
Abstract
Objective:
This study provides a descriptive sociodemographic profile of allostatic load (AL) among adult women of all age groups, focusing on how age patterns of AL vary across racial/ethnic groups. Allostatic load, an index of cumulative physiological dysregulation, captures how the cumulative impact of physiological stress responses from person-environment interactions causes wear and tear on the body's regulatory systems, which in turn can lead to disease outcomes and health disparities.
Methods:
Using data from the National Health and Nutrition Examination Survey (NHANES) 1999–2004, this study examines AL in a nationally representative sample of women ≥18 years of age (n=5765). Measures of AL using 10 biomarkers representing cardiovascular, inflammatory, and metabolic system functioning were created. Multivariate negative binomial regression models were used, and predicted AL scores were computed.
Results:
Black women had the highest predicted AL scores relative to other racial/ethnic groups, and a marked black/white gap in AL persisted across all age groups. Age by race/ethnicity interaction terms revealed significant racial/ethnic differences in AL patterns across age groups. Black women 40–49 years old had AL scores 1.14 times higher than white women 50–59 years old, suggesting earlier health deterioration. Mexican women not born in the United States had lower predicted AL scores than those born in the United States.
Conclusions:
This study provides one of the first descriptive profiles of AL among a nationally representative sample of adult women in the United States and presents racial/ethnic trends in AL across age groups that are useful for identifying demographically and clinically important subgroups at risk of having high cumulative physiological dysregulation.
Introduction
An extensive body of literature has established links between socioenvironmental factors and differential morbidity and mortality rates across social groups, and there is continued interest in better understanding how health disparities emerge over the life course. 1 –3 Allostatic load (AL), an index of cumulative physiological dysregulation, has been proposed to elucidate potential biological pathways by which socioenvironmental factors “get under the skin.” 1,4,5 AL denotes the cumulative impact of physiological stress responses that chronically exceed optimal operating ranges and cause wear and tear on the body's regulatory systems. 6 –10 The cumulative biological burden exacted on the body represents some of the earliest evidence of decline in health that may eventually lead to disease pathology and disability. 11 This study extends this line of inquiry by focusing exclusively on a nationally representative sample of women and describing AL levels by race/ethnicity, age, nativity status, and other relevant sociodemographic characteristics.
AL serves as a useful construct for gaining a better understanding of possible biological processes that link sociodemographic characteristics and health. When environmental conditions are perceived as stressful, the sympathetic adrenal medullary system and the hypothalamic pituitary adrenocortical (HPA) axis are activated, which in turn signal changes in multiple physiological systems as part of a generalized stress response. 6,11 –13 Healthy functioning requires ongoing fluctuation in physiological systems in response to stressful experiences, but these fluctuations are adaptive only in the short run and within optimal systemic ranges. 14 When repeatedly exposed to perceived challenges over the life course, however, these systems may begin to operate inefficiently or outside their optimal ranges, which leads to development of AL and additive, synergistic, and cumulative effects on health over time. 7 AL in turn may develop into disease states among individuals and health disparities at the population level. 11 Prior research has shown higher AL to be associated with mortality, cardiovascular disease, and decreased physical and cognitive functioning. 8,9,15 –19
The formulation of AL by McEwen and Seeman 13 and Seeman et al. 10 included primary mediators and secondary markers involved in physiological stress responses. Primary mediators are circulating hormonal agents that mediate the body's response to stressors through their effects on tissues and organs (e.g., cortisol, epinephrine, C-reactive protein [CRP] and dehydroepiandrosterone-sulfate [DHEA-S]). Primary mediators interact with each other and tissue substrates to produce secondary outcomes, which are biological parameters or functional states that indicate pathophysiological processes (e.g., systolic and diastolic blood pressure, body mass index [BMI], cholesterol). The research presented here draws from prior work and includes cardiovascular, metabolic, and inflammatory markers in our operationalization of AL. Although we include a comprehensive set of markers, because of data limitations, we were unable to incorporate neuroendocrine primary mediators. Nonetheless, the biomarkers we use represent a comprehensive array of physiological systems involved in the generalized physiological stress response to create an adequate and informative measure of AL among a nationally representative sample of adult women.
