
Abstract
Osteoporosis is a serious health concern affecting millions of Americans, with many patients going undiagnosed and untreated. Fractures due to osteoporosis and fracture-related complications are the most clinically relevant and costly consequences of this disorder. The Fracture Risk Assessment Tool (FRAX®), released by the World Health Organization (WHO) in February 2008, is a major achievement in helping determine which patients may be candidates for pharmacological therapy for osteoporosis. This Web-based algorithm, which has been incorporated into some dual x-ray absorptiometry (DXA) reporting software, calculates the 10-year probability of major osteoporotic fracture (clinical vertebral, hip, forearm, or humerus) and the 10-year probability of hip fracture in men and women based on easily obtained clinical risk factors and bone mineral density (BMD) of the femoral neck (optional). The National Osteoporosis Foundation updated its U.S. guidelines in February 2008 to incorporate FRAX and recommends that all postmenopausal women and men aged ≥50 years with a hip or vertebral fracture, a T-score ≤−2.5 at the femoral neck or spine (excluding secondary causes), or low bone mass (T-score between −1.0 and −2.5) and a 10-year probability of hip fracture ≥3% or of major osteoporosis-related fracture ≥20% (based on FRAX) should be considered candidates for drug therapy. Despite its demonstrated clinical utility, FRAX has limitations and should not be used in all situations. Acceptance and clinical use of FRAX may help identify men and women at increased risk for osteoporotic fracture, but implementing the tool into clinical practice may be a challenge for busy physicians.
Introduction
Osteoporosis, a silent skeletal disorder characterized by compromised bone strength, is a serious health concern associated with aging that places both men and women at increased risk for fracture and associated complications. 1 The National Osteoporosis Foundation (NOF) estimates that more than 10 million Americans have osteoporosis and another 34 million have low bone density (T-scores between −1.0 and −2.5). 2 Moreover, approximately 1 of every 2 Caucasian women and 1 of every 5 Caucasian men will sustain an osteoporosis-related fracture during their lifetime. 3 Fractures and fracture-related complications are the most clinically relevant consequences of osteoporosis; 4 the cost of treating osteoporotic fractures in the United States was estimated to be $17 billion in 2005 and is expected to increase by 50% by 2025.
Despite the availability of diagnostic tools and clinical data supporting the importance of preventing and treating osteoporosis, many patients remain undiagnosed and untreated. 5 –9 Although risk factors, such as a family history of osteoporosis, history of prior fracture, and low body weight, are often considered when determining who should be screened or treated for osteoporosis, there is a clear need for a tool that would provide a systematic approach to fracture risk assessment. As the population ages, osteoporosis will likely have an even greater impact on society, emphasizing the increasing importance of a tool that may help identify patients who are more likely to benefit from pharmacological therapy, particularly those at high risk for fracture. An algorithm released by the World Health Organization (WHO) in February 2008, the Fracture Risk Assessment Tool (FRAX®), may prove to be a valuable resource for physicians with patients who may be at risk for osteoporosis and related fractures. Because FRAX is country specific, this review focuses primarily on the clinical application of this algorithm in the United States.
The FRAX Tool: What Is It?
