
Abstract
Background:
Visual inspection with acetic acid (VIA) is a simple, low-cost alternative to traditional Pap smears that could greatly benefit the amount of screening and treatment available in low-resource areas, such as rural El Salvador. The objective of this study was to train Salvadoran health providers in VIA and cryotherapy using a week-long competency course.
Methods:
Health providers participated in the VIA training course, which consisted of 1 half-day of didactics, followed by 4 and 1 half days of clinical training. Pretests and posttests were administered. A 1-day didactic refresher course was administered to assess the quality of services being provided.
Results:
Sixty-eight nurses and physicians completed the training course. Each trainee screened approximately 120 women and performed, on average, seven cryotherapy treatments. The average trainee improved his or her score by 15% on the theoretical test and 16.7% on the image test. At the completion of the 1-day refresher, average test scores were the highest among all the courses. The final assessment was based on 41 providers.
Conclusions:
The course proved a successful tool for training healthcare providers in methods of cervical cancer screening and treatment. The course is replicable in other low-resource settings in different countries. It also provided trainees with the opportunity to adapt their clinical skills in their realistic work setting.
Introduction
Cervical cancer is the leading cause of cancer-related mortality among women in developing countries. 1 El Salvador has one of the world's highest cervical cancer incidence and mortality rates, at 45.6/100,000 and 23.5/100,000, respectively, and cervical cancer is the most frequently diagnosed cancer in women. 2
In 2002, Agurto et al. 3 conducted an intervention study to improve the efficacy of the Pap smear system in a semirural region of El Salvador. Their approach required multiple follow-up visits, however, which is not feasible in most rural areas. In 2007, only 19% of eligible women received a Pap smear through the public sector, and only 30% of these were ever read by a cytotechnologist. 4 The public sector in El Salvador does not currently have the infrastructure to handle the burden of processing hundreds of thousands of Pap smears annually.
Visual inspection with acetic acid (VIA) has gained popularity as a simple, low-cost alternative to traditional Pap smears. 5,6 The major advantage of this screening technique is that it can be performed in conjunction with treatment. All levels of healthcare providers can be trained to practice the single visit, see-and-treat approach. 7,8 Effective training courses include didactic and clinical components, supported by quality assurance measures, such as knowledge testing and refresher courses. VIA training has been implemented successfully in many low-resource settings; however, a Ministry of Health (MOH)-sponsored course had never been implemented in El Salvador.
The objective of this study was to train MOH Generalist Physicians (GPs) and Registered Nurses (RNs) in VIA and cryotherapy during a week-long competency-based course. The entire course consisted of 1 half-day of didactics, followed by 4 and 1 half days of clinical training. Pretests and posttests were administered to measure knowledge before and after the training course.
Materials and Methods
From March 2007 to November 2009, a total of 68 MOH RNs and GPs participated in the VIA training course. The study was approved by the Institutional Review Boards of New York University School of Medicine and Mount Sinai Medical Center and received official support from the Salvadoran MOH. Trainees were chosen by the MOH and were selected because they provided preventive healthcare services, including cervical cancer screening, to women living in the most rural regions of the country.
Predidactics and didactic
On the first day of the course, participants were given a training manual in Spanish and cervical image flashcards (Jhpiego, Baltimore, MD). Before the didactic session, the trainees took two pretests. The first tested their basic knowledge of cervical cancer. The second, a visual image examination, assessed their ability to recognize a normal cervix and varying degrees of cervical pathology. After taking the pretests, the trainees participated in a half-day didactic session that reviewed cervical cancer etiology and pathology, as well as screening and treatment options. The trainees watched a Power Point presentation that reviewed the contents of the training manual, and smaller groups were then formed to review the cervical image flashcards.
Clinical training
Before seeing patients, students were shown anatomical Zoe© models to familiarize them with gynecologic examinations. Students also practiced cryotherapy techniques on cervical simulation material (sausages). The trainers, all experienced gynecologists, determined when the trainees achieved competency with the simulations. The trainee was then matched with a trainer in a 1:1 or 1:2 ratio and was observed performing clinical examinations, VIA, and cryotherapy. Pap smears were performed only when the squamocolumnar junction was not visible or the woman was >50 years old, as per the El Salvador MOH guidelines. 9
Each trainee screened approximately 120 women and performed, on average, seven cryotherapy treatments. The trainer confirmed all VIA diagnoses, and immediate feedback was given on technique, diagnosis, and patient interaction.
