
Abstract
Background:
Chronic kidney disease (CKD) has emerged as an independent predictor for cardiovascular disease (CVD), which is now regarded as an inflammatory disease. This study aimed to determine the association of CKD with white blood cell (WBC) count as a marker of systemic inflammation.
Methods:
We examined the association of WBC count with CKD in 2825 Korean adults (1155 men, 1670 women) in the 2007 Korean National Health and Nutrition Examination Survey (KNHANES). CKD was defined as either proteinuria or a glomerular filtration rate (GFR) <60 mL/min/1.73 m2. The odds ratios (ORs) for CKD were calculated using multivariate logistic regression analysis after adjusting for confounding variables across gender-specific WBC count quartiles.
Results:
The proportion of CKD increased with increasing WBC quartiles, from 9.7% in the lowest quartile to 20.7% in the highest quartile for women. In multivariate logistic regression analysis, the corresponding odds ratios (95% confidence intervals [CIs]) for a CKD across WBC count quartiles among women were 1.00, 1.45 (0.91-2.31), 1.65 (1.03-2.63), and 2.11 (1.33-3.35), after adjusting for age, body mass index (BMI), systolic blood pressure, fasting plasma glucose, smoking status, current drinking high-density lipoprotein cholesterol (HDL-C), and triglyceride. In contrast, compared with women, men appeared to have no significant results of a relationship between WBC quartiles and CKD.
Conclusions:
Our study shows a significant association between WBC count and the risk for CKD in women. Accordingly, potential health benefits of early detection of a higher level of WBC count may be useful for CKD risk assessment in women.
Introduction
Chronic kidney disease (CKD) is a worldwide public health problem. According to data from the Third National Health and Nutrition Examination Survey (NHANES III), about 8.3 million U.S. adults aged ≥20 years have CKD. 1 Recently, the prevalence of CKD is showing an upward trend for a number of CKD risk factors, including an increase in the proportion of individuals with obesity, diagnosed diabetes, and hypertension. 2
It is increasingly appreciated that chronic renal dysfunction is an independent risk factor for cardiovascular disease (CVD), which is now regarded as an inflammatory disease. 3 –6 Traditional CVD risk factors, such as older age, male gender, cigarette smoking, hypertension, diabetes, and dyslipidemia, are highly prevalent in CKD populations. 7,8 Previous epidemiological studies also suggest that CKD may be a renal manifestation of metabolic syndrome, a condition linked to insulin resistance and chronic low-grade inflammation. More recent research has shown that chronic low-grade inflammation plays an important role in the pathogenesis of CKD. 9 Systemic markers of inflammation, such as C-reactive protein (CRP) levels, correlate with not only higher coronary risk but also impaired kidney function in the general population. 10 –12 A higher level of CRP is associated with endothelial injury and impaired vasodilation, which may lead to glomerular damage and progressive loss of kidney function. 13,14
White blood cell (WBC) count, a nonspecific inflammation marker, is widely used in standard clinical practice. Recently, WBC count has become a useful predictor for certain diseases, in addition to being a marker of infection or inflammation. A higher WBC count, even within the normal range, has been significantly associated with atherosclerotic CVD incidence and mortality. 15 A previous study demonstrated that the WBC count was a novel mortality predictor in hemodialysis patients. 16 If the development and progression of CKD are mediated by chronic low-grade inflammation, we would expect positive associations between WBC count and CKD.
The purpose of this study was to examine the association between WBC count and the prevalence of CKD in Korean adults in the 2007 Korean National Health and Nutrition Examination Survey (KNHANES).
Materials and Methods
Study population
This study was based on data obtained from the 2007 KNHANES, a cross-sectional and nationally representative survey conducted by the Korean Ministry of Health and Welfare in 2007.
The target population of the survey was noninstitutionalized civilians aged ≥1 year in Korea. Sampling units were households selected through a stratified, multistage, probability sampling design based on geographic area, sex, and age group using household registries. 6455 subjects from 23 households were included in the study. One hundred sampling frames, consisting of 2300 households from the primary sampling units, were randomly sampled. Of these, 4594 subjects (71.2%) were included. Weights indicating the probability of being sampled were assigned to each participant, enabling the results to represent the entire Korean population. Participants completed four parts of a questionnaire that consisted of a Health Interview Survey, Health Behavior Survey, Health Examination Survey, and Nutrition Survey. The Health Examination Survey was completed by 4264 (65.8%) of the 6455 selected individuals who had taken part in the Health Interview Survey. Blood tests were performed on 3467 people aged ≥10 years. Data from 3011 adults aged ≥18 years were used for this study. Subjects with WBC counts ≥10,000 cells/μL were excluded to rule out the possibility of current infection (n = 186). After these exclusions, 2825 subjects (1155 men, 1670 women) were included in the final analysis.
