
Abstract
Background:
Many pregnant women continue to drink alcohol despite clinical recommendations and public health campaigns about the risks associated with alcohol use during pregnancy. This review examines the predictors of prenatal alcohol use, with the long-term goal of developing more effective preventive efforts.
Methods:
A literature search of several databases for relevant articles was undertaken. Studies were included if they occurred in the context of antenatal care, collected data during the woman's pregnancy (between 1999 and 2009), investigated predictors of any drinking, had a population-based orientation (e.g., did not focus only on high-risk drinkers), and were published in English in a scientific peer-reviewed journal between 1999 and 2009.
Results:
Fourteen studies published between 2002 and 2009 fulfilled the inclusion criteria (United States, 4; Europe, 4; Australia and New Zealand, 3; Japan, 2; and Uganda, 1). The predictors of prenatal alcohol use most consistently identified were prepregnancy alcohol consumption and having been abused or exposed to violence. Less consistent predictors of drinking during pregnancy were high income/social class and positive dependence screen. Unemployment, marital status, and education level were examined in many studies but found to be predictive only infrequently.
Conclusions:
Women's prepregnancy alcohol consumption (i.e., quantity and frequency of typical drinking) and exposure to abuse or violence were consistently associated with drinking during pregnancy. Antenatal care providers should assess these factors for improved detection of women at risk for alcohol-exposed pregnancies.
Introduction
Alcohol use during pregnancy has been linked to numerous adverse health consequences for the developing fetus, including intrauterine growth retardation (IUGR), low birth weight, learning disabilities, behavior problems, and fetal alcohol syndrome. 1 –4 Even fairly small amounts of alcohol have been found to cause adverse neurobehavioral effects, many of which cause lifelong disabilities. 5 –7 There is no universally safe level of alcohol consumption during pregnancy.
Many pregnant women continue to drink alcohol despite clinical recommendations and public health campaigns about the risks associated with prenatal alcohol use in many countries. The prevalence of drinking during pregnancy differs among studies and countries: 6% in a study conducted in Sweden, 8 10% in the United States, 9 54% in Ireland, 10 and 71% in Denmark. 11 The wide range of prevalence figures reflect differences in drinking culture and social attitudes toward drinking, as well as differences in study population characteristics and study protocols. Improved identification and intervention with women who drink during pregnancy is highly desirable and could potentially prevent suffering and conserve resources.
Pregnancy may be associated with increased motivation to reduce or eliminate unhealthy behaviors, including alcohol consumption and smoking, because of the desire to have a healthy baby and to avoid risks to one's own health. 6,12 Therefore, the antenatal care setting may be the ideal place to initiate such changes. Despite the obvious potential of alcohol prevention in antenatal care, however, few countries have implemented routine screening of alcohol use by pregnant women or provision of advice to pregnant women about the risks associated with drinking during pregnancy. 13
Among the challenges in effecting routine screening and intervention of prenatal alcohol use is the necessity to identify correctly the women at risk. Pregnant women may not provide accurate self-reports of drinking for a variety of reasons, including social stigma. 14,15 Other predictors of prenatal alcohol use have been described, although it is usually not feasible to explore a wide range of potential predictors in a single study. However, improved knowledge about different risk factors for prenatal drinking could inform and improve preventive efforts in antenatal care. The purpose of this systematic review of studies completed in antenatal care settings is to identify and analyze the importance of predictors of prenatal alcohol use discovered in previous research, with the long-term goal of developing more effective preventive efforts.
Materials and Methods
Inclusion criteria
This systematic review considered studies conducted in antenatal care settings that assessed predictors of pregnant women's alcohol use. The following inclusion criteria were applied:
1. The recruitment of study participants took place in an antenatal care environment, for example, an antenatal care clinic, an ultrasound clinic, or a delivery clinic.
2. Data collection took place during the woman's pregnancy or immediately after delivery.
3. Predictors of any drinking during pregnancy were investigated.
4. The study had a population-based orientation, meaning that data were collected from all (or a subpopulation of) pregnant women during a specific time period. For example, studies that focused only on women identified to be risk drinkers were not included in this review.