Postcourse tests
After completion of the clinical practicum of the course, two posttests were administered to assess differences in theoretical knowledge (written examination) and ability to visually identify cervical pathology (image examination). Trainees' pretest and posttest scores were compared to determine the change in their knowledge.
Results
From March 2007 to November 2009, 68 nurses and physicians completed the training course. Six of the trainees took the course two times, but only their first scores were included in the analysis. Pretest and posttest scores from course 2, Cojutapeque 2007 (n=14), have been excluded from analysis because of loss of original data. Course 5 posttest scores (n=10) were not collected because of a series of unanticipated emergencies; thus, this training course was also excluded from analysis, as pretest and posttest scores could not be compared. Three medical professionals completed only pretests or posttests, and their results were also excluded from the analysis. Complete data (having completed theoretical pretest and posttest and image tests) was available for 41 trainees (Fig. 1). Average test scores are presented in Table 1 for the 41 trainees completing both theoretical pretest and posttest and image tests.
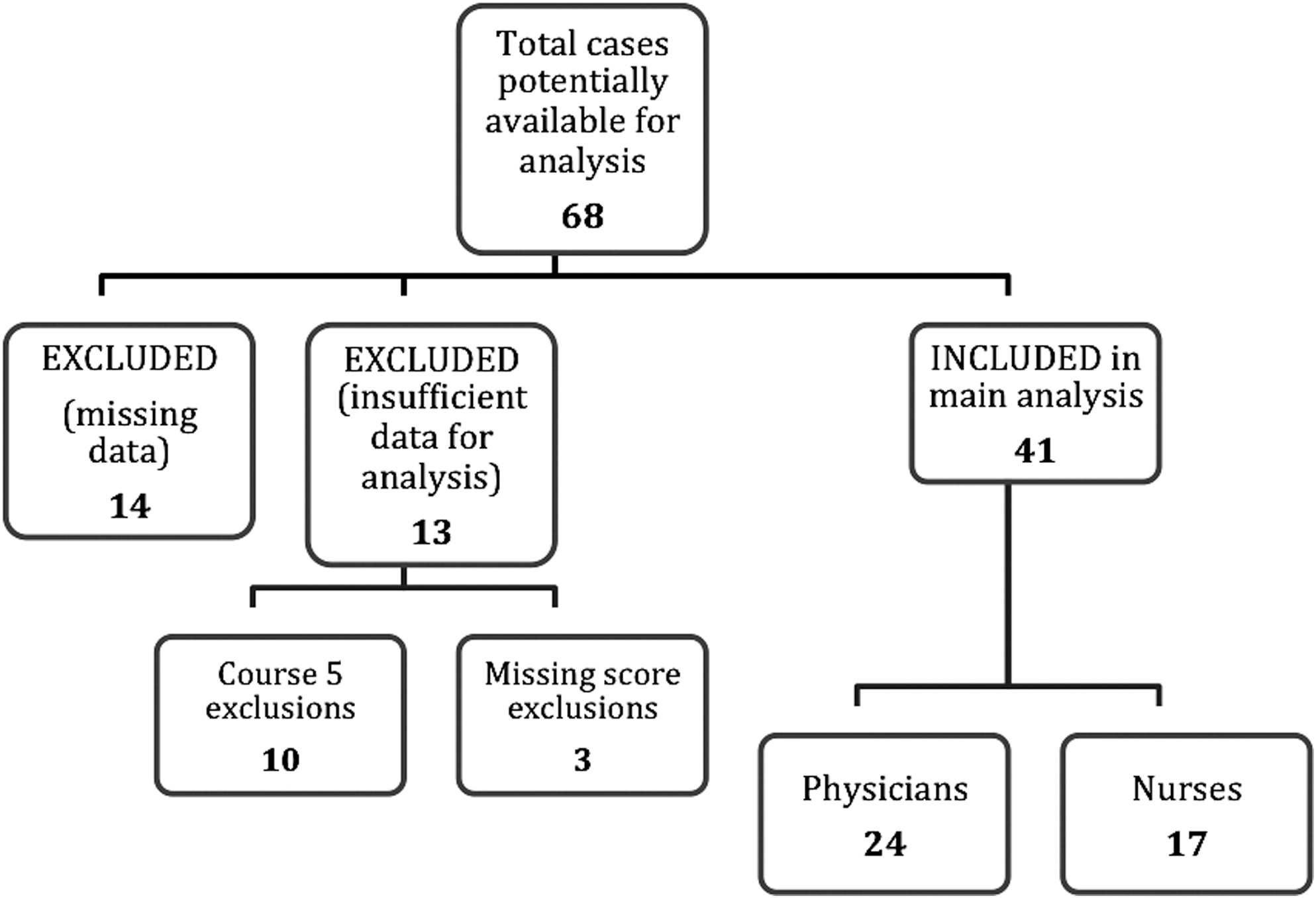
Flow chart showing number of excluded and included cases.