Measurements
At the time of the 2007 KNHANES, citizens were informed they had been randomly selected as a household to voluntarily participate in the nationally representative survey conducted by the Korean Ministry of Health and Welfare in 2007 and that they were given the right to refuse to participate in accordance with the National Health Enhancement Act supported by the National Statistics Law of Korea.
The participants gave written informed consent to participation in the study. The Korea Centers for Disease Control and Prevention also obtained written informed consent to use sera for further analysis. This study was approved by the Institutional Review Board of Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. The health examinations that were performed in 2007 included a medical history, a physical examination, a questionnaire about health-related behavior, anthropometric measurement, and biochemical measurements. Physical examinations were performed by trained medical staff following a standardized procedure.
Participants were asked about lifestyle behaviors, including cigarette smoking, alcohol consumption, and current treatments for any disease. They were asked for the data of any diagnoses and a list of medications being taken. Completed questionnaires were reviewed by trained staff and entered into a database. Smoking exposure was categorized as nonsmoker, former smoker, and current smoker. Alcohol intake was categorized as nondrinker or current drinker.
Body weight and height were measured in light indoor clothing without shoes to the nearest 0.1 kg and 0.1 cm, respectively. Body mass index (BMI) was calculated as the ratio of weight (kg)/height (m2). Blood pressure was measured in the right arm using a standard mercury sphygmomanometer (Baumanometer). Two systolic and diastolic blood pressure readings were recorded at 5-minute intervals and averaged for analysis. After a 12-hour overnight fast, blood samples were obtained from subjects from an antecubital vein.
WBC counts were quantified by an automated blood cell counter (ADVIA 120). Fasting plasma glucose, total cholesterol, triglyceride, high-density lipoprotein cholesterol (HDL-C), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and creatinine were measured using an ADVIA1650 autoanalyzer. The urine protein concentration was determined from the results of a single urine dipstick semiquantitative analysis (Uriscan pro). Dipstick urinalysis was performed on fresh, midstream urine samples that were collected in the morning. The results of the urine test were based on a scale that quantified proteinuria as absent, trace, 1+, 2+, 3+, and 4+. The dipstick results of 1+, 2+, 3+, and 4+ corresponded to protein concentrations of 30, 100, 300, and 1000 mg/dL, respectively. Proteinuria was defined as a finding of ≥1+ from the dipstick results. Kidney function was estimated by the glomerular filtration rate (GFR), which was calculated with the simplified Modification of Diet in Renal Disease (MDRD). The study equation was:
for a female subject. 1,17 CKD was defined as either proteinuria or a GFR <60 mL/min 1.73 m2.
Statistical analysis
Because WBC counts differ significantly by gender, WBC quartiles were categorized separately as follows: Q1, <5700; Q2, 5700–6700; Q3, 6800–7700; Q4, ≥7800 cells/μL for men; Q1, <5000; Q2, 5000–5900; Q3, 6000–7000; Q4, ≥7100 cells/μL for women. The characteristics of the study population were represented using the independent 2-sample t test or the 1-way analysis of variance (ANOVA) test for continuous variables and chi-square test for categorical variables. The odds ratios (ORs) and 95% confidence intervals (CIs) for CKD were calculated using a multivariable logistic regression analysis after adjusting for confounding variables across WBC count quartiles. All analyses were conducted using SPSS statistical software, version 15.0. All statistical tests were determined at a p value <0.05.
Results
Table 1 shows the characteristics of the 1155 men and 1670 women. There was no significant age difference between men and women. Men, on average, had greater BMI, blood pressure, fasting plasma glucose, triglyceride, AST, ALT, creatinine, and WBC counts, but lower total cholesterol and HDL-C than women. The prevalence of CKD was 14.2% in men and 15.1% in women.
Values are given as mean ± standard deviation (SD), median (interquartile range), or percentage.
Frequency of alcohol drinking ≥two times/month.
The demographic and biochemical characteristics of the study population in relation to WBC quartiles are shown in Table 2. The mean BMI, total cholesterol, and triglycerides were highest in the fourth quartile of WBC count in both men and women, whereas the HDL-C level was lowest in the fourth quartile. The proportion of CKD increased with increasing WBC quartiles, from 9.7% in the lowest quartile to 20.7% in the highest quartile for women.
Data are expressed as mean ± SD, median (interquartile range), or percentage.
Frequency of alcohol drinking ≥two times/month.
WBC, white blood cell; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BP, blood pressure; CKD, chronic kidney disease; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; Q, quartile.