5. The study was published in English in a scientific peer-reviewed journal in the last 10 years, 1999–2009.
6. Data were collected in the last 10 years, 1999–2009.
These homogeneous study protocol inclusion criteria were applied to facilitate comparisons of the results and to reduce the risk of methodologic differences being the main reason for different outcomes. Hence, we excluded a few population-based studies that investigated predictors of drinking during pregnancy and some studies that retrospectively obtained data about pregnancy drinking.
Search strategy
To obtain studies for the review, a literature search was undertaken by the first author (J.M.) up to October 2009. The following databases were searched: PubMed, PsycINFO, Scopus, and Web of Science (covering the databases Arts & Humanities Citation Index, Science Citation Index, and Social Sciences Citation Index). An experienced librarian assisted the first author in searching these databases. The search was limited to articles published in English after 1998.
The following search terms were used: alcohol consumption, alcohol drinking, alcohol use, drinking behavior, epidemiolog*, prevalence, statist*, pregnan*, predict*, determin*, correlate*, pattern*, and characteristic*. The database search yielded 317 potential studies. The first author (J.M.) screened the abstracts of these 317 articles against the inclusion criteria to determine which articles were eligible for inclusion. This abstract screening process produced 59 articles potentially eligible for inclusion. These articles were obtained and read in full by the first and last authors (J.M. and P.N.).
The first and last authors also examined the reference lists of the 59 selected publications by hand-searching the articles. This search process identified 4 further articles (i.e., the full text of 63 studies was read). After a review against the inclusion criteria, 14 studies were selected for inclusion in this review. The flow chart in Figure 1 describes the process of identifying the studies that were included.
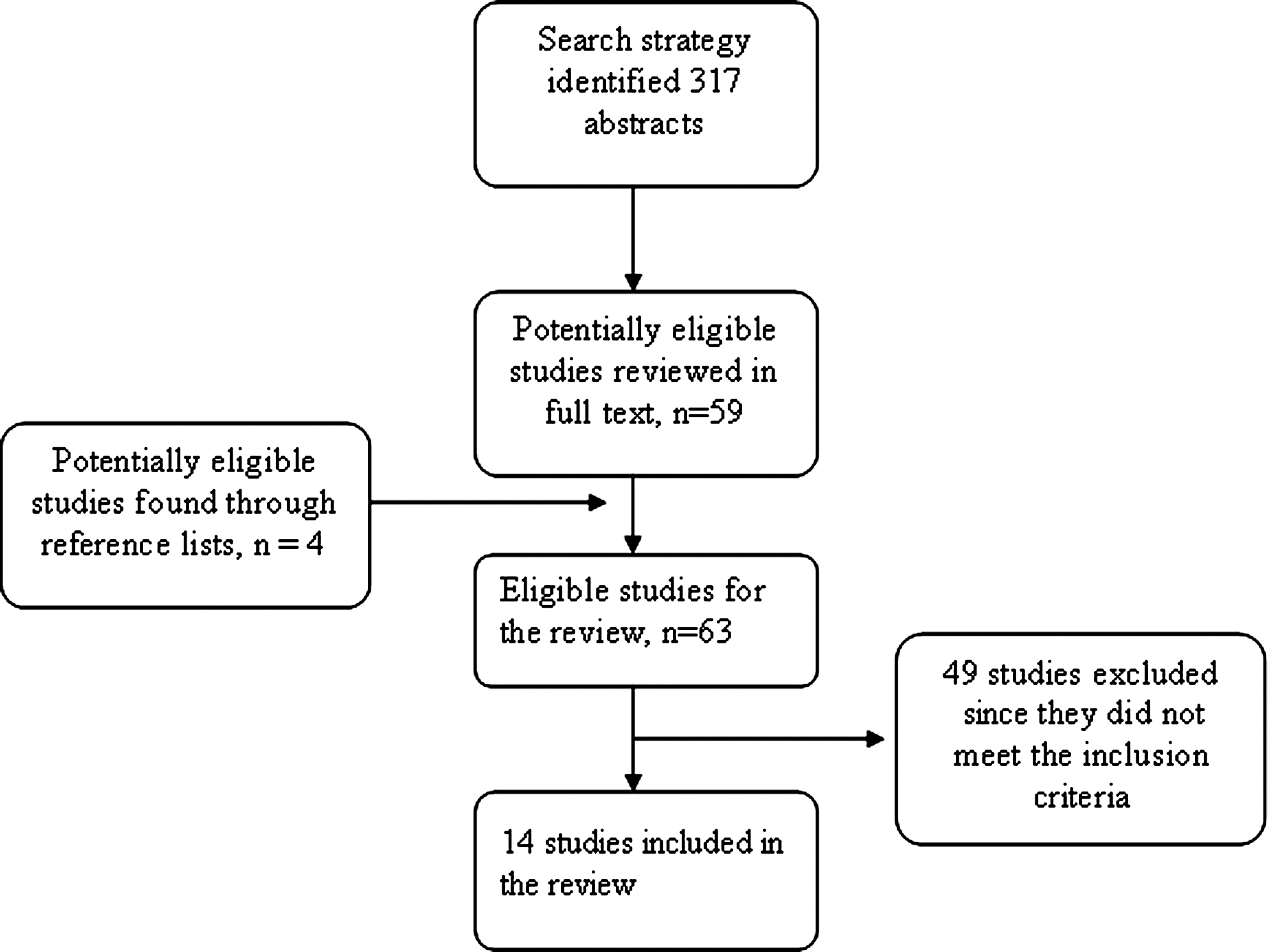
Flow chart illustrating the process of identifying studies that were included.
Data extraction
Data were extracted from the selected studies using a predefined framework that was developed for the study. Data pertaining to the following aspects were extracted from the studies.
Study setting and participants
1. Location
2. Duration and period of data collection
3. Number of study participants and response rate(s)
4. Study participant characteristics
Study protocol
5. Study design
6. Study inclusion criteria