The average theoretical pretest score was 72.7 (standard deviation [SD] 14.1), and the average theoretical posttest score was 81.3 (SD 10.9). The average image pretest score was 70 (SD 12.9), and the average image posttest score was 79.5 (SD 6.2). On average, trainees improved their score by 14.9% (SD 22.8) on the theoretical test and 17.5% (SD 24.2) on the image test.
To evaluate the impact of the training course on participant's theoretical posttest and image tests, a paired two-tailed sampled t test was conducted (Table 2). The analysis included the sample of 41 medical professionals completing the theoretical pretest and posttest and image tests. Results revealed a significant improvement from the theoretical pretest (mean [M] 72.68, SD 14.15) to posttest (M 81.34, SD 10.78) scores, t(40)=−5.141, p<0.0001. Similarly, results showed a significant increase in overall scores from image pretest (M 69.99, SD 12.87) to posttest (M 79.46, SD 6.79) examinations, t(40)=−4.473, p<0.0001.
Significant at the 0.05 level (2-tailed).
Next, an independent-sample t test was conducted to compare the theoretical and image pretest and posttest scores for physicians and nurses (Table 3). A total sample of 24 physicians and 17 nurses were included in the analysis. On average, physicians performed higher on theoretical posttests (t(39)=−2.792, p=0.008) compared to nurses. However, there was no statistically significant difference between theoretical pretest scores (t(39)=−1.736, p=0.090) and image pretest (t(39)=−1.065, p=0.294) and image posttest scores between groups (t(39)=−0.255, p=0.800). On average, GPs improved their theoretical test scores by 16.4% and image test scores by 14.8%, whereas RNs improved their theoretical test scores by 12.7% and image test scores by 21.3%.
Significant at the 0.05 level (2-tailed).
Theoretical test scores were consistent across the courses; however, a one-way analysis of variance (ANOVA), conducted to explore test score variation by course (San Vincente 2007, Illobasco 2008, Suchitoto 2008, and Suchitoto 2009) revealed a statistically significant difference in image posttest scores among the training courses: F(3,40)=3.252, p=0.032. A post-hoc comparison using the Tukey Honestly Significant Difference (HSD) post-hoc test revealed that the mean score for course 2 (M 75.57, SD 4.34) was significantly different from that for course 4 (M 84.50, SD 3.70, p=0.051). Other comparisons did not differ significantly.
In September 2008, 14 trained GPs and RNs took a 1-day didactic refresher course. Of the 14, 6 were excluded from analysis for the following reasons: 4 were participants of course 2, which was excluded because of loss of data; 1 participant took the training course twice before this refresher course; and 1 participant did not complete both the theoretical pretest and the image test before the refresher course. Thus, 8 participants in the refresher course are analyzed in this report. The average initial pretest scores of the 2 nurses and 6 physicians were 80% for pretheoretical and 75.3% for preimage compared to 83.8% and 76.3%, respectively, on the posttests from their initial training course. Posttest scores from the refresher course showed significantly greater improvement from the initial pretest scores at 90% (t(8)=−2.935, p=0.022) and 93% (t(8)=−3.797, p=0.007), respectively.
Discussion
Basic Health International's course proved a successful tool for training healthcare providers in methods of cervical cancer screening and treatment. The course was a modified version of the Association of Cervical Cancer Prevention (ACCP) training course used in more than a dozen countries around the world. 10 The ACCP report that physicians, on average, need to conduct 30 VIA examinations and two cryotherapy treatments to achieve competency, and nonphysicians need to conduct 132 VIA examinations and three cryotherapy treatments. From 2006 to 2009, we trained 68 providers in both VIA and cryotherapy. On average, each trainee conducted 120 VIA examinations and 7 cryotherapy treatments per course. In order to ensure that our program provided the highest quality training, we employed two core-quality assurance measures. Trainees were given a certificate of course completion if they (1) achieved a passing score on the written and image examinations (>70%) and (2) achieved competency in the clinical techniques of VIA and cryotherapy. This included the ability to correctly identify normal, abnormal, and cancerous cervices and to recite what treatment and follow-up protocol was to be used.
