
Abstract
Objectives:
To evaluate whether the stressor of perceived discrimination was associated with premenstrual dysphoric disorder (PMDD) and premenstrual symptoms among minority women. This study builds on previous research that found perceived discrimination was positively associated with other psychiatric illnesses.
Methods:
Participants were 2718 Asian, Latina, and black premenopausal women aged 18–40 years who completed the World Mental Health Composite International Diagnostic Interview for the National Latino and Asian American Survey or the National Survey of American Life. Perceived discrimination was assessed with the Everyday Discrimination Scale. DSM-IV-based diagnostic algorithms generated a provisional lifetime diagnosis of PMDD.
Results:
Eighty-three percent of the participants reported experiencing discrimination (due to race, gender, age, height or weight, or other reasons) in their lifetimes. The frequency of perceived discrimination was positively associated with PMDD (odds ratio [OR] 1.08, 95% confidence interval [CI] 1.05-1.10) and premenstrual symptoms (OR 1.04, 95% CI 1.02-1.05), independent of demographic covariates and social desirability. Women reporting gender discrimination (OR 5.18, 95% CI 1.80-14.90), race discrimination (OR 4.14, 95% CI 1.54-11.11), and other forms of discrimination (OR 6.43, 95% CI 2.11-19.65) were significantly more likely than women without experiences of discrimination to have PMDD. Subtle discrimination was more strongly associated with PMDD (OR 1.12, 95% CI 1.01-1.23) than was blatant discrimination (OR 1.04, 95% CI 0.94-1.15).
Conclusions:
This study is the first to demonstrate that perceived discrimination is associated with PMDD and premenstrual symptoms. These findings suggest that the prevalence of these conditions may be lessened by reducing discrimination in women's lives.
Introduction
Premenstrual dysphoric disorder (PMDD) is a chronic psychiatric disorder affecting approximately 8% of American women. 1 The severe affective symptoms of PMDD impair women's functioning and quality of life in the week before menses. Identification of psychosocial risk factors for PMDD, which are perhaps more amenable to intervention than genetic or biologic factors, is a first step toward the reduction of PMDD prevalence in American women. Because ethnic minority women were largely ignored in previous European and American research on psychosocial risk factors for PMDD, 2 –4 the Office for Women's Health Research has prioritized the investigation of PMDD among ethnic minority women. 5
We examined perceived discrimination as a potential psychosocial correlate of PMDD and premenstrual symptoms in ethnic minority women, applying a diathesis-stress model to understand how perceived discrimination might contribute to the development of these conditions. The diathesis-stress model has been applied to explain the etiology of other psychiatric disorders. 6,7 According to this model, each individual has a unique underlying biologic or genetic susceptibility to disease (diathesis) that is acted upon by environmental factors (stress). 8 Variation in the severity of these components explains why some people develop a disease while others remain unaffected.
Although the etiology of PMDD and premenstrual symptoms is unclear, multiple factors, including both internal (diathesis) and external (stress) components, have been linked to these conditions. 9 Several lines of evidence support the applicability of a diathesis-stress model to PMDD. First, compared to women without PMDD, women with PMDD and premenstrual symptoms have been shown to be more likely to manifest signs of biologic vulnerability to disease, including hormonal and genetic abnormalities, prefrontal brain asymmetry, increased sensitivity to light-induced melatonin suppression, and maladaptive neuroendocrine and circulatory responses to stress. 10 –14 Second, general life stress is associated with the prevalence of PMDD and premenstrual symptoms. For example, Swiss women reporting moderate or severe psychologic distress were more likely to suffer from premenstrual syndrome and PMDD compared to women who reported no psychologic distress. 4 In a cohort of young German women, baseline daily hassles scores were positively associated with incident PMDD and subthreshold PMDD. 3 Two studies of American women linked daily stressors and the perception of events as stressful to PMDD prevalence. 13,15 Perceived life stress was found to be positively associated with the severity of premenstrual symptoms as well. 16,17
Studies have not yet considered the stressor of discrimination as a potential risk factor for PMDD. The association between perceived discrimination and mental illness is well documented, however. A meta-analysis demonstrated that perceived discrimination was associated with greater anxiety disorders, major depression and dysthymia, psychosis, substance abuse disorders, depressive symptoms, anxiety symptoms, and posttraumatic stress symptoms. 18 Furthermore, discrimination targeting specific aspects of one's identity, such as race and gender, was positively associated with psychiatric morbidity. 18 Because ethnic minority women are likely to experience discrimination attributable to race and gender, an analysis of the association between these types of discrimination and PMDD is worthwhile.