7. Alcohol use measurement instrument
8. Data collection method
9. Measurement point(s)
10. Week(s) of gestation when alcohol use was measured
Study outcomes
11. Factors assessed and identified as predicting drinking during pregnancy
12. Factors assessed but identified as not being associated with drinking during pregnancy
Setting refers to the city or region and the country in which the study was undertaken. Study participation characteristics include the age of the participants, the proportion of women who had their first pregnancy or their first child, and the proportion of women who were married or cohabiting with a partner. The alcohol use measurement instrument is reported as Other if anything other than a validated instrument was used. We also note if alcohol questions were within larger lifestyle-oriented questionnaires. Measures of alcohol consumption (i.e., quantity and frequency) and measures of alcohol problems (symptoms of abuse or dependence) were extracted. Measurement point(s) refers to when data were collected in the study in question (e.g., in a certain week of gestation or during a particular antenatal care visit). Factors identified as predicting drinking during pregnancy in univariate (but not multivariate) analyses are not reported to be predictors of drinking during pregnancy.
Assessment of the methodologic quality
Working independently, the first and last authors (J.M. and P.N.) examined the quality of different methodologic aspects of the included studies. A checklist consisting of 9 questions was used: (1) Did the study fulfill its aim? (2) Were the study population and setting clearly described? (3) Was the recruitment of study subjects clearly described? (4) Was the response rate reported and was it over 70%? (5) Were differences between responders and nonresponders assessed? (6) Was a rationale provided for the chosen outcome measures? (7) Were p values and confidence intervals (CI) reported? (8) Was the alcohol measurement instrument or questions well described and a rationale for the chosen instrument or questions provided? (9) Was the alcohol measurement instrument or questions appropriate?
The methodologic quality was judged as very satisfactory if ≥8 questions were answered positively, satisfactory if >4 questions were answered positively, and unsatisfactory if ≤4 questions were answered positively. The assessments of the first and last authors were compared and discussed before a conclusive quality assessment was made. In all but two cases, the assessments were identical; in the two cases where assessments differed, mutual consensus was reached after discussion.