Trainees began implementing the see-and-treat modality in the fall of 2008, when the Salvadoran government officially recognized VIA as the primary screening method for women aged 25–49 living in the most rural regions of the country. 9 To assess the quality of services being provided, we administered a 1-day didactic refresher course and then accompanied trainees to their rural work areas to conduct a process evaluation. Average refresher course pretest scores decreased slightly from trainees' original posttest scores. At the completion of the 1-day refresher, average test scores increased to the highest level obtained among all the courses (average theoretical score=88.3%; average image score=91.7%). The process evaluation provided trainees with the opportunity to adapt their clinical skills in their realistic work setting and allowed each trainee to gain confidence in service provision.
The major limitations to this study were due to data collection and management. Pretest and posttest data were unavailable for analysis from course 2 because of loss of the original data. In course 5, neither the postwritten nor postimage examinations were administered because of an unfortunate tragedy that forced participants to leave the course immediately after the clinic portion. Trainees intended to take the test the following week, but El Salvador fell into a national state of emergency because of the H1N1 virus epidemic.
As the training sessions progressed, we made quality improvements to the didactic and testing elements of the course. For example, in training course 1, the image test answer key allowed for multiple correct answers to individual questions. The updated version of the image examination answer key (used for courses 2–6) eliminated this problem. During course 6, instead of the cervical images being projected onto a large screen (as in courses 1–5), each pair of trainees shared a laptop to view the cervical images. The image quality was noted to be much more clear (higher resolution, improved color quality) compared to the previously projected images. However, the only significant difference among image posttest scores was between courses 2 and 4 (p=0.051).
As we continue to evaluate our own training process, we plan to further standardize examinations and training tools. For example, it is vital for trainers to use a standardized checklist to quantify trainee progress and learning. This checklist may be used to help conduct the process evaluation of adapting the clinical skills to the real world, rural work environment. To ensure that trainees' skills remain intact, we believe it is important to issue annual competency examinations and offer refresher courses.
To help ensure that trainees can successfully integrate VIA into practice, each doctor/nurse team was provided with a cryotherapy kit that included a cryotherapy unit, three cryotips, a digital timer, instrument tray, speculums of different sizes (n=14), a cryotherapy gas tank, plastic containers, a cup for acetic acid, acetic acid, cot, folding screen, soap, Monsel's solution, and a cart to carry the entire contents. With these items, the trainees had all the items necessary to conduct VIA and cryotherapy in their rural communities. The total cost of the kit was approximately $2,200 US, with the cryotherapy unit being the bulk of that expense ($1,700–$2,000 US). Equipment costs can be significantly reduced if a cryotherapy unit is stored in a central location for access by multiple healthcare providers. In addition, by being able to diagnose and treat women at one visit, the cost savings encompass more than just the cost of the test ($US3.50/Pap test; less than $US2 for each VIA). It includes the cost of a woman's time away from work and family, the high cost of treating advanced disease, and the high cost of the morbidity and mortality from this disease to the family and community. The other major course cost was that of transporting US-based gynecologists to El Salvador. To decrease costs, a train-the-trainer program, in which previous trainees become the trainers, can be integrated. This not only decreases the course budget but also improves the chances of developing a sustainable program.
In 2009, there were 451 women screened with VIA by Basic Health International (BHI)-trained Salvadoran physicians and nurses. There are currently 22 RNs and GPs practicing this modality in El Salvador. In 2010, there have been over 2,300 women screened, 119 who received immediate cryotherapy, and 35 who were referred to a colposcopy center for delayed treatment because of a lesion that was too large or suspicious for cancer. We are currently following these women to ensure they receive necessary follow-up.
The strengths of this study are, first and foremost, that the course provided ample opportunity for trainees to master performing the skills of VIA and cryotherapy. The low ratio of trainers/trainees allowed for ample interaction and feedback from trainers. The pretests and posttests provided a much needed quality assurance measure. In each training course, there was an overall increase between pretest and posttest scores. Above all, the training courses have generated enthusiasm and attention for cervical cancer prevention among the healthcare providers and the rural women they serve.
Conclusions
We have developed a replicable cervical cancer prevention training program. It is feasible, proven to work, transportable between training facilities within El Salvador, and will be easy to implement in other low-resource settings around the globe. In addition, the course format was developed to easily scale up and integrate new screening technologies, such as CareHPV (Qiagen Corp, Gaithersburg, MD). It is our hope that the increase in screening and treatment will help to markedly decrease the incidence of cervical cancer, thus decreasing women's morbidity and mortality from this largely preventable disease.
Footnotes
Acknowledgments
This work was supported by The Einhorn Family Charitable Trust.
Disclosure Statement
No competing financial interests exist.