FRAX is a Web-based algorithm (
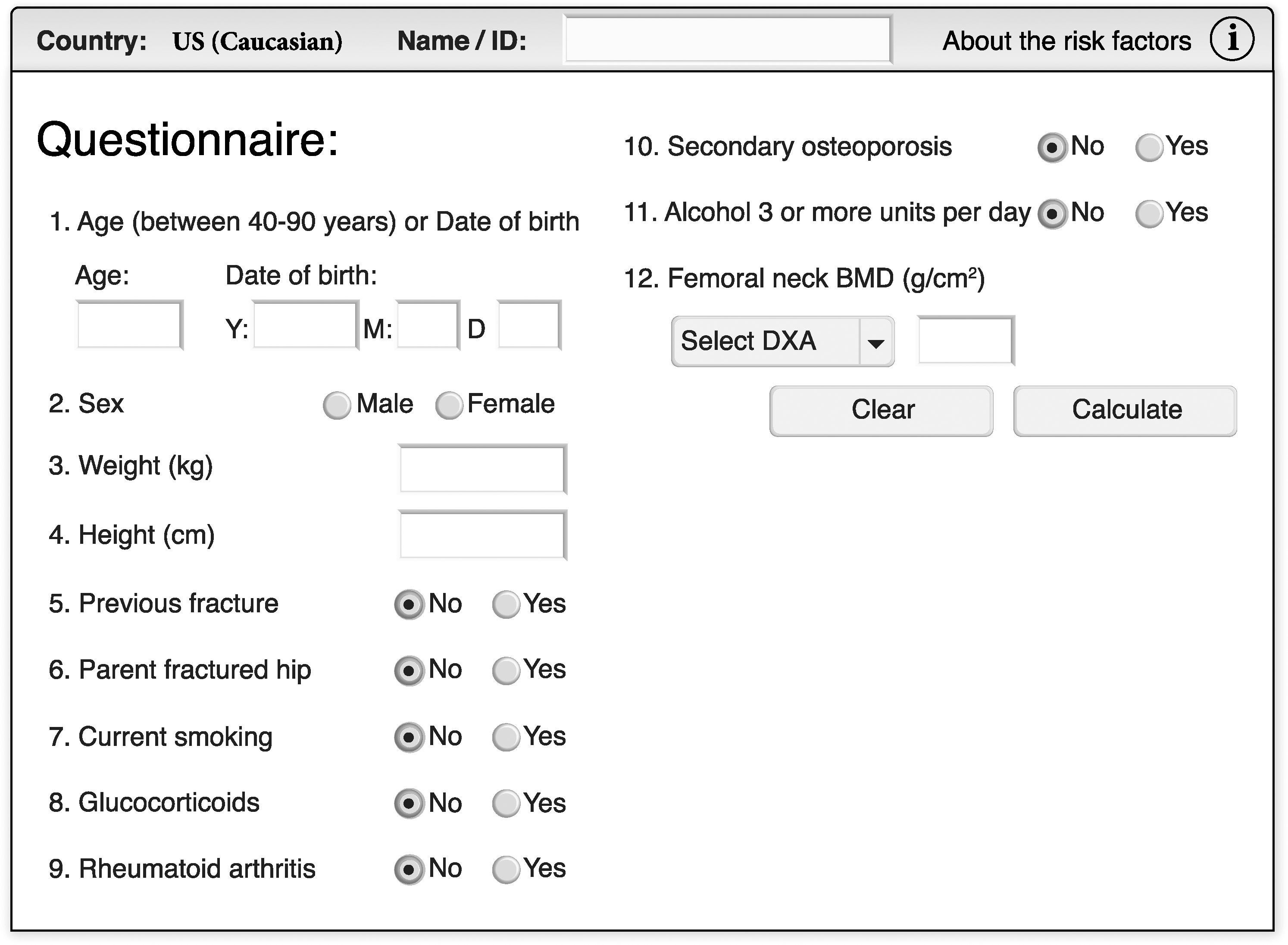
The World Health Organization (WHO) Fracture Risk Assessment Tool (FRAX®) (U.S. version). Image used with permission of the WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield. FRAX is registered to Professor J.A. Kanis, University of Sheffield.
As of August 2010, available for Argentina, Australia, Austria, Belgium, Canada, China, Taiwan, Colombia, Denmark, Finland, France, Germany, Hong Kong, Hungary, Italy, Japan, Jordan, Lebanon, Malta, Mexico, the Netherlands, New Zealand, the Philippines, Singapore, South Korea, Spain, Sweden, Switzerland, Turkey, the United Kingdom, and the United States.
If ages <40 or >90 years are entered, the program will compute probabilities using 40 and 90 years, respectively.