Subtypes of discrimination have recently emerged as a topic of health research. Subtle discrimination that is “cool, distant, and indirect” is characterized by perceptions of rudeness and unfair treatment. 19 Blatant discrimination that is “hot, close, and direct” describes physical and verbal attacks. 19 Acts of blatant discrimination are less tolerated by mainstream society; as a consequence, subtle discrimination may be more prevalent. 20,21 Subtle discrimination, but not blatant discrimination, was positively associated with depressive symptoms among Asian Americans. 22 An internal attributional style and intense cognitive and emotional processing are associated with experiences of subtle discrimination. 22 –24 Unlike subtle discrimination, blatant discrimination is more easily disregarded through external attributions, and the unambiguous nature of the experience does not engage an individual's cognitive and emotional resources to a comparable degree. 23–24 It seems likely that these differences would lead to a more damaging mental health impact of subtle vs. blatant discrimination.
In summary, we hypothesized that perceived discrimination, particularly race and gender discrimination, would be positively associated with PMDD and premenstrual symptoms in this population. We also hypothesized that subtle discrimination would be more strongly associated with PMDD and premenstrual symptoms than would blatant discrimination.
Materials and Methods
Participants
This analysis included the combined populations of the National Latino and Asian American Survey (NLAAS) 25 and the National Survey of American Life (NSAL). 26 These surveys were conducted with the same core instrument (including discrimination and PMDD modules) and focused on the mental health of Latinos and Asian Americans (NLAAS) and African Americans (NSAL). The surveys were designed to be analyzed jointly with survey weighting and stratification variables provided by the survey investigators. 27 The study population included English-speaking, noninstitutionalized adults (≥age 18). Respondents were selected for inclusion through a multistage probability sampling strategy to achieve nationally representative samples and adequate numbers of racial and ethnic minorities. Although English language proficiency was a requirement for inclusion for the NSAL, NLAAS participants could choose to complete the survey in English, Spanish, Mandarin, Cantonese, Tagalog, or Vietnamese. Interviews were conducted from 2001 through 2003. 25 Response rates ranged from 71% to 80%. Informed consent was obtained from all study participants. 28
Our inclusion criteria were (1) completed the PMDD module, (2) completed the discrimination module, (3) provided premenopausal status, and (4) 18–40 years of age. From 5801 eligible Asian, Latina, and black participants in the NLAAS and NSAL, we excluded 102 Hispanic women from the NSAL who were not given the PMDD module to reduce study costs and 197 women who randomly did not complete the PMDD module. Ten women were excluded for failing to complete the discrimination module. We excluded 1914 women whose periods had stopped permanently or temporarily (for reasons other than pregnancy), 10 women who did not disclose their menopausal status, and 850 older women (>age 40). By limiting our analytic sample to women aged 18–40, we decreased the likelihood of including women who might misreport perimenopausal symptoms as premenstrual symptoms. Our final sample included 2718 women.
Measures
The NLAAS and NSAL used the World Mental Health Composite International Diagnostic Interview (WMH-CIDI), version 3.0. Survey modules corresponded to DSM-IV diagnostic criteria for mood, anxiety, substance use, and other disorders. Algorithms developed by the survey designers yielded valid and reliable diagnoses of these disorders. 29
Predictor variables
Perceived discrimination was constructed from the Everyday Discrimination Scale (EDS) of the Detroit Area Study (α=0.91), which aggregated perceptions of chronic and routine discrimination over the course of an individual's lifetime. 30 The EDS subscale of the Detroit Area Study Discrimination Questionnaire has been validated as a reliable measure of perceived discrimination. 31 Participants rated the frequency of discriminatory events across nine domains; they were asked: In your day-to-day life, how often have any of the following things happened to you? (1) You are treated with less courtesy than other people. (2) You are treated with less respect than other people. (3) You receive poorer service than other people at restaurants or stores. (4) People act as if they think you are not smart. (5) People act as if they are afraid of you. (6) People act as if they think you are dishonest. (7) People act as if you are not as good as they are. (8) You are called names or insulted. (9) You are threatened or harassed. Responses were scored on a 6-point Likert scale ranging from never to almost every day (0–5). As in prior studies, perceived discrimination was analyzed as a continuous score (range 0–45) that accounted for the frequency of experiences within each domain summed over the nine domains; higher scores indicated more frequent experiences. 32 –34 Over 83% of the participants reported experiencing discrimination in their lifetimes; the mean score for perceived discrimination was 9.3 (standard error [SE] 0.25).
