
Abstract
Objective:
Women have exhibited anaphylaxis, urticaria/angioedema, and autoimmune progesterone dermatitis (APD) coinciding with the progesterone premenstrual rise. We report a detailed immunological evaluation of such a woman responsive to a gonadotropin hormone-releasing agonist (GHRA).
Methods:
Skin testing, enzyme-linked immunosorbent assays (ELISAs), leukocyte histamine release (LHR), and inhibition assays were performed to demonstrate progesterone immunoresponsiveness.
Results:
Serum specific-progesterone immunoglobulin G (IgG) and IgE were detected initially and disappeared 6 months after GHRA treatment. Dose-response LHR using patient basophils was observed for different hormones but after 3 months persisted only for 5β-pregnanediol. Preincubation with mouse antiprogesterone monoclonal antibody (PmAb) or mifepristone, a progesterone inhibitor, over a range of doses inhibited specific progesterone-induced LHR. Experiments with varying progesterone concentrations and a fixed dose of anti-IgE resulted in 100% LHR at a concentration as low as 0.016 nmol/mL, which, without anti-IgE, failed to release histamine.
Conclusions:
This is the first report of combined recurrent anaphylaxis, cyclic urticaria/angioedema, and APD induced by immunoresponsiveness to progesterone.
Introduction
Women of childbearing age may exhibit a variety of premenstrual allergic symptoms coincidental with the cyclic rise of progesterone about 5–7 days before menses. The spectrum of symptoms noted at such times includes anaphylaxis, cyclic urticaria/angioedema, and autoimmune progesterone dermatitis (APD), all of which suggest possible immune mediation(s). 1 –23 Although past case reports documenting these clinical manifestations focused attention on specific skin and in vitro tests, the precise role of adaptive immune responses in these syndromes is as yet problematic. 1,9,14,20,24
Over the past 21 years, we have had the unique opportunity to observe a patient who experienced anaphylactic episodes that began during administration of an estrogen-progesterone birth control pill (BCP). Detailed in vitro and in vivo immunological studies were performed to define the immunopathogenesis of her life-threatening responses followed by cyclic urticaria/angioedema and APD that required long-term treatment with the gonadotropin hormone-releasing agonist (GHRA) naferelin.
Case Report
A 48-year-old, white, nulliparous, and atopic woman was originally evaluated because of a 6-month history of oligomenorrhea and polycystic ovary syndrome at the age of 26. To regulate the menstrual cycle and frequent rupture of ovarian cysts, the patient was placed on a BCP (norethindrone 0.5, 0.75, and 1.0 mg each for 7 days plus ethinyl estradiol 35 μg; Ortho-Novum 777®). Within 2 days of beginning this drug, she experienced acute onset of labiofacial edema, bronchospasm, and hypotension. The BCP was discontinued for 1 week and then restarted; 2 weeks later, the patient had a similar reaction. Three subsequent anaphylactic episodes occurred over a 2-month period, each with increased intensity and duration. The reactions occurred 8–12 hours after ingestion of the BCP but subsided after the BCP was discontinued.
A complete history and clinical and laboratory evaluation were conducted to exclude all known causes of anaphylaxis/chronic urticaria/angioedema. A survey for possible cancer, which included a chest x-ray, mammogram, Papanicolaou cervical smear, ultrasound of the pelvis, and endometrial biopsy, was negative. Laboratory tests, including complete blood count (CBC); sedimentation rate; antinuclear antibody (ANA) and thyroid autoantibodies; a complete complement profile; tryptase level; renal, liver, and bone panels; and 24-hour urine for 5-hydroxyindoleacetic acid and histamine, were within normal limits. Total immunoglobulin E (IgE) and specific IgE to house dust mite and ragweed were modestly elevated. These tests, as well as all the progesterone immunological assays, were completed before institution of GHRA therapy.
