
Abstract
Objective:
To describe and compare breast and cervical cancer screening among women in Barcelona in 1992, 2001, and 2006 by social class, age, and screening approach.
Methods:
This was a study of trends based on analysis of Barcelona health interview surveys for the years 1992 (n=5,003), 2001 (n=10,030), and 2006 (n=6,050). Dependent variables were having regular mammographies (at least every 2 years) and having regular cytologic testing (at least every 3 years). Independent variables were age, social class, and survey year. A descriptive analysis was carried out. To compare prevalence in terms of social class and the years studied, we calculated prevalence differences (PD) and prevalence ratios (PR) by fitting robust Poisson regression models.
Results:
In 1992, women aged 40–49 had more regular mammographies than those aged 50–69, with social class inequalities in both age groups. Having cervical cancer screening was more common than having breast cancer screening, with prevalence varying from 46.4% in the low social classes to 59.2% in the high classes. In 2001, breast cancer screening had risen, particularly in women aged 50–69, a tendency that had stabilized by 2006. Inequalities diminished over the period, more markedly in women aged 50–69; PRs of 1.22 and 1.58, respectively, for high and middle social classes with respect to the lowest class in 1992 fell to PRs of 1.07 and 1.08, respectively, in 2006. In the case of cervical cancer screening, inequalities also diminished but not to the same extent.
Conclusions:
Preventive screening for breast and cervical cancer has increased, and the population screening program for breast cancer among women aged 50–69 years appears to contribute more than opportunistic screening for cervical cancer in reducing social class inequalities.
Introduction
The main aim of screening, for those types of cancer amenable to early detection, is to contribute to reduction mortality. 1,2 In the case of breast cancer, however, this contribution has been debated and questioned recently. Results are not conclusive, and the studies have important limitations, mainly because of the difficulty of finding appropriate comparison groups. It is difficult to discern if the decrease in mortality is a result of screening or better treatments for breast cancer. 3,4 The decision to set up screening and the methods used (population-based or opportunistic) depends, among other factors, on where the balance lies between the risks and benefits of each, 5 apart from the cost-effectiveness considerations. 6 One of the main risks associated with screening is the high percentage of false positives, 7,8 false negatives, and benign cancers, 9 –11 as well as overdiagnosis and overtreatment. 12,13
The population-based approach implies greater equity in opportunity of participating in the screening, as it offers access on equal terms to the whole target population. 14,15 A study conducted recently comparing various European countries where cervical and breast cancer screening is done using different approaches (opportunistic and populational) found that socioeconomic inequalities are greater in countries where opportunistic screening is implemented. 16
In Barcelona, cervical cancer screening is of the opportunistic type. The target population is women aged 25–64 years; the first two screening cytologic tests are performed annually, then subsequently every 3 years up to age 64. 17 Breast cancer screening, begun in late 1995, is population-based, targeting women aged 50–69 years, who are invited for screening every 2 years. 18
The five health interview surveys conducted in Barcelona since 1983 allow the prevalence of screening to be compared between years and permit studying social class inequalities. In the last three surveys, it was possible to follow up the regular mammographic and cytologic tests women undergo. Thus, we can investigate the way in which the type of screening approach influences the prevalence of screening and the inequalities in it. The aim of the present study was to describe and compare breast and cervical cancer screening among adult women resident in Barcelona city in the years 1992, 2001, and 2006 by social class, age, and screening approach.
Material and Methods
Design, study population, and sources of information
A study of trends was carried out by analysis of three cross-sectional health surveys. The study population consisted of noninstitutionalized women residents of Barcelona city aged 25–69 years in the years 1992, 2001, and 2006. The information was obtained from Barcelona Health Surveys (Enquesta de Salut de Barcelona [ESB]) corresponding to the years 1992, 2001, and 2006. Each year, a sample stratified by district was obtained; sample sizes were 5,003 persons in 1992, 10,030 in 2001, and 6,050 in 2006. Data were collected through interviews held at the subject's home by trained interviewers. 19 Nonrespondents were substituted by women of the same age and district in order to maintain the characteristics of the sample.
Variables studied
The dependent variables studied were: having breast cancer screening (i.e., women who state having a mammogram at least every 2 years) and having cervical cancer screening (at least every 3 years); both variables were dichotomous (yes/no). The independent variables used were social class, age, and year of survey. Social class was obtained based on the woman's occupation where possible or, otherwise, that of her partner. We used the Spanish adaptation of the British classification elaborated by the Spanish Epidemiological Society, 20 grouping together classes I–II (as high), class III (middle), and classes IV–V (low). Age was grouped as follows: 40–49 years and 50–69 years for breast cancer screening, and 25–64 years for cervical cancer screening.