A unit of alcohol is equivalent to a standard glass of beer, an ounce of spirits, or a medium-sized (4-ounce) glass of wine.
Examples include type 1 diabetes, osteogenesis imperfecta in adults, untreated long-standing hyperthyroidism, hypogonadism or premature menopause (age <45 years), chronic malnutrition, or malabsorption and chronic liver disease. This button is disabled after bone mineral density is entered into the model.
As of June 2010, either T-score or femoral neck bone mineral density can be entered.
There are many positive attributes of FRAX. First, probability of fracture can be estimated based on the presence of clinical risk factors in men and women in a wide geographic distribution. This can be done with clinical risk factors alone or in combination with BMD measurement to improve fracture risk prediction. 10 Including BMD increases the sensitivity without decreasing the specificity of the fracture risk assessment. 14,17 Moreover, the model uses primary data to optimize the accuracy of the fracture probability calculation, allowing for determination of the predictive importance of each risk factor in a multivariable context as well as of interactions between risk factors. 11 Because fracture probability varies in different regions of the world, 18 FRAX can be calibrated to the countries for which the epidemiology of fracture and death is known. 11 At present, models are currently available for Argentina, Australia, Austria, Belgium, Canada, China, Taiwan, Colombia, Denmark, Finland, France, Germany, Hong Kong, Hungary, Italy, Japan, Jordan, Lebanon, Malta, Mexico, the Netherlands, New Zealand, the Philippines, Singapore, South Korea, Spain, Sweden, Switzerland, Turkey, the United Kingdom, and the United States. With the most recent version released on August 12, 2010 (FRAX v3.2), the model is now accessible in 14 languages: English, Arabic, Chinese (traditional and simplified), Danish, Finnish, French, German, Japanese, Polish, Russian, Spanish, Swedish, and Turkish. The website was also redesigned to allow more flexibility. In addition, for the U.S. tool only, the potential contribution of ethnicity to fracture risk is considered, with separate models for Caucasian, black, Hispanic, and Asian individuals.
Clinical Applications of the FRAX Tool
Until recently, guidelines for the management of osteoporosis were based primarily on the BMD T-score. Although FRAX does not indicate which patients need to be treated, 19 this tool should be used as part of the decision-making process for individual patients who may be candidates for drug therapy for osteoporosis. Other clinical applications of FRAX include selection of patients for clinical trials of medications to treat osteoporosis and determination of treatment intervention thresholds, which are often based on cost-effectiveness analyses. 15,16,20,21 A few case studies of sample patient scenarios using FRAX to calculate fracture risk are described in Table 2.
Based on current U.S. FRAX calculations (FRAX v3.2).
All examples are based on women with an assumed weight of 60 kg and height of 160 cm.
VFA, vertebral fracture assessment.
Recommendations and guidelines from the National Osteoporosis Foundation and the International Society for Clinical Densitometry
Treatment decisions should be individualized; however, the NOF recommends that in general, men aged ≥50 years and postmenopausal women should be considered for osteoporosis-related drug therapy if they have any of the following: a hip or vertebral fracture (clinical or morphometric), T-score ≤−2.5 at the femoral neck or spine (after appropriate evaluation to exclude secondary causes), or low bone mass (T-score between −1.0 and −2.5 at the femoral neck or spine) and a 10-year probability of a hip fracture ≥3% or a 10-year probability of a major osteoporosis-related fracture ≥20%, based on the U.S. FRAX calculation (Table 3). 4 The intervention thresholds (10-year probability of hip fracture ≥3% or of major osteoporosis-related fracture ≥20%) were determined based on the value of quality of adjusted life-years saved. 22,23
Information based on the National Osteoporosis Foundation. Clinician's guide to prevention and treatment of osteoporosis.4
