
Abstract
Background:
Use of the oral contraceptive pill (OCP) is associated with numerous health benefits as well as risks, and it is important that women take these into consideration when making informed contraceptive choices.
Methods:
A questionnaire assessing contraceptive practices, knowledge and beliefs about the risks and benefits of OCP use, and information needs and preferences was distributed to 1200 Australian women aged 18–50 years.
Results:
Of the 305 women who returned the questionnaire, 93% had used the OCP at some time in their lives, with 32% reporting current usage. Only 50% of women reported satisfaction with previously accessed information about the OCP. Less than 40% of the sample reported a high level of confidence in their knowledge of the risks, benefits, and side effects of OCP use. Factors associated with greater OCP knowledge included being married (β=1.74, 95% confidence interval [CI] 1.11-2.72), having a university education (β=2.20, 95% CI 1.49-3.24), longer duration of OCP use (β=1.06, 95% CI 1.02-1.09), and having greater confidence in one's knowledge about the OCP (β=1.70, 95% CI 1.38-2.09), whereas depressive symptoms were associated with lower knowledge (β=0.93, 95% CI 0.88-0.99). Preferred formats for the communication of OCP-related information were the internet and an information booklet.
Conclusions:
The findings provide an evidence base for the future development of simple and appropriate tools by which to communicate information about the health benefits and risks of OCP use to women.
Introduction
The oral contraceptive pill (OCP) is one of the most popular forms of contraception, with usage estimates of >60 million women worldwide. 1 Although there are important health risks and benefits associated with OCP use, healthcare professionals prescribe the OCP because it is considered safe, effective, and well tolerated. Women use the OCP for these reasons, as well as for its convenience as a contraceptive. 2 Given the importance of the protective and negative effects of OCPs for women, there is a growing body of research documenting women's knowledge of and beliefs about these risks and benefits. There is also increasing awareness of women's need for information about the OCP, as well as their desire for support when making contraceptive decisions.
Benefits, risks, and side effects associated with OCP use
In terms of health benefits, OCP use has been associated with substantial reductions in ovarian and endometrial cancer risk, 3 as well as the risk of benign breast disease. 4 There are also emerging data to suggest a slight reduction in colorectal cancer risk with OCP use; however, further studies are needed to provide details of the underlying causal pathway. 5 Other benefits include a reduction in dysmenorrhea, menorrhagia, functional ovarian cysts, and ectopic pregnancy risk, 4 as well as a reduced risk of pelvic inflammatory disease (PID), acne, hirsutism, hyperandrogenism, uterine leiomyomas, rheumatoid arthritis, pain associated with endometriosis, and ailments that become exacerbated during the menstrual cycle, for example, migraines and asthma. 3,4
Several health risks associated with OCP use have also been documented. OCP use increases the risk of venous thromboembolism, myocardial infarction (MI), and stroke, 4 although the risk of any cardiovascular event is strongly related to other comorbidities, such as age, smoking, and obesity. 3,4 Use of the combined OCP may also be associated with an increased risk of cancer of the liver and uterine cervix, although this is dependent on duration of usage. 4 Although past studies have demonstrated a slight increase in the absolute risk of breast cancer with OCP use, 6 a recent review found no significant relationship between breast cancer risk and modern oral contraceptive use. 2
The OCP has many reported side effects that can manifest as weight gain, nausea, breast tenderness, headaches, acne, abdominal and back pain, breast enlargement, mood swings, premenstrual syndrome (PMS), and irregular bleeding. 2,3,7 –10 These side effects are commonly cited as a primary reason for women's negative attitudes toward the OCP and as the reason for either nonuse or cessation of use. 11,12 Given the wealth of evidence for the benefits, risks, and side effects associated with OCP use, weighing all of this information in order to come to an informed decision about what is best for the individual woman is no easy feat. Moreover, although there are risks associated with OCP use, such risks should be considered in light of those associated with unplanned pregnancies prevented by OCP use. 2,12
Knowledge of and beliefs about the risks and benefits of OCP use
Although general practitioners have long been advised to counsel women repeatedly about OCP use, as well as to provide written information, 13 previous studies suggest that there are substantial deficiencies in women's knowledge about the OCP and that many women hold misconceptions about OCP use. Studies have found that many women are unaware of the noncontraceptive health benefits associated with OCP use and have limited knowledge of OCP-related health risks. For example, in a study involving predominantly African American women, Davis et al. 14 found that over half of the women surveyed could not name a single side effect related to OCP use, and only 42% could name at least one medical risk. Similarly, Kirkkola et al. 15 found that Finnish women lacked knowledge of the risk of thrombosis associated with OCP use, as well as the dangers related to smoking while using the OCP. A range of factors may be associated with greater OCP knowledge, including younger age, higher educational level or socioeconomic status (SES), greater desire not to conceive, previous use of emergency contraception, and prior participation in OCP-related educational interventions. 16,17 Differences in level of OCP knowledge have also been reported between ethnic groups, with minority groups reported to have lower knowledge. 18