A number of key occurrences during her 21-year clinical course are noteworthy. Premenstrual urticaria at times associated with angioedema has persisted until the present time. To minimize and prevent life-threatening symptoms, naferelin (400 μg/day) was started 15 months after the initial anaphylactic episode. Although this was projected to be a short-term palliative approach, the persistence and severity of symptoms necessitated long-term control of progesterone secretion, which was generally lower when adequate doses of naferelin were administered. Naferelin dosage was either reduced or discontinued when the patient appeared to be clinically improved; unfortunately, however, recurrence of severe symptoms frequently required resumption of the suppressive naferelin dosage (400 μg/day). Since its inception, complete cessation of nafarelin was achieved sporadically for 3.6 years of a total of 21 years of therapy. Therefore, the patient was closely monitored for osteoporosis, which fortunately has not appeared. Interestingly, sporadic progesterone serum levels did not always reflect the expected therapeutic effects of naferelin. A cyclic appearance of a maculopapular dermatitis of her face and neck was first noted in January 1999, and a petechial rash appeared in mid-2005. A biopsy of this lesion was interpreted as showing nonspecific perivascular lymphocyte infiltration consistent with a drug reaction but also similar in appearance to previously reported micropathology of APD (Fig. 1). 8,11,21
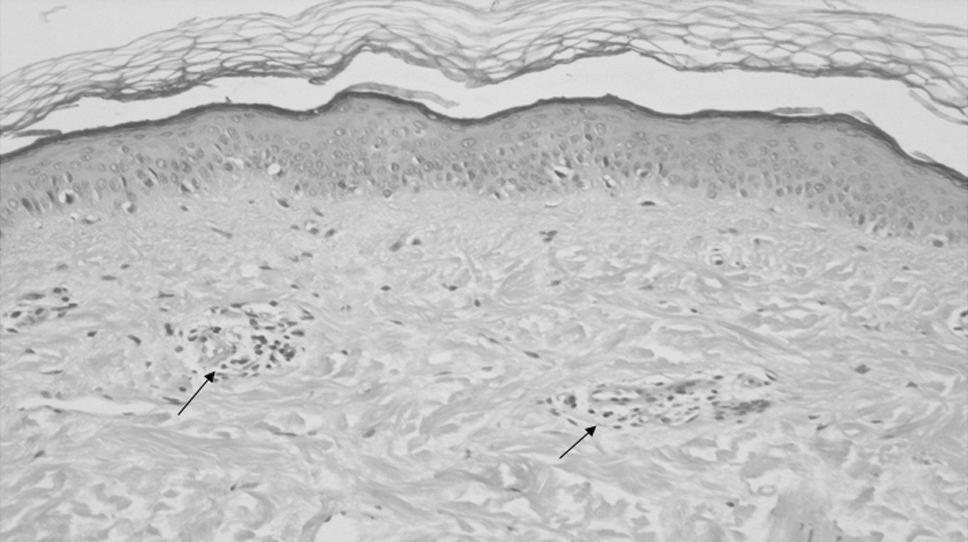
Histopathology of a petechial lesion associated with patient's autoimmune progesterone dermatitis (APD) in 2005. *Note perivascular accumulation of lymphocytes in the dermis (black arrows). This finding is nonspecific but is consistent with either a drug reaction or APD.
Materials and Methods
Skin testing
Investigations were performed to determine the possible roles of estrogen, progesterone, its major metabolite 5β-pregnanediol, and components of the BCP in the pathogenesis of the life-threatening anaphylaxis and subsequent manifestations of cyclic urticaria/angioedema and APD. Percutaneous prick/puncture (P/P) skin testing was performed with progesterone (3.0–32 nmol/mL), 5β-pregnanediol (0.35–17.3 nmol/mL), estradiol (3.5–35 nmol/mL), norethindrone (0.35–35 nmol/mL), and Ortho-Novum-777. The steroid hormones were prepared by dissolving small amounts of each in 95% ethanol and diluted further with phosphate-buffered saline (PBS) to achieve the appropriate concentrations. Histamine diphosphate 1 mg/mL, 95% ethanol, and PBS were used as control skin test reagents. Intracutaneous tests were not done because of the severity and number of recent anaphylactic events.
