
Abstract
Background:
Regular physical activity usually confers health benefits, but high-level sport may induce harmful outcomes, such as pelvic floor dysfunction. Urinary incontinence (UI) was previously documented, but few data are available about anal incontinence (AI) in female athletes. Our aim was to determine the role of high-level sport practice on AI in a young, healthy female population.
Methods:
In this cross-sectional study, we included women aged 18–40 years. Self-administered questionnaires were delivered to each female volunteer. Two groups were defined: (1) intensive sport (IS) group: high-level sport (>8 hours weekly), and (2) nonintensive sport (NIS) group: all other subjects.
Results:
Of the 393 women enrolled, 169 were in the IS group and 224 were in the NIS group. Women of the IS group were significantly younger than the others (21.74±4.28 vs. 24.87±5.61 years, p<0.001) and had less births (0.07±0.31 vs. 0.20±0.62, p=0.005). The prevalence of AI was statistically higher in the IS group than in the NIS group (14.8% vs. 4.9%, p=0.001), as was UI (33.1% vs. 18.3%, p=0.001). Multivariate analysis showed that IS practice (odds ratio [OR] 2.99, 95% confidence interval [CI] 1.29-6.87, p=0.010) and body mass index (BMI) (OR 1.14, 95% CI 1.01-1.28, p=0.033) were significantly linked to AI when taking into account major confounding factors (age and births). In the IS group, AI was mainly represented by loss of flatus in 84%.
Conclusions:
High-level sport appears to be a significant independent risk factor for AI in healthy young women. These results suggest that preventive measures, such as pelvic floor muscle training, may be proposed for this young population.
Introduction
Regular physical activity confers long-term health benefits in women of all ages. 1,2 Epidemiologic studies showed protective effects of physical activity on chronic diseases, including coronary heart disease CHD, 3 hypertension, 4 osteoporosis, 5 non-insulin-dependent diabetes mellitus, 6 and anxiety and depression. 7,8 Because of the benefits of physical activity on physical and mental health, the Centers for Disease Control and Prevention (CDC) recommends that people practice a moderate-intensity physical activity for at least 30 minutes on most days of the week. 9 However, high-level sport may induce some harmful outcomes, such as ligament and tendon injuries, stress fractures, and pelvic floor dysfunction. 10 Diagnosis and treatment of pelvic floor dysfunction in female athletes is particularly important because these lesions may compromise their future quality of life. Indeed, high-level sport induces significant modifications in function and anatomy of the pelvic floor, which may alter childbirth conditions and continence mechanisms. 11 However, whereas a higher prevalence of stress and urge urinary incontinence (UI) in elite athletes is well documented, 12 –15 only limited data are available about the impact of high-level sport on the prevalence of anal incontinence (AI), and none has evaluated this parameter vs. a control group. AI may have many causes, but postobstetrical lesions represent a frequent cause in young females. Some other risk factors, such as age, diarrhea, obesity, neurologic diseases, diabetes mellitus, idiopathic pudendal neuropathy, poor self-perceived general health status, and sexual or physical abuse have already been identified. 16 –19 Although a National Institutes of Health (NIH) conference hypothesized that sport, work, and sexual activity may be new causes of AI, 20 high-level sport is not currently considered a classic risk factor of AI.
The aim of this study was to determine the role of high-level sport practice on AI in a young, healthy female population. Other symptomatic pelvic floor disorders, UI, constipation, and dyspareunia, were also documented.
Materials and Methods
Study design and subjects
This study incorporated a cross-sectional design and took place in a public university in the South of France (Marseille, France) and focused on three schools: the sports university (450 eligible women), the physiotherapy program (150), and the nurses' institute (150). The study was supervised by the Gastroenterology Department of the University Hospital (North Hospital, Marseille, France). Information indicating the aim and design of the survey was given to all the students' managers, and all women 18–40 years old were eligible. For 1 month, short meetings were organized on the campus by the medical staff to inform female students and workers about incontinence among young, healthy people and its management or prevention strategies. These activities were performed in accordance with the law (Law on Data Processing, Data Files and Individual Liberties of January 6, 1978, amended by the law of Public Health of August 9, 2004, relating to the protection of individuals with regard to the processing of personal data).
According to the literature, a high-level sport was defined by a training regimen of at least 8 hours per week. 12 A planned or an ongoing pregnancy was an exclusion criterion. Participants had complete the questionnaire for the responses to be taken into account.