Data analysis
All analyses were weighted to take into account the sample design. We performed a descriptive analysis of the sample of women in terms of social class and age group in each survey. Prevalences of undergoing regular breast and cervical cancer screening were calculated for all three health surveys. Prevalence of cervical screening was standardized by age, and prevalence of breast screening was stratified into the following age groups: 40–49 years and 50–69 years (Table 1). In addition, these prevalences were calculated stratified by social class (Table 2).
Weighted sample.
DK/NA, Don't know/Not applicable.
Sample weighted and age-adjusted.
95% CI, 95% confidence interval; PD, prevalence difference; PR, prevalence ratio.
To study changes in prevalence over the years (Table 2), we calculated age-adjusted prevalence ratios (PR) and prevalence differences (PD) and their 95% confidence intervals (CI), comparing different years (2001 compared to 1992, and 2006 compared to 2001) for each social class and type of screening. The PRs and CIs were calculated by fitting robust Poisson regression models, 21 where dependent variables were preventive practices, and independent variables were age, social class, and year. To assess changes in social class inequalities, PR and PD and their 95% CI comparing social classes (with class IV–V as the reference category) were calculated for each year, also including age in the Poisson models (Table 3). To determine if social class inequalities changed over the years studied, the interaction between social class and survey year was included in the models.
Sample weighted and age-adjusted.
p, p value between ESB, 1992, and ESB, 2001; ** p, p value between ESB, 2001, and ESB, 2006.
All analyses were conducted using the statistical package STATA/SE version 10.1 (StataCorp, College Station, TX).
Results
Table 1 details the distribution of social classes among the women of the sample, by age group and survey year (number of women and percentage). The women aged 40–69 years, studied in the three surveys, were mostly of low social class, although their percentage decreased over time (from 53.0% in 1992 to 46.6% in 2006), whereas those of the other classes rose, particularly the middle class. The distribution of women aged 25–64 years by social class was similar to that of the women aged 40–69 except that the proportions of middle-class and high-class women are slightly higher, as the youngest women mostly fall into these classes.
Table 1 also shows the prevalence of having breast and cervical cancer screening by age group and survey year. Even though in 1992, more women attended regularly for cervical cancer screening than for breast cancer screening, the proportion having regular breast screening increased over time, particularly among women aged 50–69 years, and eventually exceeded that of cervical cancer screening. The proportion of women aged 40–69 years who declared having regular breast screening in 1992 was 29.2%, rising to 75.9% in 2001 and then to 81.3% in 2006. By age groups, in 1992 and 2001, women aged 40–49 underwent regular screening more often, but by 2006 this situation had reversed, with 71.0% of women aged 40–49 years and 87.8% of those aged 50–69 having a breast cancer screening at least every 2 years. An important increase is observed in the proportion of women declaring having a cervical cancer screening at least every 3 years, rising from 52.6% in 1992 to 75.6% in 2006.
Table 2 and Figure 1 show how the prevalence of regular cervical and breast cancer screening has changed in the different age groups and social class groups over the 3 years studied. Between 1992 and 2001, there was an important increase in undergoing periodic breast and cervical cancer screening, which was larger for breast screening among women 50–69 years, who form part of the population targeted by screening programs, particularly in the lower social class groups. Thus, the PD of having breast cancer screening, comparing 2001 and 1992, in low social class women aged 50–69 was 49.0, and the PR was 3.45 (95% CI 2.81-4.24). Between 1992 and 2001, the prevalence of cervical cancer screening also increased, although not as much as for regular breast cancer screening. The PR values for 2001 with respect to 1992 ranged from 1.54 (95% CI 1.39-1.69) in women of low social class to 1.37 (95% CI 1.23-1.52) in those of the highest social class.