Immunological assays
In vitro immunological tests included a direct leukocyte histamine release (LHR) assay, which was performed by a modification of the method of Lichtenstein and Osler 25 and enzyme-linked immunosorbent assays (ELISA) according to a technique described by Loizou et al. 26 The latter tests used polystyrene microtiter plates coated with progesterone-bovine serum albumin (P-BSA)-conjugated antigen. Stepwise incubations with serum, antihuman goat IgE or IgG, antigoat IgE or IgG alkaline phosphatase, followed by the substrate p-nitrophenol phosphate were carried out.
Results
Percutaneous testing for all hormone skin test unconjugated reagents prepared in ethanol solutions, as well as the dissolved components in the BCP preparation used by the patient, did not elicit a positive response (Table 1a). In vitro immunological assays were performed 1 month after the patient's most recent anaphylactic episode and discontinuation of the BCP. Table 1a shows serial results of maximum LHR induced by the optimal dose within the dose-response spectrum of each hormonal reagent incubated with the patient's basophils. In these experiments, a dose-dependent LHR response at least 3 standard deviations (SD) greater than the mean percent LHR of the asymptomatic controls (n=16) was considered significant. Repetition of this test 3 months after the BCP had been discontinued also showed a significant LHR response to 5β-pregnanediol, the major metabolite of progesterone. Norethindrone, ethinyl estradiol, and the combination of these drugs in the BCP also induced LHR but to a lesser extent than observed in response to either progesterone or 5β-pregnanediol. Four months after discontinuation of the BCP, a minimal LHR response (4%) was induced by both progesterone and estrogen. Six years later during treatment with naferelin, progesterone no longer induced LHR.
BSA control, enzyme-linked immunosorbent assay of bovine serum albumin (BSA) carrier protein alone.
Mean±3 standard deviations.
IgE, immunoglobulin E; IgG, immunoglobulin G; LHR, leukocyte histamine release; —, not done.
Inhibition experiments were performed 3 months after discontinuation of the BCP. Preincubation with a mouse antiprogesterone-specific monoclonal antibody (PmAb) with doses ranging from 0.001 to 1.0 μg/mL inhibited specific progesterone-induced LHR at the dose of 160 nmol/mL of progesterone, which alone induced a maximum LHR of 91% (Table 2). Inhibition of progesterone-induced LHR was also observed at all concentrations of mifepristone, a progesterone competitive inhibitor, but was maximum (94%) at the preincubation concentration of 10 nmol/mL.
To determine if an interaction between progesterone and IgE membrane receptors existed, various concentrations of progesterone were co-incubated with a fixed concentration of anti-IgE (1:1000) (Table 3). Anti-IgE (1:1000) alone stimulated 76% LHR from the patient's leukocytes. However, co-incubation of varying concentrations of progesterone with anti-IgE resulted in 100% LHR with all five concentrations of progesterone, even at the lowest concentration (0.016 nmol/mL), which, in the absence of anti-IgE, failed to release histamine. ELISA assays using haptenic progesterone alone did not show evidence of either specific IgG or IgE antibodies. Using a commercial P-BSA conjugate, both IgG and IgE antibodies were detected in the patient's serum obtained 3 months after the last anaphylactic episode (Table 1b) that occurred after BCP was discontinued. A specific IgG response was still noted 3 years but not 6 years later; specific IgE levels were equivocal at 3 and 6 years after the initial episodes. Recently, the reliability of ELISA IgG and IgE assays using P-BSA conjugates has been confirmed. 27
Discussion
To our knowledge, this is the first report of a woman with combined symptoms consistent with recurrent anaphylaxis, cyclic urticaria/angioedema, and APD induced by progesterone, thereby providing a unique opportunity to investigate the role of immune mechanisms in each of these conditions. The patient's initial symptoms of anaphylaxis were temporally associated with oral BCP pills, but persistence of symptoms over a 21-year span most likely occurred because of subsequent cross-sensitization to endogenous progesterone. Throughout this long-term observation, partial control of her premenstrual flares was accomplished by intranasal GHRA. The finding of several specific adaptive immune responses to progesterone strongly suggested a partial immunopathogenetic basis for this unusual evolution of symptoms.