Results
The main findings of the review are reported in Tables 1 and 2. Table 1 presents key features of the 14 studies included. Table 2 describes the results pertaining to different predictors of drinking during pregnancy.
AUDIT, alcohol measurement instrument, Alcohol Use Disorders Identification Test; AUDIT-C, alcohol measurement instrument, Alcohol Use Disorder Identification Test—Consumption; CAGE, alcohol measurement instrument, Cut Down, Annoyed, Guilty and Eye Opener; I, interview; IAQ, interviewer-administered questionnaire; PNQ, prenatal questionnaire; PRO, prenatal risk overview; Q, questionnaire; SAQ, self-administered questionnaire; SD, standard deviation; T1, T2, T3, time points when data were collected; T-ACE, alcohol measurement instrument: Tolerance, Annoyed, Cut down, Eye-opener; TLFB, alcohol measurement approach, Timeline Follow Back; TWEAK, alcohol measurement instrument, Tolerance, Worried, Eye-opener, Amnesia, Cut down; WIC, Women, Infants, and Children.
The relation between pregnancy drinking and having a partner who drinks alcohol was assessed in two studies and both found a positive association. 20,23 Previous pregnancy losses were assessed in two studies; one of the studies 20 found this factor to be associated with more drinking during pregnancy, but the other study 27 did not find any associations between previous adverse perinatal outcome and pregnancy drinking. Sleep duration/difficulty sleeping was assessed in two studies, in which one found an association 26 and the other did not. 27 Factors investigated in one study each and found to be associated with pregnancy drinking were (1) partner with university education, 16 (2) lack of transportation (used by the authors as a proxy for extreme poverty or social isolation), 18 (3) attending semiprivate antenatal clinic (rather than public clinic), 10 (4) nausea, 23 (5) drug use before pregnancy, 20 (6) midpregnancy intention to drink, 28 and (7) having a religion that does not prohibit alcohol consumption. 23 Factors assessed in one study each and not found to be associated with drinking during pregnancy were (1) access to telephone, 18 (2) food insecurity, 18 (3) housing instability, 18 (4) involvement in child protective services, 18 (5) years of living in the United States, 24 (6) having legal problems, 18 (7) if the pregnancy was planned or not, 28 (8) closeness to partner, 16 (9) loneliness, 16 (10) social support, 18 (11) reproductive and medical history, 23 (12) date of pregnancy confirmation, 28 (13) restless leg syndrome, 26 (14) previous or earlier medical problems, 19 and (15) self-rated health. 20
Quality assessment
The quality of all 14 studies was satisfactory or very satisfactory; hence, no study was excluded from the review because of unsatisfactory quality. Five studies were judged to have very satisfactory quality (1 study 25 had positive answers on all 9 questions, and 4 studies 16,17,18,28 had 8 positive answers). The other 9 studies were judged as being of satisfactory quality.
Inadequate assessment of potential differences between responders and nonresponders was the most common quality problem identified in the studies. Only 2 of the studies 21,24 reported on this. Two studies 20,22 did not include any details about the response rates. In 3 of the studies, 10,19,21 the alcohol measurement questions used were insufficiently described or not explained.
Study setting and participants
The 14 studies were conducted worldwide: 4 studies were carried out in the United States, 18,20,22,24 2 in Australia, 19,28 2 in Japan, 26,27 and 1 study each in Ireland, 10 New Zealand, 21 Norway, 16 Spain, 25 Sweden, 17 and Uganda. 23 The duration of the data collection period ranged from 2 weeks in 2 studies to 55 months in 2 studies. Five of the studies were conducted at a single antenatal care clinic, 10,16,17,23,25 and 8 studies were multicenter studies 18 –20,20,24,26 –28 involving between 2 and 344 clinics. One study 21 did not report if it was conducted at one or multiple centers or clinics. The number of study participants ranged from 548 to 1510 in the single-clinic studies and from 248 to 18,965 in the multicenter studies.