As individuals age, AL accumulates from prior experiences and is expected to increase due to gradual deterioration of organ and system functioning and reduced capacity to adapt to stressors. 4,20 Within an age group, however, there is variation in AL that reflects differences in life experiences and associated physiological reactions. 8 Race/ethnicity and nativity status are important social conditions contributing to these differences in AL. 21 Thus, AL may accrue more rapidly over time for certain groups of women, particularly women in disadvantaged racial/ethnic minority groups. 22 In a nationally representative sample of adults, Geronimus et al. 22 found a black/white disparity in AL to be present in all age groups, that it increased with age, and that it was especially pronounced after age 30, net of socioeconomic status (SES). There is also evidence that AL depends on both gender and race/ethnicity, with black women having disproportionately higher AL relative to black men and white women. 22 In addition, AL has been shown to be lower among Mexicans not born in the United States, that is, foreign-born Mexicans, compared to U.S.-born Mexicans and those with shorter duration of residence in the United States. 23 –25 Lower SES, as measured by education, household income, neighborhood poverty and income, has also been associated with higher AL. 26,27
Whereas prior research using nationally representative samples has investigated race or SES differentials in AL, 23,25 –27 relatively less emphasis has been placed on gender differences and gender-specific patterns in AL. In order to account for fundamentally different biological makeup and social experiences between men and women and to better understand how health disparities develop among women, women-specific research on cumulative physiological dysregulation is warranted. A unique contribution of this study is that we analyze women specifically to better identify sociodemographic patterns of AL in a nationally representative sample of women, which allows for greater generalizability of results. Prior research 8 –10,17,20,25 generally combines men and women when identifying AL cutoffpoints, with some exceptions, 24,28,29 despite research showing gender variation in distributions of individual biomarkers. 30 In comparison to women, men are at higher risk in cardiovascular markers, such as total cholesterol, blood pressure, glycosylated hemoglobin, and waist/hip ratio. 30 –34 Women, on the other hand, tend to exhibit higher risk than men in CRP (a marker of inflammation) levels and biomarkers representing neuroendocrine functioning. 30,35 –37 Other research has also shown gender differences in cumulative biological risk, with some studies showing men with higher overall levels 15,30 and other studies showing women across different populations with higher levels. 38,39 These combined findings suggest differential patterns of biological risk between men and women and warrant further examination of composite biological risk measures using gender-specific cutoffpoints. To our knowledge, this is the first study to use gender-specific cutoff points in a nationally representative of women in the United States.
Furthermore, there has been little research done on age and race interaction effects on AL, with the exception of the study by Geronimus et al., 22 which demonstrated higher AL at younger ages among African Americans compared to whites, suggesting earlier health deterioration, or weathering. This study expands upon this finding by explicitly focusing on between-women differences in AL and elaborating on interactive effects of age and race/ethnicity. A unique contribution of this study is that it expands beyond black/white differences and examines AL among a nationally representative sample of women of Mexican descent. In doing so, our analysis includes a more homogeneous group of Hispanic women, thereby allowing for more meaningful racial and ethnic comparisons. 40
This study used data from the National Health and Nutrition and Examination Survey (NHANES) 1999–2004 to examine AL among adult women of all age groups in the United States. The objectives of this study were to examine sociodemographic correlates of AL among women, assess if age patterns of AL vary across racial/ethnic groups, investigate the effect of nativity status on AL among Mexican women, and identify clinically and demographically important subgroups of women at high risk of having elevated cumulative physiological dysregulation. We hypothesized that black women would have higher AL scores relative to white women within each age group; morever, younger black women were expected to exhibit higher AL scores than older white women, controlling for other covariates. We also hypothesized that foreign-born Mexican women would have healthier cumulative biological risk profiles, as indicated by lower AL, than their U.S.-born counterparts. Examining the AL in women across age and racial/ethnic groups can help provide useful information on differential health and aging patterns, identify high-risk demographic groups, and inform timing of preventive interventions.
