
Abstract
Background:
In the last decades, several surgical approaches have been used to improve the appearance and quality of life of female Poland syndrome patients. The aim of this study was to analyze the women's quality of life and long-term outcome after breast reconstruction.
Methods:
Forty-nine women with Poland syndrome who were treated surgically between 1974 and 2007 received standardized questionnaires to evaluate their quality of life and satisfaction after surgical treatment.
Results:
Patient response was 65%, with 32 completed questionnaires by 16 women who had pedicled latissimus dorsi myocutaneous (LDM) flaps, 12 with tissue expander or silicone implants, and 4 who had free transverse rectus abdominis myocutaneous (TRAM) flaps. Of these patients, 16 were satisfied or highly satisfied with their postoperative appearance (13 with LDM, 2 with prosthesis, and 1 with TRAM), 16 patients would recommend the same surgery to others under similar circumstances (10 with LDM, 5 with prosthesis, and 1 with TRAM), and 18 patients would choose the same method again (14 with LDM, 3 with prosthesis, and 1 with TRAM).
Conclusions:
In our study, we found that satisfactory outcome in breast reconstruction was achieved particularly when using the LDM flap, which remains the only method that recreates the anterior axillary fold. Future studies on reconstruction methods with autogenous tissue (e.g., TRAM, deep inferior epigastric perforator [DIEP] flap) are needed, however, to analyze quality of life and long-term outcome in patients with Poland syndrome.
Introduction
Poland syndrome was first described by Alfred Poland in 1841. 1 In this syndrome, there is unilateral hypoplasia or absence of the pectoral major muscle, especially its sternocostal head, sometimes accompanied by ipsilateral upper limb deformities. 1 The original definition has been extended to include malformations of minor or absent breast tissue, nipple-areola complex or forearm hypoplasia, brachydactyly, microdactyly, and frequent ribcage deformities. 2 Patients with isolated malformations of the pectoral major muscle are in the minority. 3,4 Some reports note other associated muscle hypoplasia, including that of the pectoral minor, the latissimus dorsi, and the serratus anterior muscles, affecting patients' health and surgical reconstruction possibilities. 5 –7 According to the anatomical variety and individual features of Poland syndrome, the incidence ranges from 1/7,000 to 1/100,000, with a male/female ratio of 2:1 to 3:1. 3 In 1977, Mühlbauer and Wangerin 8 described the so-called Amazone syndrome, which includes unilateral breast hypoplasia in addition to the symptoms of Poland syndrome. These patients suffer from an anterior thoracic asymmetry, with lacking breast volume, varying among mild, moderate, and severe.
In the last decades, several surgical approaches have been used to improve the appearance and quality of life of patients with Poland syndrome, especially those with heavy psychologic and physical burdens. 9 –14 The are several varieties of breast and thoracic wall malformations that aggravate, limit, and even reduce surgical reconstruction. The current trend is to use autogenous tissue for breast reconstruction in Poland syndrome patients. The latissimus dorsi myocutaneous (LDM) flap, pedicled or free, has provided the most satisfactory results, according to both patients and surgeons. In this study, we evaluated the quality of life and long-term outcome after surgical reconstructive procedures in female Poland syndrome patients.
Materials and Methods
This was a retrospective study at the Clinic for Plastic Surgery and Hand Surgery at the Technische Universität München in Germany. Patient satisfaction with the long-term results were evaluated using questionnaires, followed by clinical examination. Forty-nine female patients with Poland syndrome obtained surgical treatment between 1974 and 2007. These patients were requested in writing to participate in our study, and the questionnaires were mailed to them. Patients received a number to guarantee anonymous survey responses and to differentiate responders from nonresponders. To maximize the respond rate, nonresponders were contacted twice by phone and received a second copy of the questionnaires.