Discrimination type is a categorical variable with six levels of response. Women who reported discrimination in at least one domain more frequently than less than once per year were asked to select the most likely reason for this discrimination from five mutually exclusive choices: race (includes national origin or ancestry, race, and skin color), gender, age, height or weight, and other type. Those reporting no experiences of discrimination comprised the sixth response, no discrimination. Women whose experience(s) of discrimination occurred less than once per year were not asked this question (because of a skip pattern in the CIDI) and were consequently dropped from this part of the analysis. The majority of participants attributed discriminatory experiences to their race (60.9%), followed by other reasons (21.7%), height or weight (8.1%), gender (6.8%), and age (2.6%)
The domains of EDS were separated into two subscales that reflected subtle discrimination (e.g., being treated with less courtesy than others and receiving poorer restaurant service than others) and blatant discrimination (e.g., being called names or insulted and being threatened or harassed). Factor analyses have supported this distinction in the EDS domains. 22,23 Again, we summed the frequency of discrimination across the domains to generate a score for subtle discrimination (range 0–20) and for blatant discrimination (range 0–25). The mean scores for subtle discrimination and blatant discrimination were 5.27 (SE 0.12) and 4.02 (SE 0.14), respectively.
Dependent variable
PMDD status had three mutually exclusive levels of response: PMDD, premenstrual symptoms, and the absence of premenstrual symptoms. The lifetime prevalence of PMDD was assessed with the WMH-CIDI Premenstrual Syndrome module, which was based on DSM-IV criteria for PMDD. 35 A woman was positively identified as having PMDD if she reported (in her lifetime): (1) experiencing depressed mood, anxiety, or irritability in the week before her period, (2) experiencing affective symptoms in at least 7 of 12 menstrual cycles (when symptoms were at their most frequent and severe), (3) that these mood changes were worse than normal most of the time, and (4) symptoms, such as difficulty concentrating, tiredness, change in appetite, or change in sleep. She also had to report (5) interference in work, social life, or personal relationships or (6) impairment in daily activities because of these problems. Women with premenstrual symptoms had at least one of the first four symptoms but did not meet criteria for PMDD. Women without symptoms were categorized as having an absence of premenstrual symptoms. The weighted lifetime prevalence of PMDD and premenstrual symptoms was 3.0% and 38.3%, respectively.
Covariates
The covariates included in this analysis correlated with discrimination, premenstrual symptoms, or PMDD. 2,36 –38 These included race, employment status, educational attainment, income (a continuous variable ranging from 0 to 17, calculated by dividing the total family income by the poverty threshold for a family of that size 28 ), self-rated physical health and self-rated mental health (ordinal variables ranging from 0 to 5 indicating health status as poor to excellent), smoking status, current age, history of oral contraceptive use, and the DSM-IV diagnosis of any mood disorder in the past month (includes bipolar depression, dysthymia, hypomania, major depressive disorder, major depressive episode, and mania). Finally, we included a measure of social desirability, the tendency to report information that one thinks others might like to hear. It was assessed with the Crowne-Marlowe scale (ranging from 0 to 10; higher scores indicate greater social desirability). 39