The NOF updated its U.S. guidelines in 2008 to incorporate FRAX, providing recommendations for its use in clinical practice. As recommended by the NOF, FRAX should be used when the decision to begin pharmacological treatment is uncertain. Patients meeting the following criteria are appropriate candidates for using FRAX to assist with a treatment decision: men aged ≥50 years and postmenopausal women (1) who are not on treatment and who have (2) low bone mass (T-score between −1.0 and −2.5), (3) no prior hip or vertebral fracture (clinical or morphometric), and (4) an evaluable hip for dual x-ray absorptiometry (DXA) study. 4,24 Although BMD is not required for the FRAX algorithm, the NOF recommends using FRAX plus BMD for treatment considerations. If femoral neck BMD is not available, total hip BMD may be substituted, but use of BMD from sites other than the hip is not recommended. 4
It is important when interpreting the results of a FRAX calculation to remember that these fracture probabilities are only as accurate as the risk factor information that is collected and entered into the algorithm. The NOF and the International Society for Clinical Densitometry (ISCD) have provided recommendations for consideration when entering risk factor information into the tool. 24 For example, previous fracture should be checked “yes” if the patient sustained a broken bone after the age of 40 years, excluding fractures of the skull, hands, and feet. Glucocorticoid use should only be checked “yes” for patients having received oral prednisolone 5 mg daily or an equivalent for 3 or more months (current or in the past). Only patients with a confirmed diagnosis of rheumatoid arthritis should receive a mark for “yes” for this risk factor. Although rheumatoid arthritis has been shown to be a risk factor for fracture, osteoarthritis may in fact be protective against fracture.
Based on recent reports by the NOF and the ISCD, FRAX has undergone regulatory review by the U.S. Food and Drug Administration (FDA) for incorporation into DXA scanners to allow a FRAX calculation, if appropriate, at the time of a DXA test in untreated older men and postmenopausal women with low bone mass 25 ; the FRAX reporting software has been released but with limited distribution. To provide assistance with using the FRAX tool and NOF guidelines when manufacturers release FRAX as part of the DXA report, the NOF and the ISCD have developed an optional FRAX filter. 26 This FRAX filter will be a valuable guide that limits when FRAX will be reported. In other words, the FRAX filter would not provide FRAX results in circumstances that are not specified in NOF guidelines (e.g., for patients already on treatment). It is hoped that this filtering mechanism will eliminate situations in which FRAX calculations may contradict NOF guidance, thus minimizing confusion.
Other considerations
In addition to the uses discussed, FRAX can be used dynamically. For example, a 65-year-old woman with a BMI of 23.7 kg/m2 and a T-score of −2.1 has a 10-year risk of hip fracture of 1.8% and risk of major osteoporotic fracture of 11% (based on current U.S. FRAX calculations). If she subsequently acquires a risk factor, such as parental hip fracture, however, her 10-year hip and major osteoporotic fracture risks rise to 1.9% and 20%, respectively. Likewise, if she has a history of previous fracture, her 10-year hip and major osteoporotic fracture risks rise to 3.0% and 18%, respectively. In either case, this patient may be a candidate for osteoporosis-related drug therapy based on NOF treatment guidelines. Similarly, the use of systemic glucocorticoids and a diagnosis of rheumatoid arthritis increase this patient's 10-year fracture risk to 4.7% (hip) and 22% (major fractures). Five years in the future, based on an expected bone loss of approximately 0.5% per year 16 (aged 70 years; T-score of −2.3) and no other known risk factors, this patient's 10-year risk of hip fracture is now 3.1% and of major osteoporotic fracture is 13%. Thus, FRAX can be used in a dynamic fashion to look at future fracture risk as patients' situations change over time.