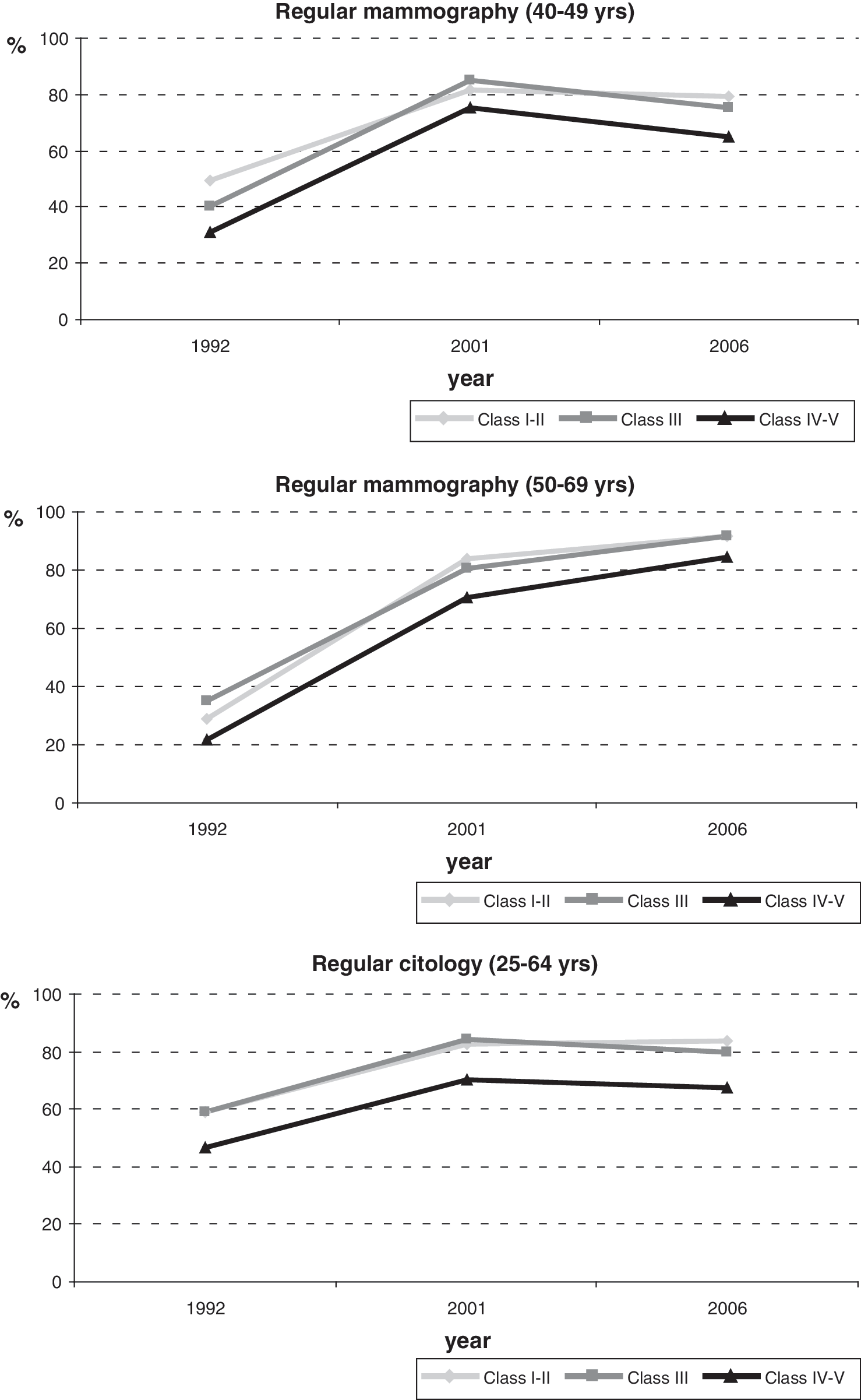
Trends in having regular breast and cervical cancer screening by social class. Barcelona Health Interview Surveys, 1992, 2001, and 2006.
Between 2001 and 2006, the proportion of women of the different social classes who had regular cervical cancer screening, as well as that of women aged 40–49 years who had regular breast cancer screening, remained constant. In contrast, among women aged 50–69 years, the prevalence of regular breast cancer screening rose in all social classes, particularly among the lowest social class, with a PR of 1.17 (95% CI 1.09-1.25) when comparing 2006 with respect to 2001. In 1992, women of the highest social classes had more regular screening, both for breast cancer among the group aged 40–49 (49.4% in the high social class vs. 31.3% in the low social class) and for cervical cancer (59.2% in the high social class vs. 46.4% in the low social class). In women aged 50–69 years, it is noteworthy that middle-class women underwent regular breast cancer screening most often (35.1%).
Table 3 presents inequalities by social class (PR and PD) for the 3 years studied. In 1992, there were clear social class inequalities, the largest of which corresponds to receipt of breast cancer screening among women aged 40–49 years (PR 1.69, 95% CI 1.22-2.36 comparing social classes I–II and IV–V). In those aged 50–69 years, it was the middle-class women who most frequently reported having regular screening (PR 1.58, 95% CI 1.15-2.17). Over time, these inequalities declined gradually, although not significantly, achieving PR values around 1 in 2006. This is different from the case of cervical cancer screening, for which inequalities had increased slightly in 2006 compared to 2001, and the inequalities observed were still significant (PR 1.23, 95% CI 1.14-1.32 comparing women of social class I–II to those of the most disadvantaged class).
PD between social classes decreased in the case of breast screening, albeit evolving differently depending on age group. Thus, in the group aged 40–49 years, between 1992 and 2001 there was an important reduction, particularly among the lower classes (PD 18.1 in 1992 and PD 6.4 in 2001), followed by a rise in 2006. In those aged 50–69 years, taking the lower social class group as reference, there was a rise in 2001 but a reduction again in 2006. In the case of cervical cancer screening, a period of stability up to 2001 was followed by a slight increase in 2006, mostly in the most disadvantaged classes.