When reported, the mean age of the participants in the studies ranged from 22.6 18 to 31.9 21 years. Two studies reported median ages of 22 23 and 26.1 24 years, respectively. Another 2 studies 10,19 did not report mean or median age. The proportion of married women ranged from 23% 18 to 96% 28 (including de facto relationships) in the 8 studies that reported this information. The proportion of women who were in their first pregnancy (primigravida) ranged from 27% 26 to 50% 16 (reported in 6 studies), and the proportion of women who had no previous child (primiparous) ranged from 37% 25 to 79% 17 (reported in 3 studies).
Study protocol
A cross-sectional study design was used in 11 studies 10,17 –20,22 –27 . These studies collected concurrent data on the women's drinking during the pregnancy. The other 3 studies 16,21,28 were longitudinal and collected data at more than one time point. The study inclusion criteria were generally heterogeneous when explicitly reported (11 studies). The most common inclusion criteria were the timing of the data collection 22,26,27 (usually during the woman's first or second visit to the antenatal clinic). Other inclusion criteria were the age of the study participants 10,23 (e.g., 16–40), speaking a particular language, 16,23 and living in a certain region. 22,25
Alcohol consumption during pregnancy was measured using questions on generic quantity/frequency in 9 studies. 16,19,21,23,24,25,26,27,28 Two studies used the quantity/frequency part of the Prenatal Questionnaire (PNQ). 20,22 One study used the three-item Alcohol Use Disorder Identification Test-Consumption (AUDIT-C), 17 which includes only the drinking quantity/frequency questions. Another study used the alcohol questions from the Prenatal Risk Overview (PRO). 18 One study did not report which alcohol consumption questions were used. 10 If nothing else is reported in Table 1, the same measurement as used during pregnancy was used to measure prepregnancy consumption in the studies that reported on this.
Five studies screened for alcohol problems during or before pregnancy, using different instruments, which included various criteria for problems related to abuse or dependence. Two studies used the risk factor part of PNQ, 20,22 and one study each used T-ACE 16 (acronym for developing Tolerance, being Annoyed by criticisms of one's drinking, wanting to Cut down on one's drinking, and having an Eye-opener drink in the morning), TWEAK 24 (acronym for Tolerance, Worried, Eye-opener, Amnesia, K/Cut down), and CAGE 23 (acronym for Cutting down, Annoyance, Guilt, and Eye-opener). One further study screened for alcohol problems before pregnancy using the 10-item Alcohol Use Disorders Identification Test (AUDIT), 17 which includes items on alcohol consumption, signs of alcohol dependence, and alcohol-related problems.
Data were collected predominantly by means of self-administered questionnaires answered in the antenatal clinic. This approach was used in 8 studies, 17,19,20,22 –24,26,27 2 studies used postal self-administered questionnaires sent to the women's home, 21,28 and 2 studies used interviewer-administered questionnaires in the clinic. 10,18 One study combined self-administered questionnaires answered in the antenatal clinic with mailed questionnaires. 16 Another study relied on personal interviews conducted in the clinic. 25
Data were collected at different time points. Five studies collected data during the women's first prenatal care visit, 10,18 –20,22 and 2 studies obtained data during the second or a later appointment. 26,27 One study gathered data during the women's last session of parental education. 17 In 1 study, the data collection took place during a specific time of gestation, for example, week 28–34. 23 One study did not specify when during pregnancy the data were obtained. 24 In all longitudinal studies, the data collection took place at two or more different time points during the pregnancy.
Study outcomes
The association between age and drinking during pregnancy was reported in 12 studies, making it the most frequently examined factor. Seven of these studies 16 –18,22,23,25,27 reported that higher age was a predictor of drinking during pregnancy. Five studies 19,20,24,26,28 did not observe statistically significant associations between age and drinking during pregnancy. Education level was assessed in 11 studies, of which 2 25,26 reported that women with less education were more likely to drink than women with higher education. In contrast, another study 27 reported higher education to be associated with more drinking during pregnancy than lower education. Two factors were examined in 10 studies each, previous pregnancies and smoking. Five of the studies investigating the importance of the number of previous pregnancies or children for drinking during pregnancy did not observe any associations. 20,23 –25,28 However, whereas 4 studies 19,21,26,27 found a higher number of children or pregnancies predicted more drinking during pregnancy, the study by Meschke et al. 22 reported that a higher number of previous pregnancies was a predictor for less drinking during pregnancy. Smoking was found to predict drinking in 5 16,18,22,23,26 of the 10 studies that reported on this.