Materials and Methods
Data description
The NHANES survey is a cross-sectional study that uses a stratified, multistage probability sampling design to provide national estimates of health and nutritional status for the civilian, noninstitutionalized U.S. population. 40 Beginning in 1999, NHANES has been collected on a continuous basis and released every 2 years; this study uses data from 1999–2004. Eligible respondents are obtained with the use of household-based sampling procedures. Survey components include questionnaire interviews, clinical examination, and laboratory procedures (the clinical and laboratory components occur in mobile examination centers [MEC]). 40 Standardized procedures and protocols were developed and validated by the National Center for Health Statistics (NCHS) for all clinical examinations and laboratory tests. The response rate was approximately 77% for the interview portion and 71% for the MEC examination portion from the screened sample; among women who completed the interview portion, response rate for the MEC examination was 92%. 41 The analytical sample included all women aged ≥18 years who had valid data on all biomarkers used to create the AL score; were not pregnant; identified themselves as non-Hispanic white, non-Hispanic black, or Mexican American; and completed the interview and MEC examination components (n=5765).
Biomarker measures and AL scores
A total of 10 biomarkers were used for the creation of AL scores and were selected based on representation of multiple systems, availability in the dataset, and prior research. 8,20,22 The cardiovascular markers were systolic and diastolic blood pressure, resting pulse rate, and homocysteine. The inflammatory markers were C-reactive protein (CRP) and serum albumin; metabolic functioning was represented by glycosylated hemoglobin, high-density lipoprotein (HDL), total cholesterol, and body mass index (BMI). AL scores were created using empirical cutoff points based on the weighted distribution of the analytical sample and a count-based summation method following previous work. 5,10
Values above the 75th percentile were defined as high risk for all the biomarkers, with the exception of HDL and serum albumin, for which values below the 25th percentile were defined as high risk. 5,8 –10 Use of empirically based cutoff points was intended to capture cumulative physiological dysregulation at more stringent levels than clinical cutoff points. AL scores were then calculated by summing the number of biomarkers for which the woman fell into the highest-risk quartile; a higher AL score was an indicator of poorer health. We also qualitatively compared our empirically based high-risk values with clinical high-risk cutoff points. 42 –50 Because AL theoretically represents the negative impact of actual physiological dysregulation, women who were on medication were not differentiated from those not on medication and were coded according to their measured values for each biomarker. 51 We considered respondents who were on medication and had biomarker values within healthy ranges to have succeeded in controlling these parameters and were thus experiencing less wear and tear on their regulatory systems.
Independent variables
Race/ethnicity was coded into three categories, with priority given to any mention of Hispanic: non-Hispanic (NH) white, NH black, and Mexican American. Women who indicated more than one race (multiracial) and then selected a main race as NH white or NH black were coded into those respective categories. Respondents who identified with other racial groups, Hispanic groups other than Mexican, more than one race and no main race, or who indicated a verbatim response to nonspecific multiracial heritage were excluded from the study. Nativity status was categorized as born in the 50 U.S. states/Washington, DC, and not born in the United States (born in any other location or foreign country). Age was included as a categorical variable (18–29, 30–39, 40–49, 50–59, 60–69, and 70+ years). SES was measured using educational attainment and family income, two of the most robust and commonly used measures of SES. 52,53 For educational attainment, responses were categorized by NCHS as less than high school, high school graduate (including GED), and more than high school. Family income in the past year was categorized according to quartile groups based on the sample distribution (<$15,000, $15,000–34,999, $35,000–64,999, ≥$65,000). Marital status was coded as never married, currently married/living together, divorced/separated/widowed, and missing. (In part of the 1999–2000 data collection cycle, individuals belonging to single person households were not asked about their marital status. For a number of these individuals, NCHS imputed marital status from other questionnaire items that made reference to their marital status. However, 204 women in our analytical sample remain missing on marital status due to lack of sufficient data for imputation; they were coded to a separate missing category to preserve sample size. Interaction variables for age and race/ethnicity were coded as mutually exclusive categories.) Three-way interaction variables for age, race/ethnicity, and nativity status could not be included in analysis because of limited numbers in categories.