Analytic strategy
SUDAAN 10 was used for all statistical analyses. Taylor Series Linearization procedures in SUDAAN 10 accounted for the clustering and weighting of the Collaborative Psychiatric Epidemiology Surveys (CPES) survey data. 40 Cluster, stratum, and weighting variables were included in the analysis. PROC DESCRIPT and PROC CROSSTAB were used for univariate and bivariate analyses of continuous and categorical variables, respectively. Multinomial logistic regression models (generalized logit) were used to explore the association between each measure of discrimination and PMDD status. In all multinomial logistic regression models, PMDD and premenstrual symptoms were modeled as (separate) outcome events, and no premenstrual symptoms represented the nonevent. Separate unadjusted and multivariate-adjusted multinomial logistic regression models were constructed for each measure of discrimination: (1) perceived discrimination, (2) discrimination type, and (3) subtle discrimination and blatant discrimination. Each multivariate-adjusted model also included all the covariates listed above. The predictor variable(s) and covariates entered each model simultaneously. We used two-tailed Wald-chi-square tests to determine the overall significance of the predictor variables and covariates, and two-tailed t tests for contrasts of individual parameter estimates. Multivariate-adjusted odds ratios (OR) and the 95% confidence intervals (CI) for these effect estimates were also presented. We confirmed that multinomial regression models met established statistical diagnostics 41 and adjusted for multiple comparisons. 42
Results
Participants were mostly Latina (43.7%) or black (40.6%) and averaged 28.8 years (SE 0.23) of age. Participants were mostly employed (60.9%), with a high school education (72.6%), nonsmokers (76.4%), and current or former users of oral contraceptives (63.4%). The prevalence of any DSM-IV diagnosed mood disorder in the past month was 3.0%. On average, participants had relatively high ratings for physical health (mean 3.5, SE 0.03) and mental health (mean 3.9, SE 0.02). Employment status, educational attainment, smoking status, any mood disorder in the past month, history of oral contraceptive use, self-rated physical health, self-rated mental health, current age, and income were significantly associated with PMDD status (p<0.05). These data are presented in Table 1. The demographic and health characteristics of the women in our cohort resembled those in a nationally representative sample of ethnic minority women who were surveyed for the 2004 Current Population Survey (CPS). 43
Unweighted n (weighted %) for categorical variables and mean standard error (SE) for continuous variables. Numbers may not sum to total because of missing data; percents weighted with national survey weights.
p value is from Wald chi-square test.
PMDD, premenstrual dysphoric disorder.
