidence that the subjective response of sedentary women not using HCs to a bout of submaximal exercise is influenced by the natural cyclical variation in hormones that characterizes the menstrual cycle, such that women in the early follicular phase experienced steeper increases in RPE and pain. The underlying mechanisms that lead to differences in subjective response to exercise across the cycle remain unclear, and further investigation is needed. These findings can be used in planning the optimal timing of interventions targeted at increasing exercise behavior in sedentary women.
Footnotes
Acknowledgments
This research was supported by grants from the National Cancer Institute (RO1 CA109858) and the General Clinical Research Center Program of the National Center for Research Resources, National Institutes of Health (M01-RR00051). We thank our participants for their contribution. Several undergraduates, graduate students, postdoctoral researchers, and professional research assistants made significant contributions to this project, including Sara Anne Tompkins, Renea Nilsson, and Laura Carpenter. We also thank Paul Hooper and three anonymous reviewers who greatly contributed to previous versions of this article.
Disclosure Statement
The authors have no conflicts of interest to report.