There were no missing data for age and race/ethnicity, and a very small number of individuals had missing data for education, nativity, and marital status. For these variables, missing cases were coded into the modal categories. Results did not change whether the missing cases were dropped or included in the modal categories. Missing values for family income were imputed using a multinomial regression model that included age, race/ethnicity, education, nativity status, and marital status.
Analysis
The distributional qualities, including range, mean, median, and quartiles, and empirical and clinical cutoff points of each of the 10 individual biomarkers and summary AL scores were examined. Differences in mean AL by sociodemographic groups were assessed using bivariate regressions and adjusted Wald F-test. Because AL was operationalized as a nonnegative integer count outcome and followed a nonnormal distribution, negative binomial regression models were used in multivariate regression analyses to investigate main effects of covariates and interactive effects between race/ethnicity and age on AL. Negative binomial regression models were used to account for overdispersion (when variance is greater than mean) and estimate the possible deviation of the variance from that expected under a Poisson distribution. 54,55 Negative binomial regression also allowed us to maximize use of the full distribution of empirical information on AL and more accurately model the underlying count process. 56 Lastly, empirical AL scores were predicted using estimates from negative binomial regression models that included age-by-race interactions and controlled for education, family income, nativity status, and marital status. The control variables were set at modal values (more than high school; $15,000–34,999; U.S.-born; married) for prediction of AL scores. AL scores were predicted separately for U.S.-born and foreign-born Mexican women by substituting appropriate values for nativity status in the same negative binomial regression model, with all other covariates set to the same modal values as described. All descriptive statistics and negative binomial regression estimates were weighted using the NHANES individual-level sampling weights, which adjust for complex sample design, selection, and nonresponse. All analyses and estimates were conducted using Stata 10. 57
Results
Table 1 presents descriptive statistics, including range, median, quartiles, and empirical cutoff points, for the 10 individual biomarkers that comprise AL in this study. The empirically based quartile cutoff points were more stringent than clinical standards of high risk for 8 of the 10 biomarkers (exceptions were BMI and CRP). Mean AL score among all women was 2.71, and the range for AL scores was 0–9, indicating that there were no women who were high risk on all 10 biomarkers. Figure 1 shows the percentage distribution of AL; almost 13% of women had an AL score of 0 (not high risk on any biomarkers), and 18% were high risk on two biomarkers.