Not surprising was the fact that P/P skin tests to ethanol extracts of the BCP, progesterone, and 5β-pregnanediol were negative in view of their small molecular weight sizes. Evidence for IgE-mediated anaphylactic episodes was documented by the presence of two in vitro correlates: (1) specific progesterone-induced LHR in a dose-response fashion and (2) serum progesterone-specific IgE, both of which disappeared during treatment with naferelin. Smaller amounts of LHR were also observed after challenge with norethindrone (17%) and estradiol (24%), suggesting that both ingredients in the BCP could have been partially implicated in the patient's initial anaphylactic occurrences. The fact that both progesterone and its major metabolite, 5β-pregnanediol, induced much higher levels of LHR (86% and 67%, respectively) suggests that her original anaphylactic response to norethindrone in the BCP ultimately led to endogenous progesterone cross-sensitization to a greater degree of activity than the synthetic progestin itself. Both direct and indirect LHR induced by progesterone have been demonstrated previously. 5,7,10,13 There was a single negative report of LHR in several patients with idiopathic anaphylaxis. 14 This prior investigation is not comparable because leukocytes were challenged with a single, high dose (0.25 μm/mL) of progesterone and not methoxyprogesterone, the agent that provoked systemic symptoms in three of the patients after intracutaneous injections. Of note, the observation that LHR occurred at four concentrations (160, 16, 1.6, 0.16 nmol/mL) of progesterone could account for direct LHR induced by unconjugated test reagents.
Subsequent clinical reactions appeared almost entirely during the patient's menstrual luteal phases, implying a minimal role of the follicular estradiol hormone. Persistence of IgE-mediated anaphylactic episodes during her clinical course may be partially explained by recently described immunomodulatory properties of progesterone that upregulate progesterone membrane receptor α (PHRα) on CD8+ cells and alter the T helper 1/T helper 2 (Th1/Th2) cytokine profile in favor of the Th2 response. 28 In addition, progesterone may activate an inhibitory G-coupled protein on T cells, further enhancing the progesterone immunomodulatory response. 29
Immunological specificity was demonstrated by preincubation of the patient's leukocytes with a broad dose range of mouse PmAb (0.001–1 μg/mL), resulting in 68%–100% inhibition of LHR (Table 2). A remarkable feature of these LHR experiments was enhancement of anti-IgE-induced LHR by 5 log dilutions of progesterone, including the lowest dose that alone did not induce LHR (Table 3). This effect is similar to the basophil priming effects of several cytokines and insulin growth factor in enhancing mediator release from basophils, contrasted with marked inhibition of LHR by glucocorticosteroids. 30,31 Further, the almost complete inhibition (94%) of progesterone-induced LHR by the progesterone competitive inhibitor, mifepristone, at a concentration of 10 nmol/mL suggests that there may be cross-activation of the intracytoplasmic and nuclear progesterone receptors and the IgE membrane receptor. 32 Cross-talk with one or both membrane progesterone receptors (mPHRα, mPHRβ) is also possible, thereby creating an ideal in vitro milieu for enhanced presentation of receptor-bound progesterone to adjacent specific IgE antibody bound to membrane IgE receptors. These potential pathways may account for LHR induced by unconjugated immune reagents in this study. It is possible that progesterone-specific IgG antibodies could also have contributed to LHR by stimulating the activation domain FcγIIA subtype IgG receptor on basophils. 33,34 These immune interactions occurred in the context of a known atopic patient whose basophils were at greater risk than normal basophils for being triggered. 35 Once activated, basophils secrete interleukin-3 (IL-3), an autocrine primer of basophils, which could contribute to even greater releasability. 36