The aims of the present study were to (1) describe the contraceptive beliefs and behaviors of a community sample of Australian women of reproductive age, (2) identify the factors associated with women's knowledge of the risks, benefits, and side effects of OCP use, and (3) establish how women have been receiving OCP-related information, whether they are satisfied with this information, and in what format(s) they would prefer to receive OCP-related information in the future. Our understanding of women's knowledge of the risks and benefits associated with OCP use is beginning to take shape, and this study will provide up-to-date data in this area. The third aim of this study is novel, as there are few published data on women's information needs in relation to the OCP worldwide. Further, women's preferences regarding the formats in which information about the OCP should be communicated are underresearched.
Materials and Methods
Participants
Eligible participants were ascertained via the Australian Electoral Commission (AEC), which organizes federal elections and maintains the Commonwealth electoral roll. The AEC provided the postal addresses for a random sample of 1200 women, with proportionally equivalent numbers of women approached from each of the 150 Australian electorate regions. All women between the ages of 18 and 50 were eligible for participation, irrespective of current or previous OCP use. For the purposes of this article, OCP refers to any combined OCP, but not the minipill (progesterone only) or the emergency contraception pill.
Procedure
The appropriate Institutional Review Board gave approval for the study, and informed consent was obtained for all participants. A study package comprising an invitation letter, participant information sheet, questionnaire, and reply-paid envelope was mailed to 1200 women. As an incentive to participate, women were also provided with a prize draw entry form, which allowed them to enter into a draw to win one of three $50 gift vouchers for a major Australian department store. Based on stipulation from the ethics committee, each package was mailed only once, and women did not receive any reminders for the study. Study recruitment commenced in October 2008 and ended in February 2009.
Materials
Based on a systematic review of the literature, a survey instrument was developed combining both validated and purposely designed scales. Before administration, the questionnaire was pilot-tested with a convenience sample of 16 women in the target age range, with modifications made accordingly. The self-report questionnaire assessed demographic and medical characteristics, as well as current and previous contraceptive practices (Fig. 1). OCP users were asked to indicate their age at the time of initial OCP use, the total duration of OCP use, and any reasons for OCP use, discontinued use, and nonuse (Table 2). A single item asked participants to indicate when they were not attempting to conceive, how often they (or their partners) used some form of birth control during sexual intercourse (response options ranged from 1=never to 5=every time). Participants were also asked to describe their attitude toward the OCP using a 5-point Likert scale ranging from 1 (Very negative) to 5 (Very positive) and their perceived confidence in their knowledge of the risks, benefits, and side effects associated with OCP use (3 items). An overall confidence score was calculated as an average of scores for the three items (α=0.88). The questionnaire also assessed the following. Knowledge of the risks and benefits of OCP use (17 items). Participants indicated whether they thought OCP use decreased, did not affect, or increased the risk of 17 different health issues, listed in Figure 2. A total knowledge score (α=0.77) was calculated by summing correct responses for all items except heart disease, benign breast disease, colorectal cancer, breast cancer, PID, and irregular periods because of the lack of substantive evidence on the association between OCP use and these health issues. Previously accessed or received information (5 items) about the benefits, risks, and side effects associated with OCP use were assessed using four response options (yes, no, unsure, and not applicable). Perceived importance of receiving OCP-related information (1 item) was assessed using a 5-point Likert scale from 0 (Not important at all) to 4 (Extremely important). Sources of OCP-related information were indicated from a list of eight possible sources, including general practitioner (GP) or other doctor, the internet, friends, or family members. Women's questions about the OCP. Eight commonly held OCP-related questions were identified from the literature. In response to each question, participants indicated either that (1) this question had been answered for them, (2) they would like to receive more information about this issue, or (3) the question was not personally relevant. Preferred format for receiving OCP-related information in the future. Women were presented with a list of eight possible patient education materials and a standard definition and were asked to indicate how useful they believed each resource would be, from 0 (Not at all useful) to 4 (Extremely useful). General anxiety and depression. The Hospital Anxiety and Depression Scale (HADS) has two 7-item subscales measuring anxiety and depression.