As hypothesized, perceived discrimination was significantly associated with the lifetime prevalence of PMDD (p<0.0001) and premenstrual symptoms (p<0.0001). Mean discrimination scores increased with increasing premenstrual symptomatology (Table 2). As shown in Figure 1, the multivariate-adjusted odds of experiencing PMDD increased by 8% for each 1-unit increase in the frequency of perceived discrimination (OR 1.08, 95% CI 1.05-1.10), and the odds of experiencing premenstrual symptoms increased by 4% for each 1-unit increase in the frequency of perceived discrimination (OR 1.04, 95% CI 1.02-1.05). These effects were independent of race, employment status, educational attainment, income, self-rated physical health, smoking status, current age, oral contraceptive use, self-rated mental health, diagnosis of past month mood disorder, and social desirability. Notably, statistical control for these demographic covariates did not alter the association between perceived discrimination and PMDD status. The unadjusted ORs (not shown) are essentially identical to the adjusted ORs presented in Table 3, which suggests that demographic factors did not account for the observed association between perceived discrimination and PMDD status.
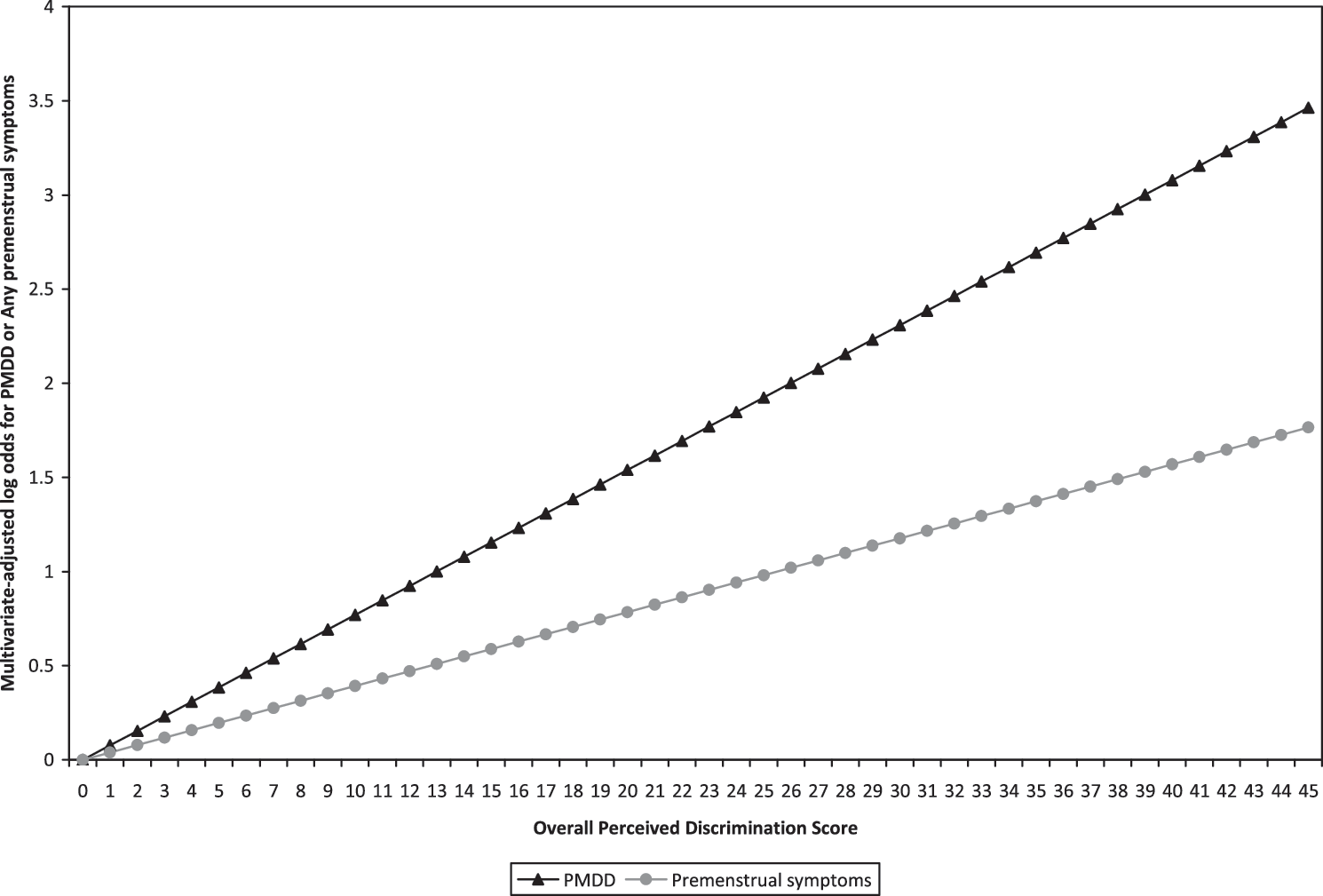
The frequency of perceived discrimination and the likelihood for premenstrual dysphoric disorder (PMDD) and premenstrual symptoms among ethnic minority women. We present the multivariate-adjusted log adds for these associations; these values were calculated by multiplying the natural log of each odds ratio (OR) [ln (1.08)for PMDD and ln (1.04) for premenstrual symptoms; or “beta”] by the overall perceived discrimination score. Effects are independent of race, employment status, education, income, self-rated physical health, smoking status, current age, oral contraceptive use, self-rated mental health, diagnosis of past month mood disorder, and social desirability.
Unweighted n (weighted %) for categorical variables and mean (SE) for continuous variables. Numbers may not sum to total because of missing data; percents were weighted with national survey weights.
p value is from Wald chi-square test.
Three separate multivariate-adjusted multinomial logistic regression models were constructed to test the relationship between each discrimination variable and PMDD status. Model 1 included perceived discrimination, model 2 included discrimination type, and model 3 included measures of both subtle discrimination and blatant discrimination. In addition to these main predictor variables, each model also included all the demographic covariates (age, race, educational attainment, employment status, smoking status, history of oral contraceptive use, self-rated physical health, self-rated mental health, diagnosis of mood disorder in the past month, and income) and a measure of social desirability.
Nonevent.
Odds ratio (OR) (adjusted). Multivariate-adjusted ORs are independent of age, race, educational attainment, employment status, smoking status, history of oral contraceptive use, self-rated physical health, self-rated mental health, diagnosis of mood disorder in the past month, income, and social desirability.
p<0.05; ** p<0.01, *** p<0.001.
Consistent with our hypothesis, women reporting discrimination due to gender (OR 5.18, 95% CI 1.80-14.90, p=0.0025) and discrimination due to race (OR 4.14, 95% CI 1.54-11.11, p=0.0051) were significantly more likely to experience PMDD compared to women who did not report discrimination. Similarly, discrimination due to gender (p=0.0007) and discrimination due to race (p=0.0023) were significantly associated with reporting premenstrual symptoms independent of demographic covariates and social desirability (Table 3).