Figure 1 shows the prevalence of CKD according to WBC quartiles. The percentage of CKD gradually increased in accordance with WBC quartiles in women: 9.7%, 13.7%, 16.2%, and 20.7% respectively (p < 0.001). These associations were not observed in men, however. In multivariate logistic regression model 2, the corresponding ORs (95% CIs) for CKD across WBC count quartiles for women were 1.00, 1.52 (0.96-2.42), 1.74 (1.09-2.77), and 2.30 (1.46-3.62) after adjusting for age, BMI, blood pressure, fasting plasma glucose, smoking status, and current drinking. We also assessed the association between WBC count and the risk for CKD after additional adjustment for triglyceride and HDL-C levels. These associations were similar after using model 3 in women. In contrast, compared with women, there appeared to be no significant relation between WBC quartiles and CKD in men (Table 3).
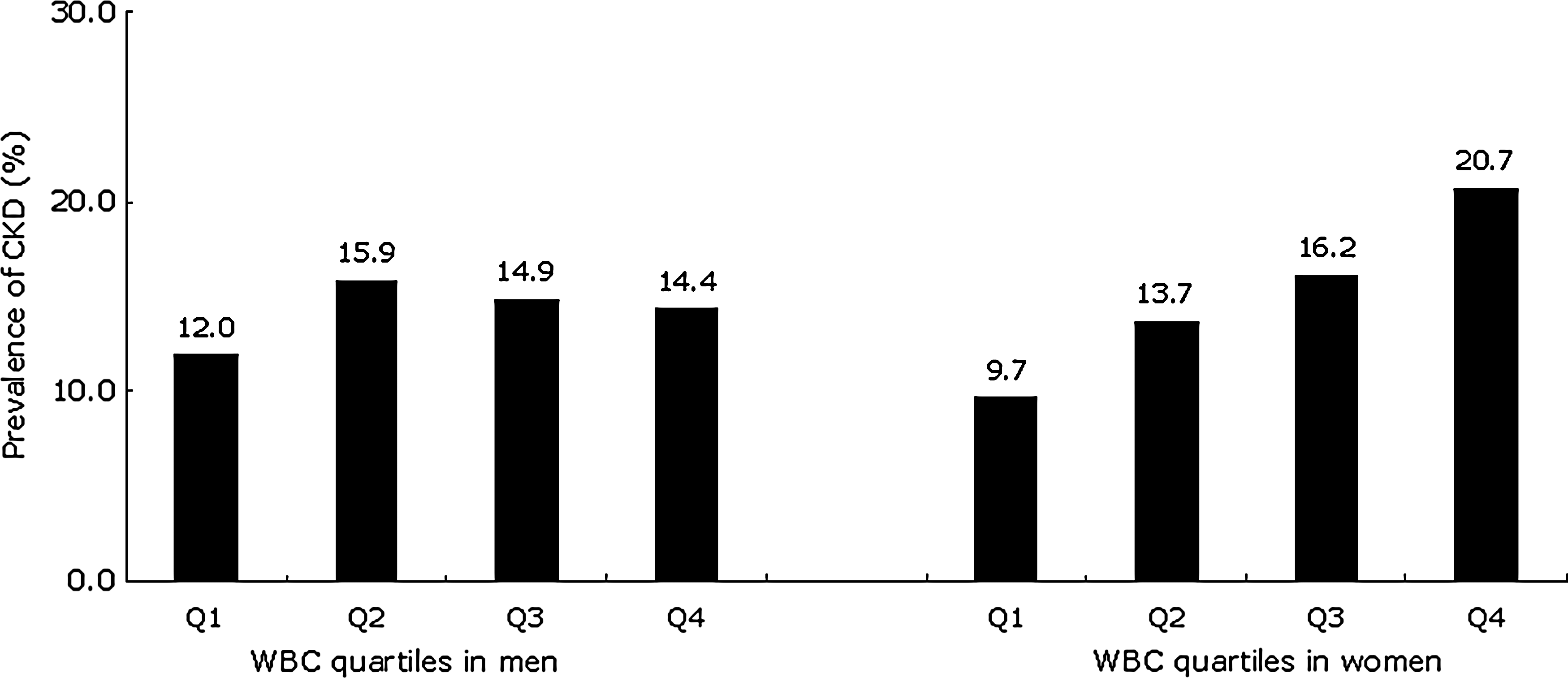
The prevalence of chronic kidney disease (CKD) according to white blood cell (WBC) quartiles (Q) in men and women.
Model 1: adjusted for age.
Model 2: adjusted for age, body mass index, systolic blood pressure, fasting plasma glucose, smoking status, and current drinking.
Model 3: adjusted for age, body mass index, systolic blood pressure, fasting plasma glucose, smoking status, current drinking, HDL-C, and triglyceride.
Discussion
In this cross-sectional study, we found positive and graded associations between WBC count and CKD independent of classic CVD and CKD risk factors for women. These data suggest a possible role of inflammation in the pathogenesis of CKD, particularly in women.