Data collection
Anonymous self-administered questionnaires were delivered to the female volunteers. A cover letter identified the sponsoring organization and outlined the purpose of the study and instructed participants to return completed questionnaires to specific locations. The ad hoc questionnaire comprised four parts: (1) demographic and personal data, including age, educational level, number of children, position during the day (mainly recumbent or not), and carrying heavy weights, (2) personal health status, including medical (especially diabetes mellitus and neurologic diseases), obstetrical, and surgical history and body mass index (BMI), (3) sport practice characteristics, that is, no activity or leisure/high-level practice, type and number of sports, and weekly frequency, and (4) information about pelvic floor symptomatology, including AI, UI, constipation, and dyspareunia. For each symptom present, more details, such as frequency, nature of leakage, and symptom history were asked.
Definitions
Anal incontinence (AI) was defined as involuntary loss of stool (solid or liquid) or flatus. 21 The single question was: Did you have an accidental anal leakage of solid, liquid, mucus, or gas at least once in the last 6 months? If yes, supplementary information was required: type of protection worn if any, leakage composition, leakage duration, and frequency.
The definition of urinary incontinence (UI) was derived from the International Continence Society collaboration as “the complaint of any involuntary leakage of urine.” 22 A single query was posed to the participants: Did you have an accidental urinary leakage at least once in the last 6 months? If yes, supplementary information was required: type of protection worn if any, leakage duration, and frequency.
Constipation was defined according to the Rome III criteria by the presence of two or more of the following symptoms: (1) straining during at least 25% of defecations, (2) lumpy or hard stools in at least 25% of defecations, (3) sensation of incomplete evacuation for at least 25% of defecations, (4) sensation of anorectal obstruction/blockage for at least 25% of defecations, (5) manual maneuvers to facilitate at least 25% of defecations, and (6) fewer than three defecations per week, with criteria fulfilled for the last 3 months and symptom onset at least 6 months before diagnosis. 23 The single question was: Did you have constipation problems, such as less than three bowel movements per week, difficult evacuation of stools, forced straining during defecation, or a sensation of incomplete evacuation after defecation? If yes, supplementary information was required: number of stools per week, diarrhea, digital evacuation, sensation of anorectal blockage, and history of the symptoms.
Dyspareunia was defined as pain during sexual intercourse. 24 The single question asked was: Did you feel discomfort or pain during sexual intercourse?
Types of sports
The different sports included in the study were distributed into seven groups as previously described 12,25 : group 1: technical (alpine skiing, horseback riding, sailing, water skiing); group 2: endurance (swimming, cycling, track and field), group 3: aesthetic (gymnastics, dance, rhythmical gymnastics, fitness), group 4: weight class (karate, judo); group 5: ball games, tennis; group 6: power (discus, javelin); group 7: gravity (climbing, high jump).
Statistical analysis
Sample characteristics were detailed using mean (standard deviations [SD]) for quantitative variables and frequencies for qualitative variables. Two groups of women were defined in accordance with the literature 12 : (1) intensive sport (IS) group: women practicing high-level sport or >8 hours weekly or both, (2) nonintensive sport (NIS) group: all other subjects. Comparisons between the IS and NIS groups were performed using Student's t tests for quantitative variables and chi-square or Fisher's exact tests for frequencies. Multivariate analysis using logistic regression models were performed using a forward stepwise approach to determine variables potentially linked to AI and UI. Variables relevant to the models were selected on their clinical interest or a threshold p value ≤0.2 during univariate analysis. Variables selected for AI were age (clinical interest), BMI (p<0.20), sport group (p<0.20), having had children (clinical interest), and sport practice in the past 6 months (p<0.20). The use of forceps during vaginal delivery was not selected as a variable because this applied to only 2 women in the AI group. Variables selected for UI were age (clinical interest and p<0.20), BMI (p<0.20), sport group (p<0.20), having had children (clinical interest), educational level (p<0.20), forceps delivery (clinical interest), and sport practice in the past 6 months (p<0.20). The final models expressed the odds ratios (OR) and 95% confidence intervals (CI). All the tests were two-sided. Statistical significance was defined as p<0.05. Statistical analyses were performed using the SPSS version 15.0 software package (SPSS Inc., Chicago, IL).