Clinical studies validating the FRAX tool
Because FRAX has only been available since February 2008, data demonstrating the clinical utility of the tool are limited. Two clinical studies have shown that patients at increased risk for fracture based on FRAX will respond to osteoporosis treatment. 27 –29 McCloskey et al. 27 evaluated the effect of an oral bisphosphonate, clodronate, on fracture rates when risk was calculated using the FRAX algorithm. The efficacy of clodronate was evident in high-risk women, even in the absence of information on BMD. 27 Similarly, Kanis et al. 28,29 evaluated the efficacy of bazedoxifene, a novel selective estrogen receptor modulator (SERM), on fracture outcomes using FRAX, based on data from the pivotal phase III treatment study. Bazedoxifene was shown to significantly reduce the risk of morphometric vertebral fractures, all clinical fractures and nonvertebral fractures relative to placebo in postmenopausal women at or above a FRAX-based probability threshold. 28,29 In a meta-analysis of data from the Multiple Outcomes of Raloxifene Evaluation (MORE) phase III study, treatment with raloxifene significantly decreased the risk of morphometric vertebral fractures and all clinical fractures versus placebo, but there was no significant association between treatment efficacy and fracture probability using the FRAX tool. 30 Whereas these studies support the validity of FRAX, another study has shown that FRAX may not be useful for prediction of treatment-related reduction in fracture risk. 31
Circumstances in which the FRAX tool is not appropriate
Although FRAX is an exciting new development for physicians and their patients, there are situations in which the tool should not be used or in which the results may be misleading (Table 4). As mentioned, FRAX is only applicable to untreated patients. According to the NOF and the ISCD, examples of untreated patients include no hormone, SERM, calcitonin, parathyroid hormone, or denosumab therapy for the past year or no bisphosphonate therapy for the past 2 years (with the exception of oral bisphosphonates taken for <2 months). 24 Calcium and vitamin D do not constitute treatment with respect to use of the FRAX tool. Although it may seem obvious, it is worthwhile to mention that FRAX is unnecessary in patients for whom treatment is clearly indicated. FRAX also may not be appropriate for patients with T-scores better than −1.0, as treatment has not been shown to be effective in this patient population. 16 Again, according to NOF guidelines, FRAX should be used only when a treatment decision is uncertain. Because there is some discrepancy about whether to use FRAX in patients receiving glucocorticoid therapy, this decision is best left to each individual physician. NOF guidelines suggest use of FRAX in these patients, but the American College of Rheumatology recommends pharmacological treatment for the prevention of glucocorticoid-induced osteoporosis in select patient subgroups based on fracture risk (guided by FRAX), dose and anticipated duration of glucocorticoid therapy, and patient age/menopausal status. 32 In addition, there are some diseases or conditions that were not captured in FRAX when it was first developed that would likely have an impact on fracture risk, such as aromatase inhibitor therapy for breast cancer or androgen deprivation therapy for prostate cancer.
Limitations of the FRAX Tool
With FRAX now available for everyday clinical use, it is important to be aware of its inherent limitations, many of which are mentioned on the FRAX website. Some of these limitations are a result of information that was not available in the initial datasets used to develop the algorithm. As an example, dose-response is not taken into account for several of the risk factors, such as type/location/number of fractures, glucocorticoid dose and duration, and smoking and alcohol quantity and duration; instead, the tool assumes average risk, providing risk ratios for an average dose or exposure. 10,11,33 Meanwhile, evidence suggests that fracture risk associated with excess alcohol, cigarette smoking, and the use of glucocorticoids is dose-responsive. 34 –36 Likewise, the number and severity of fractures as well as fracture site affect the risk of subsequent fracture. 15,37,38 Thus, fracture probability may be underestimated for patients having higher than average exposure to glucocorticoids, cigarettes, or alcohol or for patients having experienced multiple prior fractures (likewise, a lower risk for patients whose exposure is less than average). There are also a number of risk factors for fracture that are not incorporated into the algorithm, based on lack of data, including biochemical markers of bone turnover, risk factors for falls, previous exposure to pharmacological intervention, vitamin D deficiency, and physical activity. 11,16,39 Thus, calculated fracture risk using FRAX may be less than the actual risk if some of these other factors are present. As mentioned previously, the BMD input to FRAX is limited to the femoral neck, again based on data taken from the population-based cohorts used to develop the algorithm. 11,13,15 This could be problematic for a patient who may have a low lumbar spine T-score, and thus be at high risk for fracture, but a relatively good femoral neck T-score. 33
Other limitations of FRAX relate to proper interpretation of the various risk factors, as not all risk factors are straightforward. For instance, what constitutes a previous fracture is not clearly defined, and users of the tool may answer “yes” based on fracture sites that are not related to osteoporosis. 33,40 This could lead to an overestimation of fracture risk and perhaps unnecessary treatment. Moreover, secondary causes of osteoporosis are not explained well, 33 and the tool does not allow for combinations of secondary risk factors. 16 For example, a patient may have both hyperthyroidism and malabsorption, but FRAX assigns the same relative risk as if this patient had only one of these conditions. 16 In addition, the algorithm does not take into account both BMD and secondary osteoporosis; if BMD is entered into the model, answering “yes” to secondary osteoporosis does not change the fracture risk calculation. 16 With the exception of rheumatoid arthritis, there is little or no evidence that secondary causes of osteoporosis incur a higher fracture risk than that incurred by loss of BMD alone. FRAX assumes that the effects of secondary causes of osteoporosis on fracture risk are mediated through changes in BMD and, thus, are irrelevant when BMD is entered into the model.