19
Each item has four response options ranging from 0 (Not at all) to 3 (Very much). Subscale scores ≥8 indicate potentially elevated distress.
19
In this sample, internal consistency was 0.84 and 0.77 for anxiety and depression scores, respectively.

Range of currently used contraceptive methods reported by this sample of Australian women (n=305). *Other includes douching, diaphragm, female condom, spermicide, and those participants who preferred not to respond to this item.
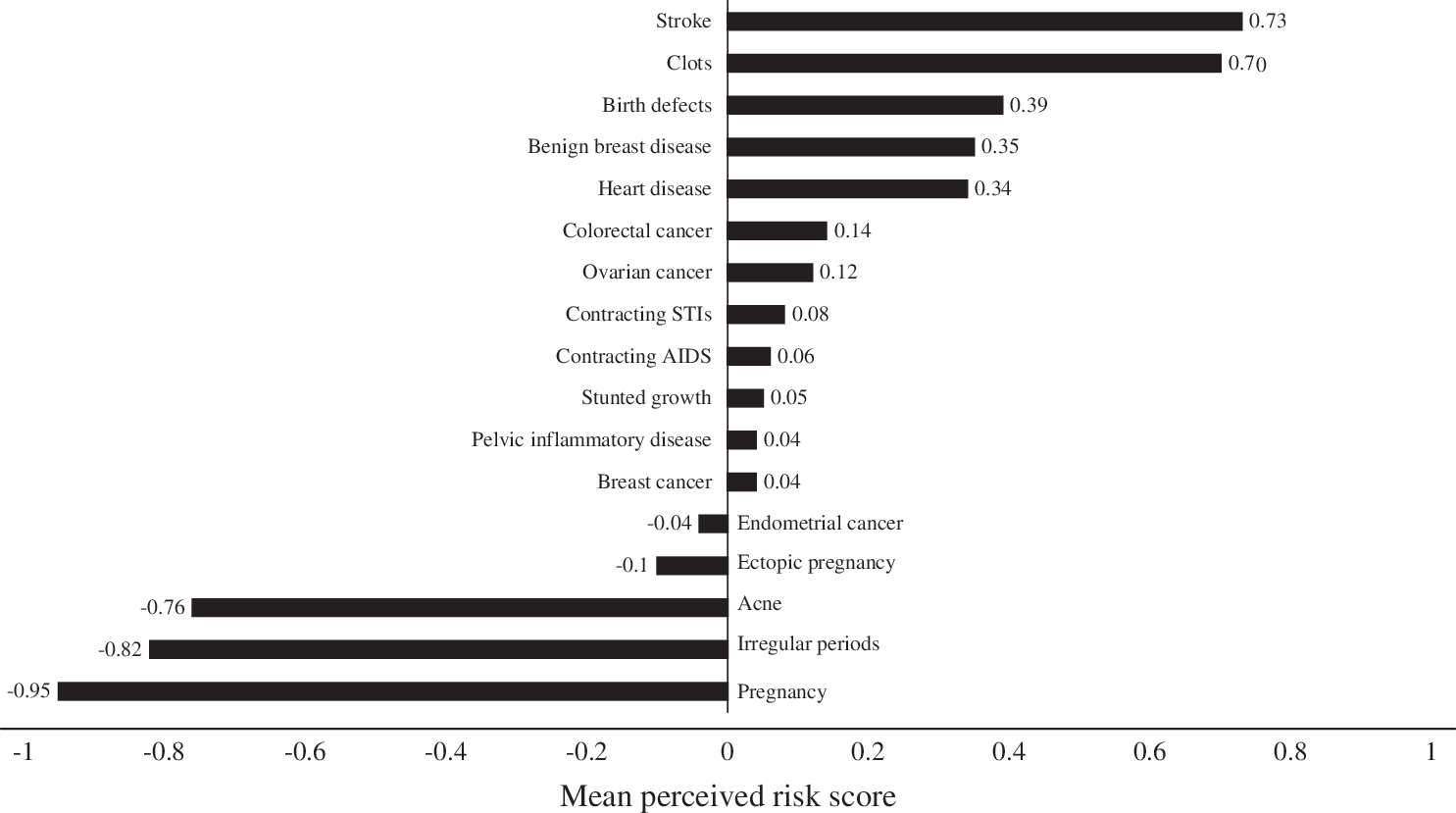
Women's beliefs about the risks and benefits associated with OCP use. OCP, oral contraceptive pill; STIs, sexually transmitted infections.
A copy of the survey instrument can be obtained on request from the research team.
Statistical analysis
Data were analyzed using SPSS 17.0. Descriptive statistics were used to describe the sociodemographic characteristics and OCP-related attitudes and behaviors of the sample. Spearman's rank correlation coefficients (rs ) were used to examine associations between OCP-related knowledge and continuous predictor variables, and Mann-Whitney U tests were used when the predictor variable was binary. Linear regression analysis was used to identify variables that were independently associated with OCP-related knowledge. Predictor variables with p<0.10 in the bivariate analyses were included in the multivariate analysis. A progressive, backward elimination modeling strategy was employed until a final model was obtained containing only variables with p<0.05. Given its importance, age was included in the final regression model as a covariate. Interaction terms were entered into the final model separately, with their corresponding main effects.
Results
Response rates and sample characteristics
Of the 1200 women aged 18–50 years who were sent a study package, 42 packages were returned unopened because of incorrect address details. Of the remaining 1158 women, 305 returned the study questionnaire, yielding a response rate of 26%, which is consistent with similar previous studies. 20 The mean age of the sample was 35.1 years (standard deviation [SD]=9.2), and just over half the sample (59%) had children. The demographic characteristics of the sample are summarized in Table 1.
SD, standard deviation.
Contraceptive practices
Ninety-three percent of women reported using the OCP at some time in their lives. The mean age of women at the onset of OCP use was 18 years (SD=3.2), and the mean duration of usage was 9 years and 7 months (SD=6.5 years). Thirty-two percent of women were currently using the OCP. The most common reasons for OCP use are listed in Table 2, along with participants' reasons for discontinuation of use or nonuse. The reported range of current contraceptive practices among the women is represented pictorially in Figure 1. Overall, 18% of participants indicated they rarely or never used any form of birth control while sexually active and not intending to conceive (of which 49% were aged ≥40 years), and 56% indicated they used some form of birth control almost every time or every time. Further, 31% of women had had an unplanned or surprise pregnancy, and 11% had become pregnant while using oral contraceptives.
OCP, oral contraceptive pill.