Reporting discrimination due to other reasons was also associated with PMDD (OR 6.43, 95% CI 2.11-19.65, p=0.0012) and premenstrual symptoms (OR 2.27, 95% CI 1.61-3.19, p=0.0002). In an effort to identify the possible types of discrimination that were encompassed by the label, other reasons, we explored whether sexual orientation (discrimination toward gays, lesbians, and bisexuals), income and education (discrimination based on social class), and religious affiliation (religious discrimination) were associated with selecting other reasons rather than race, gender, age, and height or weight among persons who experienced discrimination. Sexual orientation, income, and education were not significantly associated with selecting other reasons for discrimination, nor were race, gender, age, and height or weight. However, we found that women who were members of marginalized religious minority groups in America 44 (e.g. non-Christian affiliations, such as Rastafarian, Jewish, Muslim, and Hindu) were more likely to attribute experiences of discrimination to other reasons rather than race, gender, age, and height or weight compared to women who identified as a member of a majority group 44 (e.g., Christian denominations or agnostics/atheists/no religious affiliation; OR 1.69, 95% CI 1.08-2.63). This finding suggested that other reasons for discrimination may have actually reflected experiences of religious discrimination in this sample.
As hypothesized, subtle discrimination was more strongly associated with PMDD and premenstrual symptoms than was blatant discrimination (Table 3 and Fig. 2). Furthermore, only subtle discrimination (p=0.0026) and not blatant discrimination (p=0.6910) was significantly associated with PMDD status. This pattern was observed in both the unadjusted models and the multivariate-adjusted model. Adjustment for covariates had a negligible impact on the association between these discrimination measures and PMDD status (unadjusted results not shown), indicating that the relationships among subtle discrimination, blatant discrimination, and PMDD status were not accounted for by demographic factors or social desirability.
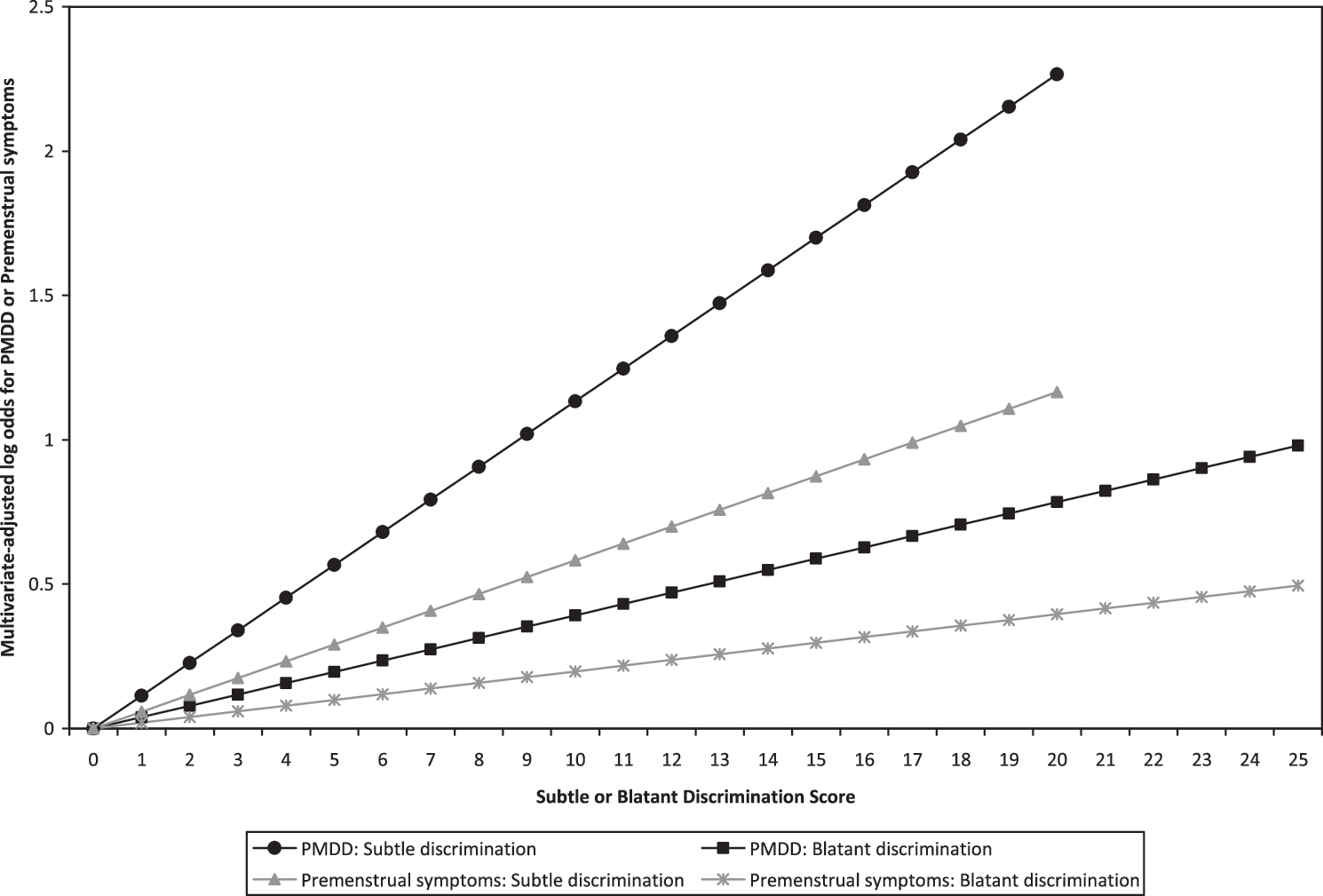
The frequency of subtle and blatant discrimination and the likelihood of PMDD and premenstrual symptoms in ethnic minority women. We present the multivariate-adjusted log odds for these associations; effects are independent of race, employment status, education, income, self-rated physical health, smoking status, current age, oral contraceptive use, self-rated mental health, diagnosis of past month mood disorder, and social desirability.
Discussion
This study demonstrated for the first time that perceived discrimination, discrimination due to race, gender, or other reasons, and subtle discrimination elevated ethnic minority women's odds of experiencing PMDD and premenstrual symptoms. These results were concordant with existing literature that shows a positive association between discrimination and mental illness. 18 Furthermore, our discrimination findings add to the body of work demonstrating that stress (in the form of general life stress 3,4,13,15 and traumatic events 3,45 ) contributes to PMDD. Thus, according to the diathesis-stress model, perceived discrimination may be an environmental stressor that acts on existing biologic or genetic vulnerabilities to exacerbate premenstrual symptoms and eventually bring about the full symptomatology of the disorder.