The questionnaires
For an objective evaluation, two testing instruments were used—the standardized self-assessment test on life satisfaction (FLZM) by then rich and Herschbach 15 and a self-developed questionnaire established in our preliminary studies—evaluating demographic details, sources of information for breast reconstruction, reasons for seeking the operation, patient satisfaction with appearance, and patient satisfaction with the postoperative outcome. 16 –18 The questions on the self-developed questionnaire were divided into multiple choice, open-ended, and those in which patients described several aspects of their life and their appearance using scales from 1 to 10.
The FLZM 15 has proven validity, is standardized for German-speaking countries, and evaluates subjective quality of life (weighed satisfaction). The questionnaire consists of two modules, general life satisfaction and satisfaction with health, containing 8 items each. Subjects rate every item first for its subjective importance and second for its subjective degree of satisfaction on a 5-point scale (not important/not satisfied=0, rather unimportant/unsatisfied=1, rather important/satisfied=2, quite important/satisfied=3, very important/satisfied=4). The general section consists of eight areas: friends/acquaintances, leisure time/hobbies, health, income/financial security, occupation/work, housing/living conditions, family life/children, partner relationship/sexuality, and one additional question on global satisfaction. The health section evaluates physical condition/fitness, ability to relax/stay on an even keel, energy/zest for life, mobility, vision and hearing, freedom from anxiety, freedom from aches and pains, and independence from help/care.
Because for every individual each aspect of life has different importance, the influence on quality of life is variable. Therefore, weighting is necessary and is done subjectively by the individual. 19 To gain such a weighed satisfaction (wS), Herschbach and Henrich applied a specific formula:
with both ratings made on a scale of 0–4. 15 This method avoids negative and positive effects by any unimportant area of life, and the sum of I*S values is calculable for each module. 19,20 The results of the FLZM were adapted to a control group representing the German healthy population consisting of n=2534 for the module general satisfaction and n=2218 for the module satisfaction with health. 21 For this evaluation, the unpaired t test was used. For all statistical analysis, the software SPSS 11.5 for Windows (SPSS Inc., Chicago, IL) was used. The data distribution of each variable was evaluated using the one-sample Kolmogorov-Smirnov test, and for all tests, the overall statistical level of significance was set at p<0.05.
Results
Patient response was 65%, with 32 completed questionnaires. The age range was 4–28 years (mean 18 years), and patients' age at the time of reconstruction was between 14 and 56 years (mean 25 years). The Reasons for the 65% patient response were change of address and name and refusal to participate. The women in our study suffered only from breast malformations, and none of them had upper limb deformities. In 56% (n=18), the right breast region was affected, and 44% (n=14) had malformed left breasts. In order to analyze the optimal breast reconstruction method in female Poland syndrome patients, we separated the patients into three subgroups according to the applied surgical method: 48% (n=16) received a pedicled LDM flap for breast reconstruction combined with tissue expander and silicon implant or contralateral reduction mammaplasty (Figs. 1 and 2), 39% (n=12) underwent surgical treatment using silicone implants alone or combined with additional previous tissue expansion, and 13% (n=4) received a free transverse rectus abdominis myocutaneous (TRAM) flap.