These limitations are important considerations, but perhaps the greatest limitation of FRAX may be that too few physicians are using it routinely to help guide daily decisions about their individual patients.
16
Physicians are unlikely to access a Web-based tool and are often too busy to find time to use it. Case in point, a recent study showed that only 1 in 20 physicians who were asked to access a Web-based fracture risk assessment tool similar to FRAX did so.
41
To expand accessibility of the model to clinical settings without Internet access, an iPhone application was recently launched in partnership with the International Osteoporosis Foundation (
Other Fracture Risk Calculators
Other fracture risk tools have been developed 42 –45 and recently reviewed and compared with FRAX. 46,47 Advantages of some of these tools are the inclusion of other risk factors (such as falls), the addition of fractures other than the 4 major sites used in FRAX, and flexibility with timelines (5-year projections). Some of these tools are useful only for women, and most are only validated for a single country. FRAX is the only risk assessment tool that is calibrated for multiple countries as well as for both women and men.
Conclusions
FRAX is a major achievement for the medical community and is currently the gold standard among fracture models. It is the only model that is derived from extensive databases; it provides validated results for men and women over a large age range and both with or without BMD results. 16 Based on these algorithms, physicians may be able to more accurately determine which patients may benefit from osteoporosis treatment (i.e., those at an increased risk for fracture) as well as those patients who do not need treatment. Recent studies have demonstrated the clinical utility of FRAX in identifying patients at high risk for fracture who were effectively treated with pharmacological therapy (clodronate and bazedoxifene). 27 –29 Moreover, FRAX may be used dynamically to periodically assess fracture risk and the potential need for pharmacological therapy as individual patient circumstances change over time. Despite its proven clinical utility, however, it is important to remember that FRAX has limitations and should not be used in all situations. Whereas acceptance and use of FRAX may help identify and treat men and women at risk for osteoporotic fracture, implementing the tool into everyday clinical practice may still pose a challenge.
Footnotes
Acknowledgments
Medical writing support for this article was provided by Bo Choi, Ph.D., of MedErgy and was funded by Wyeth Pharmaceuticals, Collegeville, PA, which was acquired by Pfizer Inc in October 2009. The author was not compensated and retained full editorial control over the content of the manuscript.
Disclosure Statement
I am the co-founder, stockholder, and director of OsteoDynamics. I have received honoraria for lectures from the following companies in the past year: Amgen, Novartis, Warner Chilcott. I have received consulting fees from the following companies in the past year: Amgen, Arena, Baxter Healthcare, InteKrin, Johnson & Johnson, Eli Lilly, MedPace, Merck, NPS, Orexigen, Pfizer/Wyeth, Takeda Pharmaceuticals, Vivus, Warner Chilcott. Through my university, I have research support from the following companies: Amgen, Merck, NPS.