Discussion
Screening of both breast and cervical cancer has increased over time, although more notably among women aged 50–69 for breast screening. Meanwhile, inequalities by social class in regular breast cancer screening have declined over the three surveys studied. This is particularly so among women aged 50–69, who because of their higher risk, constitute the target population of most breast cancer screening programs, 22 including that of Barcelona. In contrast, with an opportunistic screening program operating in Barcelona, a slight increase in inequalities in cervical cancer screening was observed in 2006.
Cancer screening programs, among other initiatives, have doubtless played an important role in these overall positive results, which may also be related to a declining trend in mortality from breast and cervical cancer observed in our setting, 23,24 although the contribution of screening to this reduction in mortality is often difficult to establish. 25,26 Moreover, the fact that different approaches are used (i.e., population-based screening for breast cancer, opportunistic screening for cervical cancer) raises the question of the influence this difference may have in the various evolutions observed for these screenings.
In spite of the controversy and constructive debate surrounding screening programs generated in recent years, they are still the best tools for secondary prevention, 27 not only for reducing premature mortality from breast and cervical cancer but also for facilitating less aggressive treatment of the women diagnosed. 28 Overdiagnosis can be a limitation, however, 10 it is important to perform cancer screening according to evidence-based recommendations in order to obtain benefits and minimize harm.
The program of early breast cancer screening in Barcelona began its pilot phase in 1995 and has been implemented gradually over 8 years; it was not until 2004 that all women of the target population had been invited at least once. 29 Although we did not know which surveyed women participated in the program, the results of this study suggest that the program has contributed to reducing social class inequalities, as these inequalities diminished more in women of the age group that is the target population of the program (50–69 years) than in the other age group and more than in cervical cancer screening. It is worth mentioning that previous reports show that women's participation rates in the program are higher in deprived neighbourhoods, 30 –32 implying that the program itself has contributed to the participation of women in these poor areas, a fact that probably also reduces social class inequalities in screening.
According to World Health Organization (WHO) estimates, 33 organized cervical cancer screening can reduce the risk of cancer by 80%–98% depending on program coverage. Organized cervical cancer programs are more effective than opportunistic screening, 34 as the latter may miss women at highest risk, they cannot control the clinical and diagnostic quality of the process because they cannot be systematically evaluated, and there is less control over the adverse effects intrinsic to any screening process. 35,36 It is not always easy to decide which is the best approach, however, because many factors must be taken into account. Such factors include those linked with screening itself, described by Wilson and Jungner, 37 and basically related to the importance of the disease in terms of severity or prevalence, availability of an appropriate screening test, and, of course, ability to influence the outcome of the disease. The unequal distribution of the disease in the world and adequate cost-effectiveness are also important. Breast cancer is most common in developed countries, whereas in the case of cervical cancer, the situation is reversed. 38 Moreover, the human papillomavirus (HPV) presents new challenges for implementation of cervical cancer screening. 34 These facts led to the decision not to implement a population-based program for cervical cancer screening in Catalonia 39 but rather to conduct a highly protocolized opportunistic screening conducted by, among others, primary care professionals and those of the Sexual and Reproductive Health Programme. 17 Various health education programs in different settings probably have contributed to increased awareness among both professionals and the population, contributing to the generally favorable results seen in the uptake of screening practices by women in Barcelona.
The main strength of the present work is that it provides real, objective, and comparable data on the population-based evolution of the two types of screening in our setting.
One limitation of the study is that nonrespondents were substituted for by women of the same age and district, and we cannot rule out some bias. However, we think that by including women of the same age group and district, the main sample characteristics were maintained. Another limitation is that the most vulnerable and inaccessible population groups are probably underrepresented, and they are the ones exposed to the worst circumstances and social determinants. Finally, a third limitation concerns the validity of the information provided by women, especially in the case of cervical cancer screening, but there are no other sources or records to compare with our results. In breast cancer screening, the results found are similar to those obtained by the screening program of the city.
Conclusions
In Barcelona, screening for breast and cervical cancer has increased. Moreover, the population screening program for breast cancer among women aged 50–69 years appears to contribute more than opportunistic screening of cervical cancer in reducing social class inequalities. Both breast and cervical cancer screening programs have a long history of implementation in our society and are well known by the majority of the population and health professionals. Monitoring the trends and social class inequalities of screening prevalence should be a priority of policymakers and technicians involved in these programs.
Footnotes
Acknowledgments
This article is part of the Ph.D. dissertation of Rosa Puigpinós-Riera in the Doctoral Programme in Public Health, University of Barcelona.
Disclosure Statement
The authors have no conflicts of interests to report.