Patient with moderate right breast deformity characterized by lack of the pectoral major muscle and breast aplasia. Reconstruction of the breast was achieved by a pedicled latissimus dorsi myocutaneous (LDM) flap and a silicon implant after tissue expansion. (
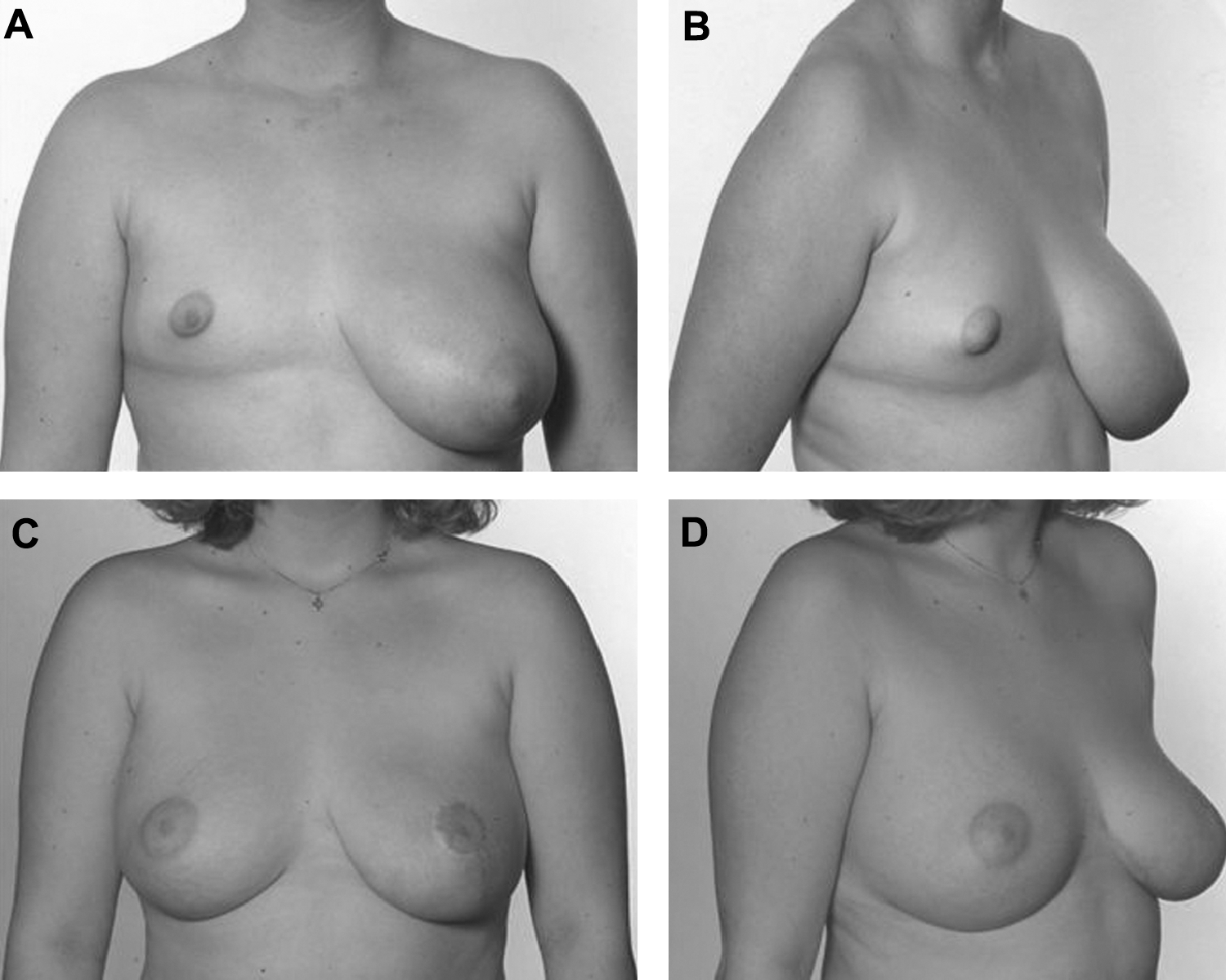
This patient suffered under a mild degree of Poland syndrome, with the right breast and pectoral major muscle hypoplasia covered by subcutaneous tissue and a ptotic left breast. (
Evaluation of self-developed questionnaire
The self-developed questionnaire was divided into multiple choice and open-ended questions and those in which patients described several aspects of their life and their appearance using scales from 1 to 10. A score of 10 indicated the best possible satisfaction, a score≥7 indicated satisfaction, and a score<7 indicated lack of satisfaction. The results are summarized in Table 1.
LDM, latissimus dorsi myocutaneous flap; TRAM, transverse rectus abdominis myocutanoeus flap.