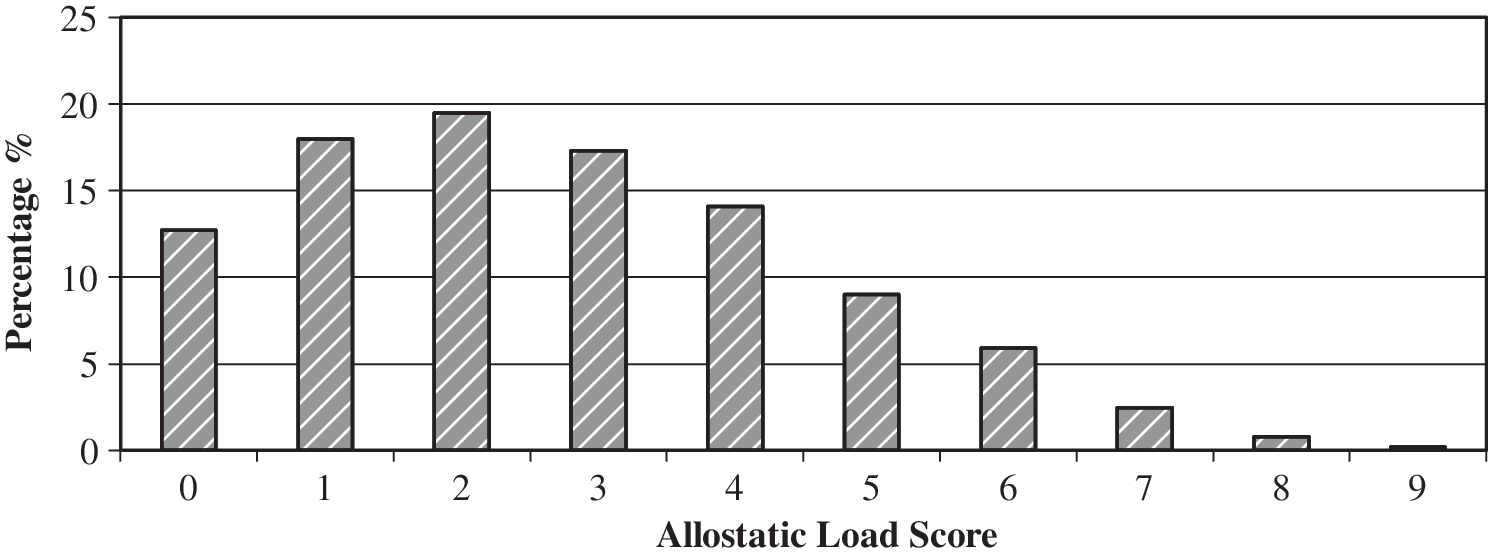
Percentage distribution of allostatic load, adult women, National Health and Nutrition Examination Survey 1999–2004 (n=5765).
There is no established clinical high-risk standard for homocysteine.
Allostatic load scores are the sum of the number of values that are ≥75%, or high risk, for all individual biomarkers, with the exception of albumin and high density lipoprotein, for which values ≤25% are defined as high risk.
Almost 40% of women were under age 40, 37% of women were between the ages of 40 and 59, and about 25% of women were ≥60 years (Table 2). Approximately 80% of women were NH white, 12% were NH black, and 7% were of Mexican descent. The majority of women had more than high school education, and about 28% had a family income of ≥$65,000. Over half of the women were married, and almost one quarter were separated, divorced, or widowed; 16% of women were never married. Most women (92%) were born in the United States. Mean AL scores increased monotonically with older age and lower educational attainment and family income (Table 2). NH black women had the highest mean AL score (3.33); Mexican women had slightly lower AL scores (2.42) than NH white women (2.65). Separated, divorced, and widowed women had the highest mean AL score (3.36), followed by married/cohabiting women (2.62). U.S.-born women had higher mean AL scores than foreign-born women (2.74 vs. 2.41). Median AL scores varied less than mean AL scores across these variables.
p≤0.001 based on adjusted Wald F-test.
NH, non-Hispanic.
In multivariate analysis, an adjusted Wald F-test indicated that the age by race/ethnicity interaction terms were significant (F=40.47, p≤0.001; results not shown). Compared to white women 50–59 years old, younger white women had significantly lower estimated AL scores (Table 3). AL scores of white women ≥60 years were not significantly different from scores of white women 50–59 years old. Black women 18–29 years and 30–39 years old had AL scores 37% and 20%, respectively, lower than white women 50–59 years old. However, black women 40–49 years old had AL scores 14% higher than white women 50–59 years old. Black women 50–59 years of age had AL scores 24% higher compared to their white counterparts, and this significant black/white disparity continued through older ages. Mexican American women 50–59 years old did not differ significantly from their white counterparts in the same age group (differences also were not significant for 60+ year olds for Mexican American and their white counterparts; comparisons not shown).
For a 1-unit change in the predictor variable, the estimated AL score is expected to change by a factor of the respective count ratio relative to the reference category, while holding all other variables in the model constant.
p≤0.05; **p≤0.01; ***p≤0.001.
NH, non-Hispanic.