Eight studies assessed the relationship between marital status and drinking during pregnancy. Seven of these studies did not find any significant associations 16 –18,23 –25,28 ; 1 study 22 found unmarried women drank during pregnancy more than did married women. Seven studies assessed if prepregnancy alcohol consumption and employment status were predictors of pregnancy drinking. Prepregnancy drinking was found to be a predictor of drinking during pregnancy in all 7 studies that reported this relation. 16,18,23,25 –28 In 1 of the studies, 25 prepregnancy heavy episodic (or binge) drinking and drinking during weekdays but not weekends were predictive of drinking during pregnancy. Being employed was found to predict drinking during pregnancy in 2 studies. 25,26
Six studies examined potential associations between drinking during pregnancy and the woman being at a specific time in her pregnancy. Higher number of weeks of gestation was associated with drinking during pregnancy in 2 20,22 of the 6 studies that assessed this relation. In the study by O'Connor and Whaley, 24 the opposite was found, that is, lower number of weeks of gestation was a predictor of drinking during pregnancy.
Higher income or higher social class was found to be a predictor of drinking during pregnancy in 4 16,21,25,28 of 5 studies that assessed this factor. “Not having a Community Services Card” was used as a proxy for income in one of these studies. 21 Having a positive screen for alcohol problems with PNQ, T-ACE, TWEAK, CAGE, or AUDIT was found to be a predictor of drinking during pregnancy in 4 of 5 studies that examined screening results as a potential predictor. O'Connor and Whaley 24 found higher TWEAK scores to be a predictor, and Göransson et al. 17 found higher AUDIT scores to be a predictor. Leonardsson et al. 20 and Meschke et al. 22 identified specific factors, such as a history of not remembering things because of alcohol use and a need to cut down on drinking. One study 16 found being T-ACE positive to predict binge drinking but not smaller amounts of alcohol during pregnancy. Namagembe et al. 23 assessed CAGE as a predictor of drinking during pregnancy but did not find any association.
Being abused or exposed to violence was found to be a predictor of drinking during pregnancy in all 3 studies that explored this factor. One of these studies 18 reported that physical or sexual abuse by a person other than the intimate partner was predictive of drinking during pregnancy, whereas the other 2 studies 20,22 did not specify who the perpetrator was. In the study by Meschke et al., 22 the effects of abuse on prenatal drinking were mediated by alcohol risk measures. Psychiatric symptoms, such as anxiety and depression, were assessed in 3 studies and were reported in 2 of them to predict drinking during pregnancy.
Several factors were assessed in only 1 or 2 studies. These are reported in the footnote to Table 2.
Discussion
This study examined predictors of drinking during pregnancy by systematically reviewing 14 international studies conducted in this field. Although the population characteristics and protocols of these studies differed, some predictors were found to be highly consistent. Several sociodemographic factors yielded inconsistent and sometimes contradictory results. Not unexpectedly, higher alcohol consumption before pregnancy was found to predict drinking during pregnancy in all the studies that reported on this factor.