A meta-analysis demonstrated that gender discrimination and race discrimination were equally deleterious to mental health. 18 We also found that gender and race discrimination are both correlated with PMDD. This suggests that minority women may be exposed to at least two types of discrimination that can contribute to their experience of PMDD. Other studies have found that lifetime assessments of discrimination are less strongly tied to other mental health outcomes than assessments of recent discrimination. 18 Consequently, our findings related to lifetime gender and race discrimination may have underestimated the association between these types of perceived discrimination and PMDD. Also, in our study, participants were allowed to select only one reason for the discrimination they experienced over their lifetimes. It is likely that some participants were exposed to discrimination targeting multiple aspects of their identity, which may differentially impact participants' vulnerability to PMDD. In future studies it will be important to examine how recent gender and race discrimination relate to PMDD.
We found that subtle discrimination but not blatant discrimination was significantly associated with reporting PMDD and premenstrual symptoms. This finding extended prior results demonstrating that subtle discrimination was a stronger predictor of depression than was blatant discrimination. 22 As discussed previously, subtle discrimination may be more stressful because these experiences engage more intense cognitive appraisals than experiences of blatant discrimination. Subtle discrimination is associated with an internal attributional style that may negatively impact an individual's self-esteem, whereas blatant discrimination is associated with an external attributional style that is less harmful to individuals' self-esteem. 23,24 Self-esteem is negatively associated with major depression 46 and menopausal symptoms 47 and, thus, may also be correlated with PMDD. Although episodes of blatant discrimination are generally decreasing, there has been an escalation in episodes of subtle discrimination in society. 26 Our study suggests this trend could have pernicious consequences for women's mental health.
Our findings linking perceived discrimination with PMDD status are consistent with a diathesis-stress model of PMDD. The chronic, unpredictable, and uncontrollable experiences of discrimination may provoke maladaptive physiologic and psychologic responses that could lead to the development of PMDD and premenstrual symptoms in biologically vulnerable women. The process by which discrimination could influence PMDD is not yet known, but several studies are suggestive of a biologic mechanism. For example, women with PMDD are more physiologically reactive to stress compared to controls. 48,49 Evidence also suggests that PMDD, like major depressive disorder, is associated with dysfunction in the serotonergic system. 50 As the serotonergic system is sensitive to environmental stressors, particularly in women, 51 this pathway may represent a mechanism linking perceived discrimination to PMDD. Studies also support the role of other neurotransmitters and steroids in the etiology of PMDD, 52 and these may represent additional biologic mechanisms linking perceived discrimination to PMDD status.