Results
General characteristics
Over a 6-month period, a total of 393 of 750 eligible women were enrolled (participation rate 52.4%), 169 in the IS group and 224 in the NIS group. None of them had diabetes or neurologic disease. The characteristics of the sample are presented in Table 1. IS women were significantly younger than the others (21.74±4.28 vs. 24.87±5.61, p<0.001), were more likely to have >12 years of education (92.9% vs. 81.7%, p=0.001), and were less likely to have had children (4.7% vs. 12.6%, p=0.008). Among those reported to have had at least one child, the IS group reported fewer forceps deliveries. As detailed in Figure 1, the prevalence of AI was statistically higher in the IS group than in the NIS group (14.8% vs. 4.9%, p=0.001), as was the prevalence of UI (33.1% vs. 18.3%, p=0.001) and dyspareunia (20.1% vs. 9.4%, p=0.002). A total of 13 different sports were represented, and they were grouped in accordance with the seven groups: group 1: sailing, horseback riding, alpine skiing, water skiing; group 2: swimming, cycling, track and field; group 3: gymnastics, dance, fitness; group 4: fighting; group 5: ball games, tennis; group 7: climbing, high jump. No sport belonging to group 6 was represented. Figures 2 and 3 show the distribution of reported sport categories among the IS women, according to incontinence status. AI was reported in 31.6% (6 of 19) of climbing athletes (group 7), whereas 9.5% (2 of 21) of athletes in group 4 reported having AI.
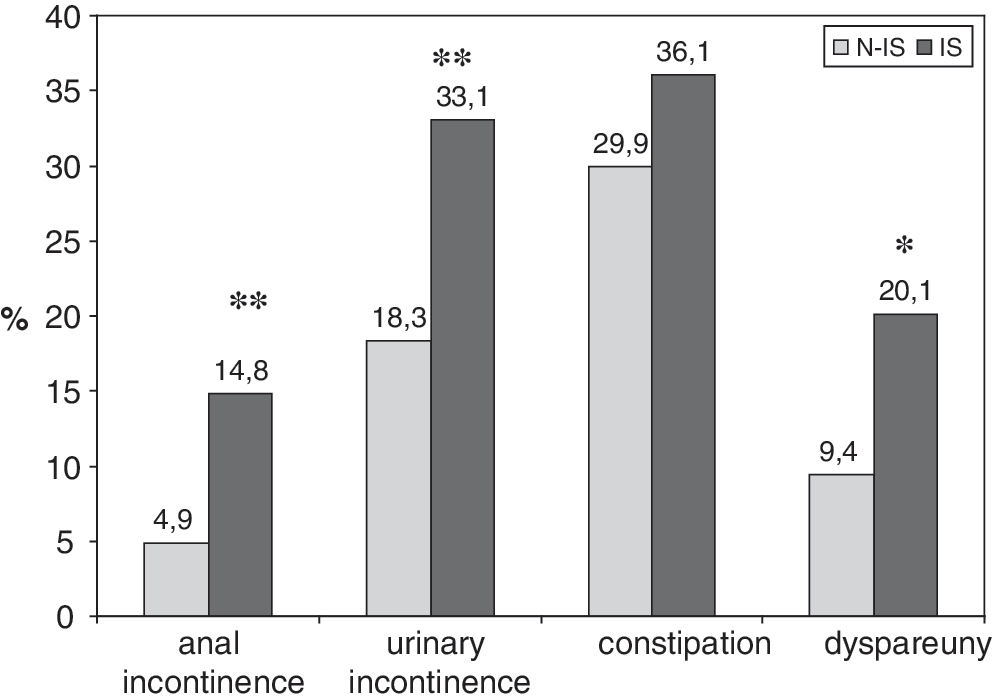
Prevalence of anal incontinence (AI), urinary incontinence (UI), constipation, and dyspareunia according to sport practice: nonintensive sport (NIS), intensive sport (IS). *p=0.002; **p=0.001.

Distribution of AI in the different sport categories among women in the IS group. Group 1: sailing, horseback riding, alpine skiing, water skiing; group 2: swimming, cycling, track and field; group 3: gymnastics, dance, fitness; group 4: fighting; group 5: ball games, tennis; group 7: climbing. No sport belonging to group 6 was represented.