Net of other covariates, higher SES was associated with lower AL scores. Having more than a high school education was associated with a 12% reduction in AL score relative to having less than a high school education, but having a high school education did not confer a significant health advantage. The highest two family income categories of $35,000–64,999 and ≥$65,000 were associated with a reduction in AL score by 7% and 23%, respectively, in comparison to having an income of <$15,000. Nativity status was also a significant predictor of AL score, with foreign-born women estimated to have AL scores 11% less than scores of U.S.-born women. Marital status was not significantly associated with AL score.
Figure 2 displays predicted AL scores based on the negative binomial regression results by age and racial/ethnic groups. Predicted AL scores for all racial/ethnic groups increased with age, leveling off around ≥60 years. In general, black women consistently had the highest predicted AL scores across all age groups, and white and foreign-born Mexican women had the lowest predicted scores. The greatest disparity between black and white women was observed at the 40–49 years category (3.73 vs. 2.66). Moreover, black women aged 40–49 years had higher predicted AL scores than white women aged 50–59 years (3.73 vs. 3.27). At ages 40–49, predicted AL for U.S.-born Mexican and white women diverged, with U.S.-born Mexican women having higher predicted AL than whites. Foreign-born Mexican women had lower predicted AL scores in comparison to U.S.-born Mexican women in all age groups, and this disparity increased with age.
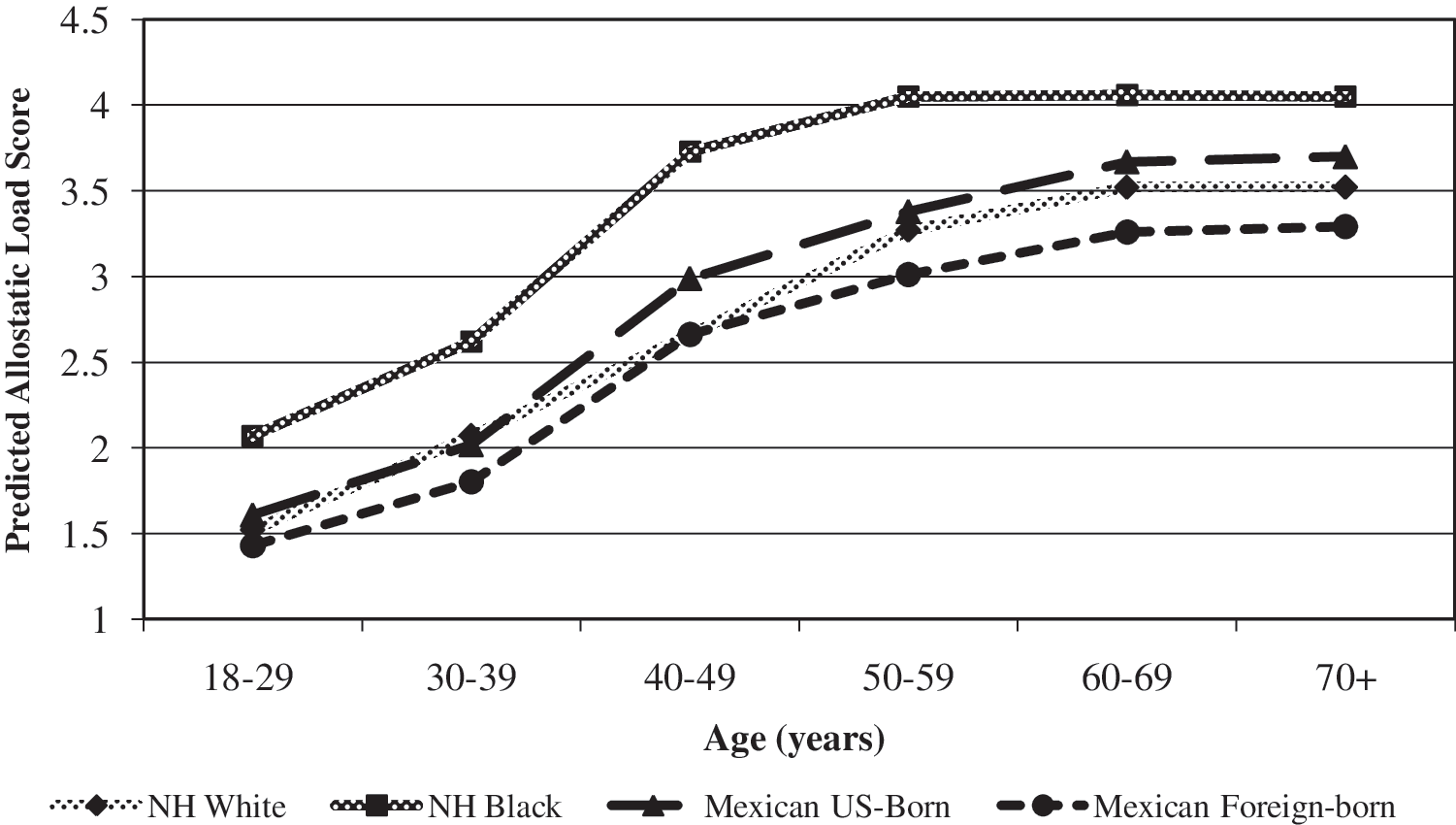
Cross-sectional predicted allostatic load score by age and race/ethnicity, adult women, National Health and Nutrition Examination Survey 1999–2004 (n=5765). NH, non-Hispanic.
Discussion