Knowledge and beliefs
Overall, 66% of women expressed positive attitudes toward the OCP, with a mean score of 3.76 (SD=1.0, possible range 1–5). In contrast, a small subset of women (11%) conveyed negative attitudes toward the OCP. Figure 2 illustrates participants' beliefs about the association between OCP use and 17 different health issues or disease processes. The mean total knowledge score was 3.88 (SD=1.79) out of a possible 8, with OCP users (mean=3.95, SD=1.75) demonstrating significantly greater knowledge compared to those who had never used the OCP (mean=2.85, SD=2.03) (Z=−2.46, p=0.01). Table 3 shows the percentage of participants who responded correctly to each knowledge item. Approximately one third of the sample indicated they were not at all or only slightly confident in their knowledge of the risks and side effects associated with OCP use (32% and 30%, respectively), and 20% of women indicated a lack of confidence in their knowledge of OCP-related benefits. In contrast, the percentages of women who felt very or extremely confident in their knowledge of OCP benefits, risks, and side effects were 38%, 28%, and 31%, respectively.
n=299 for all items except those indicated by an asterisk.
n=301.
Correlates of knowledge
The results of the bivariate analyses are shown in Table 4. After allowing for age, the mean OCP knowledge score for women with a university degree was 2.20 higher than for those without this educational qualification (p<0.001, 95% confidence interval [CI] 1.49-3.24). The mean OCP knowledge score for married women was 1.74 higher than for women who were not married (p=0.02, 95% CI 1.11-2.72). For every 1 year increase in duration of OCP use, the mean knowledge score increased by 1.06 (p=0.001, 95% CI 1.02-1.09). For every 1 unit increase in mean confidence in OCP knowledge, the mean knowledge score increased by 1.70 (p<0.001, 95% CI 1.38-2.09). Finally, for every 1 unit increase in self-reported depression, the mean knowledge score decreased by 0.93 (p=0.02, 95% CI 0.88-0.99).
Information and support needs
One third of the sample could not recall ever receiving information about the contraceptive benefits associated with OCP use, and more than half (54%) had not received information about its noncontraceptive benefits. A large proportion of women also had not received information about the risks of OCP use (41% and 48%, respectively). Finally, 31% did not recall receiving information about the side effects associated with OCP use. Nineteen percent of the sample was unable to recall receiving information about any of the aforementioned issues, and 31% of the sample recalled receiving information about every issue.
Sixty-five percent of women rated information on the benefits, risks, and side effects associated with OCP use as very or extremely important. Only a small proportion (11%) perceived OCP-related information as not important at all. The majority of participants (84%) had discussed OCP use with a GP or other health professional at some time in their lives. Seventy-four percent of women indicated they had initiated their first discussion about the OCP in a medical setting, and 19% reported GP initiation of this discussion. Further, 63% of women identified their GP or other doctor as being their main source of information, followed by 46% for the information booklet included with the OCP. Other sources of information included friends (15%), magazines (13%), the internet (9%), family (8%), pharmacists (6%), or television (4%). Only 50% of women expressed satisfaction with the quality and quantity of information received about the OCP. Table 5 shows the areas in which women reported a desire for more information.
Of the eight communication strategies presented to participants, Figure 3 shows that an online resource or website containing accurate and up-to-date information about the risks, benefits, and side effects of OCP use was rated as the most preferred option (mean=3.05, SD=1.13), followed by an information booklet (mean=3.02, SD=1.01), and consultation with an expert (mean=2.83, SD=1.13), with a CD-rom being the least preferred option (mean=1.77, SD=1.26).