The factor investigated most frequently was age (12 studies). Seven of the 12 studies found higher age to be associated with more drinking during pregnancy. All three European studies 16,17,25 that assessed the relationship between age and drinking during pregnancy identified higher age as a predictor, whereas neither of the 2 Australian studies 19,28 noted an association between these factors. Four of the seven studies that found higher age to be a predictor were conducted at urban clinics, 16 –18,23 whereas the studies that did not observe this association did not describe the setting as urban. Higher social status, measured as income or social class, was the sociodemographic factor that exhibited the most consistent results. Although only reported in 5 studies, 4 of them (80%) found higher income to be associated with drinking during pregnancy. The 4 studies 16,21,25,28 that found an association reported higher mean ages (29.6–31.9 years) than did the study 20 that did not find any association (26 years). Further, all 4 studies that reported higher income or social status to be a predictor collected data late in pregnancy, whereas the study that did not find an association collected data during the first antenatal care visit. Alvik et al. 16 found that higher income was a predictor for drinking after 13 weeks of gestation but not in early pregnancy, which suggests that the timing of the data collection might be of importance when assessing this factor. Previous research has shown that higher alcohol consumption among people with high socioeconomic status is primarily because of frequent light social drinking rather than heavier binge drinking. 29 Higher age, which is likely associated with more years of drinking, can lead to stronger ingrained habits. Habits have been described as a milder form of dependence, being learned sequences of acts that have been repeated until they become more or less automatic responses to contextual cues. 30 A certain degree of repetition or practice is required for a habit to develop, 31 but the association between frequency of behavior and habit strength is not fully understood. 32 Harrison and Sidebottom 18 found that frequency of alcohol use was a key predictor for drinking during pregnancy. Similarly, Göransson et al. 17 found that the question: How often do you have a drink containing alcohol? was by far the most significant item predicting drinking during pregnancy. Palma et al. 25 concluded that drinking during weekdays, but not weekends, predicted drinking during pregnancy, which also suggests that frequency of drinking plays an important part in establishing habits that might be difficult to break.
Higher prepregnancy alcohol consumption measured using questions on quantity and frequency of drinking was consistently identified as a predictor for drinking during pregnancy. All the studies that assessed this factor identified it as a predictor. The scientific literature has provided a solid evidence base that supports the efficacy and effectiveness of relatively brief interventions at reducing hazardous and harmful alcohol consumption in nondependent, nontreatment-seeking patients. 32 As most pregnant women are highly motivated to change their behaviors, 6 it has even been speculated that brief alcohol interventions are even more effective in pregnant populations than in general populations.
Having a positive result from a screen for alcohol problems was found to predict drinking during pregnancy in 4 of the 5 studies that assessed the association. 17,20,22,24 The study that did not find an association for any drinking identified an association between positive score and binge drinking during pregnancy. 16 However, the studies used different screening instruments, which should be borne in mind when interpreting these results. Definitions of dependence include difficulties in controlling use, persistent use despite harmful consequences, 33 and unsuccessful attempts to cut down on drinking. 34 Identification of women who abuse alcohol or who are alcohol-dependent for specialist treatment referral is critically important because these women are likely to have difficulties abstaining from alcohol even despite knowledge about the harmful effects of alcohol intake during pregnancy. Also, these women tend to enter antenatal care later than other women, 5,6 emphasizing the importance of providing them with expert help as soon as possible. Previous research has found simple screening instruments to be effective for detection of women who drink during pregnancy. 35
Being abused or exposed to violence was positively associated with drinking during pregnancy in the 3 studies that examined this association. This finding is consistent with research that has shown that physical violence is associated with more drinking before and during pregnancy. 36 Two explanations have been offered for the drinking-violence link: women self-medicate, that is, use alcohol as a means of coping with the emotional and physical pain caused by violence, or the women's alcohol use triggers violent episodes because their partners or other members of society view the women's behavior as inappropriate or find it easier to gain access to intoxicated women. 36,37 Another possible explanation is that women who drink might also have partners who drink more, and those partners may be more violent because of their drinking. In 1 of the studies, measures of alcohol problems mediated the relation between abuse history and prenatal alcohol use. This indicates that exposure to violence has an effect on prenatal alcohol use only if alcohol is used as self-medication for the effects of trauma associated with the violence. 22 The importance of abuse and violence as predictors for drinking during pregnancy suggests the need for screening for various types of victimization within antenatal care. It is noteworthy that all 3 studies examining this relationship were conducted in the United States.