The main reason for seeking breast reconstructive surgery in our study for the majority of the patients (86%) was to improve the physical appearance instead of feeling malformed. Additionally, all patients also underlined the psychologic aspects (loss and lack of self-confidence, self-esteem, sexual and female attractiveness, and social isolation), which were important factors in the decision in favor of having reconstructive surgery (Table 1). All women considered their breast either important or very important to the attractiveness of their body and their female appearance. They reported difficulty in choosing the right clothes to cover the malformation. After surgery, 86% (n=28) felt more satisfied with their appearance when dressed than when undressed. The remaining 14% (n=4) were similarly satisfied both undressed and dressed (Table 1).
Women's satisfaction with the postoperative outcome was divided according to different aspects: total result of breast reconstruction, color, shape, and aesthetic outcome, as well as symmetry, tissue texture, and softness of the reconstructed breast (Table 2). Fifty percent (n=16) were satisfied or very satisfied (Figs. 3 and 4) with the postoperative outcome (LDM=13, prosthesis=2, TRAM=1). The remaining 50% (n=16) were unsatisfied with the surgical outcome (LDM=3, prosthesis=10, TRAM=3). The unsatisfied 50% all judged their satisfaction with low scores but declined further corrective interventions. Of the women, 5% (n=18) would choose the same operation again (LDM=14, prosthesis=3, TRAM=1), and the remaining 43% (n=14) would not choose the same operation again (LDM=2, prosthesis=9, TRAM=3). Under similar circumstances, 50% (n=16) would recommend the same operation to others (LDM=10, prosthesis=5, TRAM 1), and the remaining 50% (n=16) would eventually recommend the same operation to others (LDM=6, prosthesis=7, TRAM=3).

Comparison of the weighted satisfaction difference for each item between the study group and the control group for the module, general life satisfaction. The sum score for both study groups showed no significantly higher quality of life compared to the control group (significant difference at *p<0.05, unpaired t test).

Comparison of the weighted satisfaction difference for each item between the study group and the control group for the module, satisfaction with health. The sum score for both study groups showed significantly higher quality of life compared to the control group (significant difference at *p<0.05, unpaired t test).
Score of 10 indicates best possible satisfaction, a score of ≥7 indicates satisfaction, and a score<7 indicates lack of satisfaction.
Evaluation of FLZM questionnaire
We calculated the weighted satisfaction for each item and achieved the sum scores for the whole Poland study group of the two modules, general life satisfaction (Table 3) and satisfaction with health (Table 4) and compared the scores of our Poland study group with those of a control group. For the first module, general life satisfaction, there was a significant difference in quality of life after breast reconstruction not only within the individual aspects but also for the sum score (Table 3). For the second module, satisfaction with health, we found no significance only for the item, ability to relax (p=0.125); the other items and the sum score showed a significant difference (Table 4).
Significant difference at p<0.05, unpaired t test.
SD, standard deviation.
Significant difference at *p<0.05, unpaired t test.
Because the results of the self-developed questionnaire showed higher satisfaction rates for the LDM flap reconstruction, we further divided the Poland study group in two groups: LDM flap reconstruction and other methods (prosthesis and TRAM) We again calculated the weight satisfaction for each item and the sum score for both groups (LDM and other methods) for the two modules, general life satisfaction (Fig. 3) and satisfaction with health (Fig. 4) and compared the scores with those of the control groups. For the first module, general life satisfaction, only the LDM group showed significant differences with the items, friends and hobbies (both p<0.05, unpaired t test). All the other items and the sum score showed no significant difference in quality of life after surgery compared to the control group (Fig. 3). For the second module, satisfaction with health, we found significant differences with the following items for the LDM group: mobility, vision and hearing, and independence from help and for the sum score (all p<0.05, unpaired t test). Other methods showed significant differences with the items: vision and hearing, and independence from help and for the sum score (all p<0.05, unpaired t test). However, the evaluation of the scores demonstrated a higher subjective satisfaction of Poland syndrome patients compared to the normal population. This impressive feature could be explained by the well-being paradox described by Herschbach. 22 Objectively negative factors in patients' lives have relatively little effect on subjective quality of life.