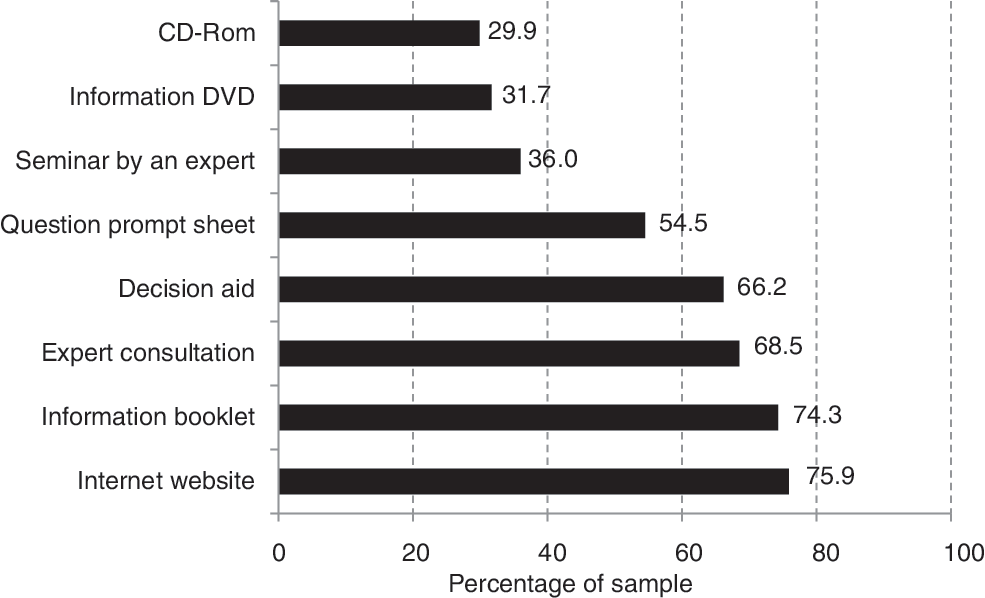
Percentage of participants (n=305) endorsing each potential method of information delivery as very useful or extremely useful.
Discussion
Despite the popularity of the OCP and the frequency of general practitioner consultations involving prescription of the OCP, this study identified a number of shortcomings in women's knowledge of the risks and benefits associated with OCP use. Less than half of the women surveyed were able to correctly identify the increased risks of thrombosis and stroke associated with OCP use, and even fewer women demonstrated knowledge of the noncontraceptive benefits associated with OCP use, such as a reduction in the risk of both ovarian and endometrial cancer. Further, the mean knowledge score for the sample was <4 out of a possible score of 8. Despite this evidence of insufficient knowledge, however, >60% of participants expressed positive attitudes toward the OCP, a result also found in other similar studies. 2,12
A unique aspect of this study was its assessment of women's confidence in their knowledge of the OCP, as well as their satisfaction with previously received or accessed information about the OCP. Low levels of confidence as well as knowledge, coupled with the finding that 50% of participants were dissatisfied with the quality and quantity of available OCP-related information, signal a need for improvement in this area of health education and promotion. For example, the data show that many women still believe that OCP use is unnatural or unhealthy and frequently cite these beliefs as a reason for cessation of OCP use or nonuse. 12,21,22 These beliefs are contrary to medical research supporting the general safety of the OCP 2 and demonstrate the powerful subjective perceptions that may motivate individuals' health behaviors. It was startling to find that almost 20% of women of reproductive age indicated that they rarely or never used any form of birth control while sexually active and not intending to conceive. This indicates that there may be important practical, medical, and attitudinal barriers to the effective use of contraception among women, which may in turn lead to unplanned pregnancies. Approximately one third of the women surveyed indicated they had had an unplanned pregnancy, and 11% of women had become pregnant while using the OCP. This suggests a need for greater education and community awareness about the range of possible contraceptive options currently available to women, along with information about the associated benefits, risks, and side effects of these options.
A number of variables were found to be independently associated with women's knowledge of the health benefits and risks associated with OCP use. Educational level was associated with greater OCP-related knowledge, potentially indicating inequitable access to information between those with and those without a university education. This finding may also be accounted for by the positive link between educational status and health literacy level, whereby women with a higher educational level report greater motivation and ability to gain access to, understand, and use information in ways that promote and maintain good health. 23 Greater duration of OCP use was also found to be positively associated with knowledge, suggesting that women's knowledge is intrinsically linked to their personal experiences over time. Longer use also may have provided a greater number of opportunities to engage in discussions about the OCP with one's general practitioner. Also of interest is the finding that higher depression scores were associated with lower OCP-related knowledge. Future work to better understand this association is warranted and could focus on exploring in greater detail the ways in which depressed mood may interfere with the processing or recall of medical or health-related information.