This study provides one of the first descriptive profiles of the sociodemographic correlates of AL among a nationally representative sample of American adult women. The extensive, nationally representative biomarker data in NHANES are conducive for studying AL and have been used in previous studies to develop AL measures. 20,22,25,27 Another advantage of NHANES is that sample sizes are large enough to allow for meaningful racial/ethnic and age comparisons. As expected, higher AL scores, indicative of greater cumulative biological risk, were observed at older ages, lower SES, and among U.S.-born women and black women. Moreover, black women accrued higher AL at younger ages than women of other racial/ethnic groups. Foreign-born Mexican women had lower AL scores than U.S.-born Mexican women across all age groups.
Not only were black women more likely to have the highest AL scores relative to other racial/ethnic groups in all age groups, but black women 40–49 years old were expected to have AL scores 1.14 times higher than white women 50–59 years old. These results support the findings of Geronimus et al. 22 that black women had significantly higher AL than white women and suggest earlier aging and health deterioration among black women. One possible explanation is the weathering hypothesis, which posits that blacks experience earlier aging from the cumulative impact of racial and gender discrimination, socioeconomic disadvantage, and political marginalization over the life course. 22,58 The repeated experiences of social and economic adversity among racial/ethnic minorities, especially black individuals, over the life course are theorized to elicit chronic stress responses, increase cumulative physiological burden, and accelerate aging processes. 22 Studies have shown that black individuals exhibit AL, morbidity, 59,60 and mortality rates 61 typical of older white individuals. AL provides insight into possible physiological pathways by which these social influences get under the skin, impact biological processes, and eventually manifest as disease and disability. The persistent black/white disparity in AL across all age groups observed in this study suggests that black women are already at a significant health disadvantage in early adulthood, and this pattern persists over the life course, with particularly pronounced black/white disparities by midlife.