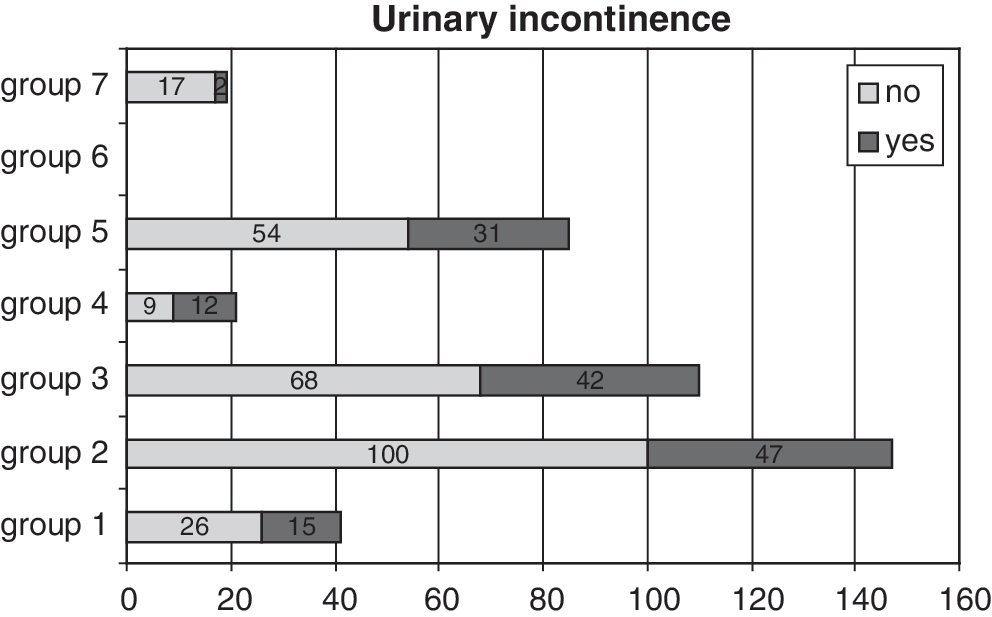
Distribution of UI in the different sport categories among women in the IS group. No sport belonging to group 6 was represented.
p value of NIS vs. IS.
BMI, body mass index; IS, intensive sport group; NIS, nonintensive sport group; SD, standard deviation.
Characteristics of anal incontinence, urinary incontinence, and constipation
The characteristics of AI and UI were not significantly different between IS and NIS women (Table 2). In the IS group (n=25), AI was mainly represented by loss of flatus in 84%, with a need for protection use in 8%. Anal leakages were daily in 20.0% of subjects, weekly in 36.0%, and monthly in 44.0%. Anal leakage duration was <6 months in 52.0% of subjects, 6–12 months in 8.0%, 12–24 months in 24.0%, and >24 months in 16.0%. Among the 56 IS women who reported IU, 61.8% noted that urinary leakage occurred only during practice sessions, and 19.6% admitted to wearing a pad. Urinary leakage frequency was daily in 1.9% of the women, weekly in 80.8%, and monthly in 17.3%. Duration of urinary symptoms was <6 months in 46.4%, 6–12 months in 7.1%, 12–24 months in 12.5%, and >24 months in 33.9%. Of the 128 women reporting constipation, the IS women indicated significantly more important difficulties with stool evacuation than did the NIS women: 31.1% (19 of 61) vs. 13.4%, p=0.02. No differences were noted in sensation of incomplete evacuation after defecation, forced straining during defecation, or digital evacuation.
NS, not significant.
Risk factors of anal incontinence and urinary incontinence
Tables 3 and 4 showed risk factors of AI and UI, respectively. Women with AI (n=36) differed statistically from women without AI (n=357) on two parameters: they were younger (p=0.007) and more frequently practiced high-level sport (p=0.001). Carrying heavy weights and position during the day were associated with AI in single variable analysis but not in multivariate analysis. After adjustment, IS practice and BMI were the two parameters linked to AI (OR 2.99, 95% CI 1.29-6.87, p=0.010, and OR 1.14, 95% CI 1.01-1.28, p=0.033, respectively). Women with UI (n=97) were statistically more frequently involved in intensive sport than women without UI (n=297). After adjustment, BMI and the IS group were significantly associated with UI (OR 1.99, 95% CI 1.14-3.30, p=0.02, and OR 1.09, 95% CI 1.00-1.19, p=0.04, respectively).
p value of no anal incontinence vs. anal incontinence.
p value by multivariate analysis.
CI, confidence interval; OR, odds ratio.
p value of no urinary incontinence vs. urinary incontinence.
p value by multivariate analysis.