Study strengths and limitations
The methodology used to ascertain a random sample of women from the Australian population is a strength of this study. Working in collaboration with the AEC, care was taken to recruit women from each Australian state, with proportionally equivalent numbers of women approached from each voting electorate in the country. This strategy ensured adequate representation of as many views and perspectives as possible. Although the response rate for this study was low (26%), this figure is in accordance with previous studies 20 and is likely the result of new ethical requirements for opt-in research, such that women were required to opt-in to the study without reminders from the research team. This opt-in approach has been shown to have markedly lower response rates. 24 The low response rate in the present study may limit the generalizability of the findings and may have influenced the results if women with higher education levels or those with better (or worse) experiences with the OCP were more likely to participate in the study. There is also the possibility of recall bias; that is, participants may not necessarily be accurate in their recollections of whether or not they received information about the risks and benefits associated with OCP use. One means of addressing this issue in the future is to consider the use of a prospective research design. Further, given the cross-sectional design, the data cannot elucidate the causal direction of associations.
Implications for clinical practice and health education
Taken together, these findings are likely to have important implications for clinical practice. By identifying the characteristics of those women most likely to have lower levels of knowledge about the risks and benefits associated with OCP use, clinicians (particularly general practitioners and pharmacists) may target or tailor patient education and counseling to such women. Clinicians could also use Table 5 as a guide for developing a list of frequently asked questions to acknowledge and, if appropriate, address with their patients. The study findings show that women are particularly lacking in knowledge about the noncontraceptive benefits of the OCP (Fig. 2 and Table 3), indicating that women who could be using the OCP to their advantage (e.g., women with a strong family history of ovarian cancer) are perhaps not. This finding combined with the prominence of misconceptions about the OCP demonstrates a need for the design and implementation of more widespread public health messages about the possible health effects of OCP use. It is important that this information be communicated to women in a way that is aligned with their preferences in order to facilitate more accurate and well-informed community opinions, which may lead to an increase in appropriate usage of the OCP.
Future directions
Given the large proportion of women who could not recall receiving or accessing information about the risks and benefits of the OCP, it is critical that the communication strategies developed to inform and educate women on contraceptive-related issues use delivery mechanisms that are considered appropriate and accessible to women. This study provides both scope and direction for the development of educational materials for women considering use of the OCP. These data demonstrate women's preference to receive OCP-related information via an interactive educational website or via a paper-based information booklet, which may be particularly advantageous for those women with limited access to the Internet. Moreover, the findings suggest that general practitioners play an important role in directing women to relevant health information; thus, these clinicians should be closely consulted (along with other health professionals) throughout the development and implementation of new health information tools and resources. The effectiveness of such resources in increasing women's knowledge about the risks and benefits associated with OCP use could be assessed in a randomized controlled trial (RCT), with multiple assessment points to track possible changes in attitudes and contraceptive behaviors over time. Little et al. 25 conducted an RCT to determine if provision of information leaflets or questions on contraception improved knowledge of OCP use in women and found that educational intervention had a significant effect on knowledge. It is possible that such educational interventions could also be used to improve women's knowledge of the health risks and benefits associated with OCP use. Studies of this nature are needed, particularly given the evidence that women tend to rely primarily on printed information for knowledge of OCP effects on health. 26 Finally, women's beliefs and knowledge are also likely to be affected by their personal experience of, and family history of, the conditions affected by OCP use. Studies specifically assessing the knowledge and information needs of women with a family history of different types of cancers and cardiovascular disorders, for example, would be a valuable addition to the literature.
Footnotes
Acknowledgments
We thank the women who generously volunteered their time to participate in this study. We also thank Associate Professor Bettina Meiser for providing valuable feedback on an earlier draft of this article, as well as infrastructure support via the Psychosocial Research Group in the Department of Medical Oncology at Prince of Wales Hospital. We express gratitude to the Australian Electoral Commission for providing access to the Australian Electoral Roll and Ms. Felicity Rea and Dr. Alison Rutstein for administrative support. N.A.K. and C.E.W. are supported by Clinical Research (Australia) Post Doctoral Fellowships from the National Health and Medical Research Council of Australia (ID 510399 and 510421, respectively).
Disclosure Statement
No competing financial interests exist.