Psychiatric symptoms, such as anxiety and depression, were found to predict drinking during pregnancy in 2 of the 3 studies that investigated this. The studies assessing anxiety or depression used different instruments to measure these symptoms, which could possibly explain the disparate results. Research into the association between various psychiatric symptoms and alcohol consumption has established that problems related to alcohol use and anxiety and mood disorders tend to occur in the same individuals. 38 Again self-medication is suggested as an explanation. Another causal explanation is that alcohol use serves to promote development of the psychiatric symptoms. 39
Smoking was found to be associated with drinking during pregnancy in half of the studies examining this. We could not find any consistent differences between the studies that reported an association and those that did not find an association in such factors as location and setting of the studies, participant characteristics, study design, data collection method and occasion, or questions on smoking. The co-occurrence of tobacco use and alcohol use is well established. The association has been found among nonpregnant women of fertile age. 40 Other studies 41,42 have found that smokers engage in heavy episodic drinking (binge drinking) more often than nonsmokers. Because smoking, like alcohol consumption, can cause adverse pregnancy outcomes and negative health effects to the fetus, 43 it is of great importance to be aware of the smoking-drinking association in order to enhance the detection and prevention of these risk factors.
This review has some potential limitations that must be considered when interpreting the results. Some of the predictors were investigated in only a few studies, making it necessary to interpret the importance of these predictors with more caution. Small study populations in some studies may also restrict the possibility of identifying statistically significant associations that may have been found in a larger population.
The studies included in the review were conducted around the world. Alcohol consumption and drinking patterns vary greatly between countries and cultures, but the focus of this review was not on the epidemiology of drinking but rather on predictors of drinking during pregnancy. Cultural differences in drinking may have affected the results, as it is possible that the extent to which women report drinking during pregnancy is influenced by cultural norms and acceptability concerning alcohol. Cultural norms regarding drinking tend to be more influential on drinking behavior than do legal restrictions. 44 Sociodemographic differences in general may also have influenced the results, as there are known associations between drinking patterns and such factors as income, education, and social status. 45 Hence, the generalizability of predictors identified in only a few studies may be limited. Some predictors require further investigation to clarify their associations with drinking during pregnancy, for example, maternal age. Another example is that both studies 26,27 that identified an association between pregnancy drinking and higher number of weeks of gestation were conducted in Japan. The study 24 that found the opposite and the studies 20,22 that did not identify this association were conducted in the United States.
The study protocols differed among the studies. For example, data collection took place at different time points in pregnancy, the inclusion criteria differed, and the methods used to collect data varied. Data were collected by means of interviewer-administered questionnaires and self-report questionnaires filled out at the clinic or at home. Different modes of data collection may have impacted the results. Obtaining data through interviews could bias the results because of social desirability effects; that is, the respondents provide the answers they believe make them appear socially responsible with regard to the behaviours and attitudes under investigation. Studies of alcohol consumption that have used face-to-face interviews to gather data have shown lower levels of drinking than self-administered questionnaires. 46 However, the opposite has been found in a study among adolescents; consumption was underreported in questionnaires compared to interviews, although adolescents may differ from pregnant women in terms of what they view as socially acceptable behaviour. 47 These differences might have influenced the prevalence of drinking during pregnancy reported in the studies, but it is unlikely that they would have a significant effect on the predictors. Still, other differences in methodology might have impacted some results. For example, 2 of the studies that reported different results about education 26,27 were conducted in the same country, applied the same alcohol measurement, but used different categorization of years of education.
The review also has considerable strengths. Studies investigating predictors of drinking during pregnancy tend to focus on a few predictors that are believed to be of interest. This review provides information about potentially important predictors for planning preventive work in antenatal care and implementing new routines to identify women who drink during pregnancy. The study findings provide a large sample of international antenatal care populations, reflecting a diversity of women in terms of ethnicities, cultures, age distributions, alcohol policies, and antenatal care systems. Although not all women were asked the same questions, they were all asked about their drinking during (or immediately after) their pregnancy.
Conclusions
On the basis of this systematic review of 14 international studies, drinking during pregnancy appears to be consistently associated with women's prepregnancy alcohol consumption (i.e., quantity and frequency of typical drinking) and exposure to abuse or violence. Antenatal care providers should assess these factors for improved detection of women at risk for alcohol-exposed pregnancies.
Footnotes
Acknowledgments
This review was supported in part by R01 AA 14678 and K24 AA 00289 (to G.C.).
Disclosure Statement
No competing financial interests exist.