Discussion
Our study is the first to demonstrate convincingly that high-level sport is a significant risk factor for AI. We studied a population of 393 women, 169 in the IS group and 224 in the N-IS group. Women were defined as IS practitioners if they trained at least 8 hours per week, as previously defined. 12 In the general population, the prevalence of fecal incontinence and AI ranges from 0.4% to 18% and 2% to 24%, respectively. 18 Differences in prevalence estimates are explained partly by differences in case definition, with some studies including involuntary loss of flatus in the definition and other studies limiting the definition to loss of stool or mucus. There is an evolving consensus to use the term “fecal incontinence” to refer only to involuntary loss of solid or liquid stool or mucus and to use the term “anal incontinence” to include flatus as well as solid or liquid stool and mucus 16 ; therefore, these two definitions can be confusing. In our study, we decided to evaluate anal incontinence, including loss of flatus because all kinds of incontinence can interfere with quality of life and have a severe impact on social interaction and self-image, especially in young women. 26 As a majority of subjects with AI only reported loss of flatus, the prevalence of AI was probably artificially overestimated. The clinical significance of this study should be interpreted cautiously in accordance with this chosen definition. The rate of AI in our control group (4.9%) is in accordance with the literature, as the general prevalence of AI, including flatus, ranges from 2.2% to 4%, 21,27,28 with another study showing a prevalence of only flatus incontinence of 5.8%. 29
We used an anonymous self-administered questionnaire in this study, as recommended. 18,30 For AI, severity tools have used three distinct measures: (1) stool loss, (2) use of coping mechanisms (such as wearing a pad), and (3) impact on or changes in life. To assess the severity of AI, we used a self-reported instrument adapted from the Jorge and Wexner scale, 31 including type of loss, use of pad, and frequency of loss episodes. The strength of this instrument is the ease of scoring, 32 which was an important parameter in our study because of the large number of items in the questionnaire. We observed a participation rate of 52.4%, which may be a limit of our study because it may overestimate or underestimate the prevalence of AI.
IS women were significantly younger than those in the NIS group, and a lower percentage of them had given birth. However, whereas age and childbirth are risk factors for AI, a mean younger age and lower rate of child birth (that may induce anorectal damages) in the IS group reinforces the fact that IS is an independent risk factor for AI. In our study, the prevalence of AI was nearly three times higher in the IS group than in the NIS group (14.8% vs. 4.9%, p=0.001). To our knowledge, this is the first study to assess these data, as studies in elite female athletes most often studied UI.
A high BMI is known to be a risk factor for AI. 17,33 After multivariate analysis in our study and as previously described in the literature, BMI appeared to be a risk factor of AI. The difference in BMI between the two groups was slight, however, perhaps indicating that in some categories of subjects with some other risk factors, a small increase in BMI may have consequences on AI. In the IS group, AI was mainly represented by loss of flatus in 84% of subjects, with a need for protection use in 8%. Leakages were observed daily in 20% of subjects, weekly in 36%, and monthly in 44%. There were no significant differences between the IS and the NIS groups concerning the characteristics of AI (wearing of protection, leakage frequency, leakage nature, and leakage duration).
In our study, 33% of the women in the IS group reported urinary loss, which is in accordance with the prevalence observed in elite athletes. 12 –15 The prevalence of UI (18.3%) observed in the NIS group was similar to the prevalence of UI reported for the general population of women <45 years old (19%). 20 Moreover, we observed a significant difference between the IS group and the NIS group in UI that has not been described previously. The prevalence of dyspareunia was also significantly higher in the IS group than in the NIS group (20.1% vs. 9.4%, p=0.002). In the literature, data suggest that dyspareunia is influenced by age and psychosocial factors and that sexual problems are more common in young women. Moreover, the presence of urinary tract symptoms appears to impact sexual function. 34
The main causes of AI and UI are child birth injuries and advanced age. In women participating in high-level sport or in elite female athletes, etiologic factors may include inadequate abdominal pressure transmission, stress injuries to the fascia, pelvic floor muscles, or ligaments, and changes in connective tissue or collagen. 15,35 Thus, such activities as ball games, which create a sudden increase in intraabdominal pressure, are associated with an increased prevalence of both AI and UI. In the present study, no one type of sport was significantly associated with a higher prevalence of AI than the other types of sport. There are no established data about type of sport and AI in the literature, although more data are available for UI. Indeed, gymnastics and ball games are the sports more frequently associated with urinary leakage 15 even in the absence of known risk factors for UI. This trend was not observed in our study.
By demonstrating a higher prevalence of the symptoms of AI in a group of young women who do not have any of the conventional risk factors for incontinence (such as child birth injuries, advanced age, or postmenopausal status), the current study may help to identify a new at-risk population, as was suggested by the NIH in 2008 20 but that had not yet been demonstrated. Owing to the benefits of regular body exercise, women should not be discouraged from exercising. However, young women who engage in long-term high-impact sports should be informed of possible consequences of exercise on pelvic floor function. In light of the findings of the current study, preventive measures could be developed in this newly identified population. Primary prevention in young high-level female athletes, such as education about methods for preventing incontinence, should take precedence over secondary prevention measures of detecting AI symptoms at an early stage.
Footnotes
Acknowledgment
We thank Pr. Pascal Auquier for reviewing the manuscript.
Disclosure Statement
The authors have no conficts of interest to report.