U.S.-born Mexican women had higher predicted AL than foreign-born Mexican women in all age groups. Furthermore, predicted AL scores for foreign-born Mexican women were comparable or lower than predicted scores for white women in all age groups. These results are consistent with prior research findings of health and mortality patterns reflecting selective in-migration of healthy individuals and out-migration of sick individuals among U.S. Mexicans 62,63 and confirm the findings of Crimmins et al. 25 of a foreign-born advantage in biological risk profiles among Mexican men and women in the United States. Our findings also support Peek et al., 24 who reported that foreign-born Mexicans from a sample of men and women in Texas had lower scores of AL compared to U.S.-born Mexicans. In addition, results from our study demonstrated that nativity status differences in predicted AL scores for Mexican women increased with age, suggesting that the foreign-born health advantage is particularly salient among older individuals. This may be caused by AL accumulating with age, resulting in more pronounced nativity status difference at older ages. Our finding is consistent with the study by Kaestner et al. 23 in which being foreign-born was more strongly associated with lower AL among older Mexican immigrants than among younger Mexican immgrants and compared to U.S.-born counterparts, although this health advantage was attenuated with time spent in the United States. These combined findings underscore the importance of differentiating nativity status to account for selection effects and significant heterogeneity between U.S.-born and foreign-born groups. With Mexican and other Hispanic groups being among the fastest growing demographic groups in the United States, 2 further research is needed on migration experiences, acculturation, behavioral factors, social structures, and sources of stress specific to nativity status and how they contribute to increasing burden of cumulative biological risk.
Limitations to this study must be acknowledged. First, the data used in this study are cross-sectional and thus limit interpretation of results to be descriptive and associative. Furthermore, the cross-sectional nature of the data presents selection issues; selectivity becomes greater with older age, as the healthiest remain in the population and the sickest people die. The cross-sectional nature of the data also precludes examination of longitudinal AL trajectories over the life course. The biomarkers included in measures of AL, while guided by theory and previous research on AL, were limited by availability in the dataset and did not include markers of neuroendocrine system functioning and other primary mediators that would help provide a more nuanced characterization of AL, particularly those reflecting the HPA axis. In this study, all biomarkers were given equal weight, although it is likely that risk factors contribute differentially to multiple health outcomes across different sociodemographic groups and at different life stages. 64 Evidence suggests, however, that if equal weighting of biomarkers does not reflect physiological reality, it may still provide a conservative estimate of the association between AL and health outcomes. 16 Another limitation of this study is that AL scores were created using cutoff points indicating the traditional high-risk end of the distribution (75th or 25th percentile). It is possible that for some biomarkers, having a value at the other end of the distribution may also confer disease risk. Finally, this study does not include psychosocial variables (e.g., social support, locus of control, optimism) or health behaviors (e.g., healthcare visits, physical activity, smoking) that may mediate or modify the association between sociodemographic variables and AL.
The rapidly increasing integration of biomarker data into large, population-based studies holds many exciting avenues for future research aimed at better understanding how health disparities are formed. Additional research should explore differential weighting and subscales of biomarkers to disentangle the underlying dynamics of individual systems and biomarkers that comprise AL. 27 Heterogeneity of cumulative physiological dysregulation in response to socioenvironmental challenges can be explored by constructing subscales of biomarkers as well as composite summary measures, such as AL, and then comparing patterns across different age, racial/ethnic, or SES groups. Different criteria for high risk also need further development and examination, including existing standardized clinical cutoff points, standardized subclinical cutoff points, and age-specific and gender-specific cutoff points that can be applied to different samples. By examining a nationally representative sample of women, this study is an important first step toward developing gender-specific cutoff points for high risk. Further research on potential mediators, such as pyschosocial factors and health behaviors, on the association between sociodemographic characteristics and AL will also have important implications for specific issues that health interventions target.
Conclusions
This study provides a useful description of associations between major sociodemographic factors and AL among a nationally representative sample of women, focusing on racial/ethnic differences in age patterns of AL and nativity status. AL is an emerging construct that contributes to our understanding of how social factors impact physiological functioning and shape health and aging disparities, particularly along gendered and racial/ethnic lines. Developing AL as a construct and refining measurement has potential utility for informing clinical applications as well as policy-making aimed at eliminating health disparities among women and high-risk groups.
Footnotes
Acknowledgments
This research was funded by the University of California Dissertation Year Fellowship (Dr. Chyu) and NIH grant AT002156 (Dr. Upchurch).
Disclosure Statement
The authors have no conflicts of interest to report.