Discussion
Ascertaining the most beneficial surgical reconstruction method for Poland syndrome patients has the attention of many surgeons, especially because the most affected area of this syndromeis: the female breast. 8 –11,14,23 –26 In the last decades, the LDM flap (pedicled or free) has been established for Poland syndrome breast reconstruction in both genders. 8 –11,14,24 Even the development of autogenous free soft-tissue transfer for breast reconstruction, as used in the TRAM, deep inferior epigastric perforator (DIEP) flap, and other free flaps, 27 has not displaced the LDM flap in the surgical treatment of Poland syndrome patients. The use of autogenous free soft-tissue transfer was introduced to avoid striking scars on the back, implants, and potential capsular fibrosis. However, the beneficial use of the LDM flap has been confirmed, and this method presents the only opportunity to recreate the anterior axillary fold, one of the most conspicuous features of Poland syndrome. 13 Furthermore, the LDM flap provides nearly similar volume to the absent major pectoral muscle. If more volume is required, as in many women, combining the LDM flap with silicone implants is recommended after previous tissue expansion. 14,28
The most common procedure in females is the LDM flap accompanied by expander or silicone implants, eventually followed by a contralateral reduction mammaplasty. If fully developed, a pedicled ipsilateral latissimus dorsi muscle is harvested, avoiding the need for microsurgical anastomosis. In case of an absent ipsilateral LDM, a free LDM flap from the contralateral side has to be applied. Drawbacks to this method are increased operating time, the necessary familiarity with microsurgery, and the need for special equipment. Furthermore, to secure a sufficient blood supply, excellent recipient vessels are required, and these do not exist in some Poland syndrome patients because various vessel malformations are described. 3,29 Therefore, other microsurgical reconstruction methods (e.g., TRAM, DIEP) are the second choice.
Our study included 32 female patients, which limited statistical analysis to ascertain the most effective surgical method for breast reconstruction in patients with Poland syndrome, and we have received considerable criticism. We have to underline the rarity of this syndrome, however, and current publications mention only several cases, up to a maximum of 37 cases. 30,31 Additionally, we are not aware of any report that analyzes the long-term outcome and satisfaction of Poland syndrome patients after breast reconstruction.
The purpose of our study was to relate our evolving experience with Poland syndrome breast reconstruction over the last three decades. Regarding satisfaction with the total result, our study found only 3 unsatisfied patients treated with LDM flap; 2 of the 3 women developed breast cancer later, requiring several surgical interventions. We can only assume that this condition could be a reason for their being unsatisfied. Two satisfied patients confirmed the assumption that in minor degrees of Poland syndrome, breast reconstruction using silicone implants obtains only acceptable results. 11,32
We evaluated which patients would choose the same operation again under similar circumstances. Among the LDM flap patients, only the 2 patients who developed breast cancer would decline the operation rather than having surgery again. Three women with minor manifestations of Poland syndrome who had silicone implants for breast reconstruction would choose the same operation, whereas those patients with more severe features of Poland syndrome who had prosthesis reconstruction would refuse the same operation. In our experience, breast reconstruction in moderate or severe Poland syndrome patients using tissue expansion and silicone implants leads to poor operative outcome; therefore, we would consider this procedures only as second choice.
We have to consider our study results in the context of breast reconstruction history. In the 1970s early 1980s, the LDM flap represented an absolute method for surgical correction in Poland syndrome; in the 1980s and 1990s, additional reconstructive methods (TRAM and DIEP) were established. The patients in our study underwent surgical reconstruction between 1974 and 2007. During this time, according to our results and patient report, the method of first choice was the LDM flap. We will continue our studies to determine if there are changes in patient satisfaction according to the advancements in breast reconstructive surgery.