Our study has a number of strengths. This is the first study to examine the association between perceived discrimination and PMDD status. Second, we focused on ethnic minority women because they have been left out of the majority of PMDD studies. Third, the participants in our analytic sample were drawn from a nationally representative sample of Latino, Asian, and black women; the sample included adequate numbers of first-generation, second-generation, and third-generation Americans. Thus, our results are likely to generalize to other populations of American ethnic minority women. Fourth, we demonstrated that discrimination was associated with PMDD beyond other social-contextual stressors by controlling for poverty and physical health as well as other potential confounders. Fifth, we minimized the potential effect of reporting bias by statistically controlling for social desirability. To minimize the possible effect of current mental states on symptom reporting, multivariate models also included a measure of self-rated mental health and an indicator of past month mood disorders.
Sixth, we explored whether a lifetime history of any mood disorder would affect our findings, as disorders are often comorbid with PMDD. 53,54 Statistical control for this variable had no effect on the relationship between any measure of discrimination and PMDD status (analyses not shown). Seventh, we limited our sample to premenopausal women less than age 40 with regular menstrual periods; such women were unlikely to be perimenopausal or menopausal. Consequently, this strategy lessened the likelihood that participants mistakenly reported perimenopausal or menopausal symptoms as premenstrual symptoms. Finally, PMDD status was evaluated with an established diagnostic module. 3,45
Limitations of the study are as follows. First, the data were cross-sectional; thus, we could not establish whether perceived discrimination preceded the onset of premenstrual symptoms or PMDD or determine if the observed associations were of a causal nature. Because this measure of discrimination assessed lifetime experiences, however, it is likely that the measure captured experiences of discrimination that predated the onset of PMDD, which women usually develop in their late 20s through early 30s. Second, the WMH-CIDI yielded a provisional rather than conclusive diagnosis of PMDD because the module addressed two of the four DSM-IV diagnostic criteria for PMDD. The module content adequately assessed criterion A (the cyclical recurrence of affective and somatic symptoms in the week before the onset of menses) and criterion B (these symptoms cause substantial impairment and interfere with functioning), whereas criteria C and D were not assessed. Criterion C states that these affective symptoms cannot be the premenstrual exacerbation of an existing psychiatric illness; rather the symptoms must be discretely linked to the menstrual cycle (PMDD may be comorbid with another disorder, however). Although we statistically controlled for lifetime history of mood disorders in our analyses, this approach does not fully account for criterion C, which may be best assessed by clinician interview. Finally, criterion D states that criteria A, B, and C must be confirmed over two consecutive menstrual cycles. The CIDI could not address criterion D because the survey was administered at a single point in time. Despite these limitations, the WMH-CIDI module yielded prevalence estimates of PMDD that were similar to those obtained through prospective assessments. 56 Research should further examine the relationship between different types of discrimination and PMDD with a more detailed assessment of PMDD among different cohorts of women to confirm the associations that we have found and report for the first time in this investigation.
Conclusion
Perceived discrimination was associated with PMDD and premenstrual symptoms among ethnic minority women; our findings extended literature linking discrimination to mental health and stress to PMDD status. Perceived discrimination may be particularly toxic to ethnic minority women in three forms: (1) as a chronic exposure, (2) when targeting two aspects of their identity, race and gender, and, (3) in its subtle form. To understand and identify the mechanism(s) linking perceived discrimination to PMDD, future studies should incorporate longitudinal designs with prospective assessments of PMDD, detailed inventories of discriminatory experiences, and biologic measures. Temporal changes in discrimination may also affect these relationships and, thus, require further study in contemporary cohorts. With a greater understanding of the etiology of PMDD, clinicians may target those factors most amenable to intervention and reduce the prevalence of PMDD and its associated disability.
Footnotes
Acknowledgments
We thank Dr. Haiqun Lin, Dr. Kimberly Ann Yonkers, Dr. Jhumka Gupta, and Dr. Elizabeth Bertone-Johnson for providing helpful feedback on drafts of this article. This research was funded by the National Institute on Aging grant 5 T32 AG00153.
Disclosure Statement
The authors have no competing financial interests.