Increasing evidence suggests that CKD and CVD share common risk factors and are outcomes of the same predisposing disorders. 18 –20 Patients with detected chronic renal insufficiency are at risk for the development of CVD as well as progression to end-stage renal disease (ESRD). Moreover, the level of renal function is independently effective in predicting the CVD mortality and morbidity. Based on these data and others, the National Kidney Foundation practice guidelines recommend identifying persons at increased risk (those with diabetes and those with hypertension) and detecting patients with kidney damage and estimating the GFR. 18 Demonstration of common risk factors may indicate that cardiovascular and kidney diseases are mediated by common underlying mechanisms. Furthermore, the number of cardiovascular risk factors appears to correlate with the severity of kidney dysfunction in a dose-response manners. 8 In our study, however, there were gender difference associations between WBC count quartiles and the prevalence of CKD.
Although the reason for these discrepancies in gender difference associations of WBC count with CKD prevalence is unclear, some explanations may be offered. There is a marked sexual dimorphism in the aging kidney, with women being protected. Previous studies have shown that age-related falls in GFR tend to be delayed in women. 21 It is reasonable to attribute the sexual dimorphism in the aging kidney to the different vascular actions of estrogen and androgen. Estrogen may have potent and direct antigrowth effects on glomerular mesangial cells and also have inhibitory effects on mesangial extracellular matrix (ECM) accumulation, which are important in the development of glomerular sclerosis. 22 –25 However, hormonal status, such as estrogen level, was not measured in the present study. Thus, further studies of the gender-specific relationship between WBC count and CKD are warranted. Apart from the beneficial effect of estrogen, androgen itself may be associated with the development and progression of CKD. Experimental studies have shown that castrated male rats are protected from mild renal vasoconstriction and glomerular sclerosis. 26 Another possible explanation is that there is a sexual dimorphism in the nitric oxide (NO) system. NO deficiency occurs in various types of CKD and may contribute to progressive loss of kidney function. 27 NO is known to be a potent vasodialator and is also recognized as an antigrowth mediator that can inhibit mesangial cell growth and ECM production. Indeed, endothelial NO-dependent vasodilation has been documented to be impaired with increasing age in normal humans and rats. 28 –30 There is a sexual dimorphism in the NO system between men and women, with premenopausal women making more total NO than do men. 31 Moreover, there is a greater abundance of the constitutive NO synthase (NOS) in female than in male rat kidney. 32
Our study has several limitations. First, it comprises a cross-sectional design, suggesting that caution should be used in causal interpretations. Because of the limitation of the study design, we cannot conclude whether a higher WBC count is a risk factor actively involved in the development of CKD or just a bystander of CKD. Further prospective and experimental research is warranted to better understand its pathophysiological role in the development and progression of CKD. Second, only one measurement of WBC count was included in the analysis, and it was not possible to determine if an acute and brief episode of infection or chronic inflammation was responsible for the correlation observed. In order to minimize the possibility of including subjects with current active infection, we excluded subjects with a WBC count ≥10,000 cells/μL. Moreover, we did not take into consideration the effect of WBC differential count, particularly WBC differential count, such as neutrophils and monocytes, which are known to be associated with CVD and metabolic syndrome. 33,34 Unfortunately, because this study used secondary data from the 2007 KNHANES, we could not obtain differential WBC counts. Further studies are needed to examine whether or not the differential WBC count was associated with CKD.
Third, we used an estimated GFR instead of a directly measured GFR to define CKD. A recent review article 35 reported that current GFR estimates had greater inaccuracy in populations without known CKD than in those with the disease. The recent report of the Asian Forum of Chronic Kidney Disease Initiatives also suggested that a planned action is needed to validate the existing GFR-estimating equations in Asian populations. 35 The serum creatinine and estimated GFR equations may be influenced by a number of factors, such as genetic variation, dietary habits, and lifestyle behaviors. Moreover, commonly used methods for serum creatinine measurement may have analytic bias and nonspecificity issues. 36 Nonetheless, current GFR estimates facilitate the detection, evaluation, and management of CKD, and many organizations recommend the use of equations that estimate GFR for the evaluation of renal function in epidemiological studies and in clinical practice. 37 Finally, dipstick urinalysis may have imperfect sensitivity and specificity, but the number of false positive results can be higher because of menstruation or comorbid illnesses in women and older people. In addition, the National Kidney Foundation Kidney Disease Outcome Quality Initiation Advisory Board recommends that under most circumstances, spot urine samples rather than timed urine collection (overnight or 24 hours) can be used for detection and monitoring proteinuria in adults. 1
In conclusion, our study shows positive associations between WBC count and the risk for CKD in women independent of traditional CVD and CKD risk factors. Given the health implications of CKD, early detection of a higher WBC count may be useful for CKD risk assessment in women.
Footnotes
Disclosure Statement
The authors have no conflicts of interest to report.