If the indicated factors are indeed operative, why were the skin tests negative? Very few small molecular weight substances, particularly water-insoluble ones, elicit positive skin tests unless they are conjugated to peptides or proteins. In past case reports, positive skin tests were noted only at relatively high progesterone concentrations, and many tests were performed without appropriate solvent controls or establishment of a subirritant, intracutaneous threshold in normal subjects. 1,24 The majority of positive skin tests used as diagnostic adjuncts for APD were administered by endodermal or subdermal routes and caused 24–48-hour delayed reactions, which in some instances were due to oily vehicles. 1 The fact that negative skin tests have also been observed in some cases of APD indicates that progesterone skin testing has not been standardized and, therefore, is not a reliable predictor of progesterone-induced hypersensitivity phenomena. 1,18,20,24
Apart from the biopsy appearance of a dermal lymphocytic perivascular infiltrate (Fig. 1), which is also observed in chronic autoimmune urticaria, we have no objective evidence about the immunological basis of the patient's chronic maculopapular dermatitis. Although originally designated as autoimmune because it was associated with late skin responses to progesterone in sesame oil and positive intracutaneous skin tests, the objective evidence of autoimmune mechanisms is scant, if any. Specific IgG antibodies were present in our patient, but these disappeared before the dermatitis occurred. There has been one report of APD preceding ulcerative colitis as an extraintestinal manifestation. 12 There was a single report of APD in association with a positive leukocyte migration inhibition test. 5 In vitro release of interferon-γ (IFN-γ) from progesterone-stimulated peripheral blood mononuclear cells (PBMCs) suggested a Th1-type cytokine response. 6 A Th1-type cytokine pathway might be expected, although not yet demonstrated, to be associated with rare exacerbations of pustular psoriasis during the second trimester of pregnancy. 37 In contrast, progesterone induced the production of IL-4 and IL-13 in PBMCs from allergic rhinitis patients, suggesting, as in our case, that progesterone favors Th2 rather than Th1 immune responses. 38 Hormonal exacerbation of other Th2-mediated skin diseases, such as atopic dermatitis, has also been reported. 39 Reconciliation of these disparate clinical findings is not yet possible, and it is evident that the underlying mechanisms in APD remain to be determined.
Possible treatment options for the severe life-threatening symptoms manifested by our patient are listed in Table 4. None of the immunomodulatory agents have yet been tried. One of the anovulatory approaches appeared to and ultimately proved to offer optimal efficacy for the complex symptom triad in our patient. Nafarelin suppressed her life-threatening anaphylactic episodes within a few months and also ameliorated the severity of her cyclic urticaria/angioedema for the past 20 years. Because in vitro immunological results in our patient suggested that mifepristone might be beneficial, a future therapeutic trial of this agent might be warranted. Several gynecological consultants declined to perform the ablation procedure as long as the patient's symptoms were controlled by Nafarelin. Treatment efficacy of nonanaphylactic diseases induced or exacerbated by progesterone by any of the approaches in Table 4 has not yet been determined, and, therefore, they are not recommended.
GHRA, gonadotropin hormone-releasing agonist.
Footnotes
Acknowledgments
We gratefully acknowledge the excellent technical expertise of Dr. John Scinto, Dr. Joan Gallagher, and Ms. Mary Enrione (deceased) for the initial immunological assays and Rebecca Martin and Jocelyn Biagini-Meyers for the ELISA tests. The patient, L.E., has provided written consent to allow publication of this case.
Disclosure Statement
The authors have no conflicts of interest to report.