We achieved unexpected results regarding patients' opinions on recommending the applied method to other patients. Despite their satisfaction with the postoperative outcome and the decision to choose this procedure again, only 10 LDM flap patients would recommend the same surgery to others under similar circumstances. This should increase awareness of a notable psychologic impact of breast reconstruction using the LDM flap; patients require psychologic balance to overcome surgery and the encountered complications. Seven unsatisfied patients with a prosthesis and 3 patients who received a TRAM flap for breast reconstruction would not recommend surgery to others. Further, these patients declined additional corrective interventions to improve their appearance.
Our study exposed higher scores of life satisfaction in the patients who received LDM flaps and patients who did not receive LDM flaps in relation to the normal population. Comparing the groups with each other, we found no significant results. However, we observed higher scores of LDM flap patients compared to non-LDM flap patients in regard to general life satisfaction and health-related satisfaction. Thus, the well-being paradox 22 appears to exist after surgical treatment even in Poland syndrome patients.
In contrast to other women who desire breast reconstruction (e.g., mastectomy patients), female Poland syndrome patients live with their malformation to some degree from their early childhood. The problems increase, especially in adolescence, leading to social marginalization. 27 A large number of publications in recent years dealt with patient satisfaction after breast reconstruction. 17,18,33 –39 The generally accepted consensus is that autogenous breast reconstruction achieves significantly higher patient satisfaction than prosthesis-based reconstruction. 18,34,38,39 Our preliminary work showed that both reconstruction groups (autologous tissue and expander/implant) have equal quality of life sum scores compared to the healthy control group. 18 Our study confirms both of these findings because not only do LDM patients have higher satisfaction scores than those with prosthesis-based reconstruction but also both groups (autologous tissue [LDM and TRAM] and prosthesis) showed higher quality of life after surgery than the control group. Both Saulis et al. 34 and Spear et al. 35 included LDM flaps in their outcome analysis of breast reconstruction and showed that LDM reconstruction is less satisfying than TRAM flap reconstruction even though these results were not statistically significant. Yueh et al. 39 showed that LDM flap reconstruction provides significantly lower general and aesthetic satisfaction than abdominal-based flaps. It is well established that breast reconstruction patients have high levels of patient satisfaction. 36,38
At the current time of modern reconstruction techniques (e.g., free perforator flaps), outcomes research is more important than ever because in times when cost-effectiveness plays a key role in daily clinical routine, sophisticated outcomes research will provide patients and surgeons with transparent and objective knowledge to guide a more reliable decision making process. There are a number of limitations to our study. One limitation is responder bias, as it is possible that only highly satisfied or unsatisfied patients responded. We tried to reduce responder bias by reminding nonresponders twice by phone and mailing them an identical copy of the questionnaire. A second limitation is selection bias because patients could not be randomized to the type of reconstruction they received. Surgical techniques developed over the time, and patients from 1974 to 2007 were included in our study. Plastic surgeons have different preferences, and such preferences change over time. Older surgeons probably prefer other techniques than younger surgeons who are more familiar with modern reconstruction techniques. Furthermore, in retrospective studies, recall bias exists as patients try to remember the details of their surgery, especially with a mean follow-up of 18 years; this study is susceptible to recall bias.
Conclusions
Our study found the most promising results with the use of the LDM flap in female Poland syndrome breast reconstruction. The LDM volume is almost sufficient to match the lacking muscle volume. If breast volume is too small intraoperatively, tissue expansion or silicone implants or both could be necessary to achieve symmetry. The LDM flap enables the surgeon to reconstruct the anterior axillary fold, one of the most conspicuous features of Poland syndrome patients. Females with mild malformations, however, benefit from silicone implants alone because the postoperative outcome is acceptable and the surgical burden is smaller compared to those of other methods (LDM flap, tissue expansion, free flaps). Future studies are necessary to prospectively investigate modern surgical techniques for breast reconstruction in patients with Poland syndrome to understand the different components that improve the quality of life.
Footnotes
Acknowledgments
This work was presented, in part, at the 14th International Congress of the International Confederation for Plastic, Reconstructive and Aesthetic Surgery (IPRAS), June 26–30, 2007, Berlin, Germany.
Disclosure Statement
The authors have no conflicts of interest to report.