
Abstract
Background:
Osteoporosis is very common in older women in the United States. Osteoporotic fractures cause significant morbidity and mortality, as well as high healthcare costs. Since 2002, the United States Preventive Services Task Force (USPSTF) has recommended screening for osteoporosis of all women aged ≥65. Our objective was to determine adherence to osteoporosis screening guidelines by primary care internists in a large academic medical center and to assess if adherence varies based on provider gender or practice location.
Methods:
This was a retrospective electronic medical record (EMR) review. All women aged ≥65 who were seen in the General Internal Medicine Center (GIMC) or the Women's Health Care Center (WHCC) at the University of Washington Medical Center by internal medicine attending physicians between January 1, 2006, and February 2, 2008, were included in the study. We determined if the patient had a dual energy x-ray absorptiometry (DEXA) study in the EMR database. We calculated the percentage of patients screened per provider and also compared the rate of screening for male vs. female providers and for GIMC vs. WHCC providers.
Results:
Of the 1363 women included in the study, 70% had documentation of a DEXA study. Adherence to screening recommendations for individual providers varied from 33% to 100%. Screening was more likely to occur in the WHCC than in the GIMC (79.2% vs. 66.7%, p<0.001). Although women providers were more likely to screen than their male counterparts (72.2% vs. 66.1%, p=0.023), this relationship did not hold true after excluding women providers from the WHCC.
Conclusions:
We found good adherence to the USPSTF 2002 guidelines for osteoporosis screening in women aged ≥65 years by primary care physicians in a large urban academic medical center. The practice site and not gender of the provider resulted in significantly different screening rates.
Introduction
Osteoporosis is a disease defined by low bone mass, skeletal fragility, and increased risk of fracture. Approximately 8 million women>age 50 in the United States have osteoporosis, 1,2 and about 50% of postmenopausal women will suffer from an osteoporosis-related fracture during their lifetime. 3,4 Those at greatest risk are women aged ≥65.
Bone mineral density (BMD) is a major predictor of fracture risk. 5 –7 There are now fracture risk calculators, such as the FRAX® tool, that improve fracture risk estimation by integrating clinical risk factors and BMD. 8 Although studies are limited, data suggest that BMD screening decreases the risk of fracture by at least 25% 9,10 and increases the likelihood that women will start medication for osteoporosis and comply with osteoporosis therapy. 11 Treatment of osteoporosis decreases fracture risk as much as 50%, based on numerous randomized controlled trials. 12 Estimates of the number needed to screen to prevent one osteoporotic vertebral fracture and one hip fracture are 248 and 741, respectively. 13
In 2002, the U.S. Preventive Services Task Force (USPSTF) recommended that all women ≥65 years should be screened for osteoporosis. 13 Universal screening of women aged ≥65 has been recommended by other organizations as well. 14 –18 Despite these recommendations for osteoporosis screening, many women are not being screened, and, therefore, the condition is underdiagnosed. 19
U.S. physicians suboptimally screen individuals at high risk for osteoporosis. Primary care physicians' screening rates for women aged ≥65 range from 11% to 62%. 20 –24 Curtis et al. 25 found that although the rates of BMD testing with dual energy x-ray absorptiometry (DEXA) in women aged ≥65 increased by 50% between 1999 and 2005, the overall screening rate remained low at 30%. One study reported that 46% of women aged ≥65 had BMD testing in 10 primary care clinics (5 hospital based and 5 community based) affiliated with an academic medical center. This rate increased to 55% when screening criteria also included women who were taking an osteoporosis medication. 24 A recent study performed at a university-based academic geriatric practice reported the highest screening rate of 64%. 26
Few studies have been performed evaluating independent predictors of BMD screening. Three, based on databases as opposed to surveys, found that female providers have higher rates of screening compared to male providers. 24,27,28 Solomon et al. 24 found a wide variation in guideline adherence by practice site not explained by patient case mix. The site with the highest proportion of adherence specialized in women's health.
Our study was designed to determine how well physicians in a large urban academic medical center adhere to the USPSTF 20002 guidelines for osteoporosis screening in women aged ≥65 years. We also wanted to determine if the rates of screening differed based on physician gender or clinic practice site, the General Internal Medicine Center (GIMC) vs. the Women's Health Care Center (WHCC).
Materials and Methods
The Medical Information Networked Database (MIND) at University of Washington Medical Center (UWMC), a system that stores the records of>1.9 million UWMC patients, was accessed. All women aged≥65 who were seen in the GIMC or the WHCC at UWMC by internal medicine attending physicians between January 1, 2006, and February 2, 2008, were included in the study. The GIMC is an internal medicine residency and medical student teaching clinic staffed by internists and nurse practitioners. Attending physicians split their time between direct patient care and overseeing care provided by resident physicians and medical students. The WHCC is staffed by internists, gynecologists, and nurse practitioners. The attending physicians participate in direct patient care, as well as medical student and resident oversight. The gynecologists have their own primary care practices separate from the internists. The only time a gynecologist sees an internist's patient (either from GIMC or WHCC) is as a consultant for a gynecologic problem. There were 8 female and 15 male internal medicine attending physicians in the GIMC and 5 female internal medicine attendings in the WHCC. We excluded patients whose primary care provider was a gynecologist, nurse practitioner, or resident physician.
A total of 1363 of women were included in the study. We determined which of these women had had BMD testing with DEXA within the previous 15 years, regardless of the physician who ordered the test. Our electronic medical record (EMR) does not have the capability to provide prompts for healthcare maintenance screening or prevention. Tables were constructed that display the number of women seen in the clinic and the percentage of these patients who had BMD testing performed, based on attending physician gender and clinic practice site (GIMC vs. WHCC). Figure 1 illustrates the number of women seen and the number who underwent BMD testing per individual physician. Using chi-square analysis, we compared the percentage of women in this population who were screened for osteoporosis based on provider gender and clinic practice site.
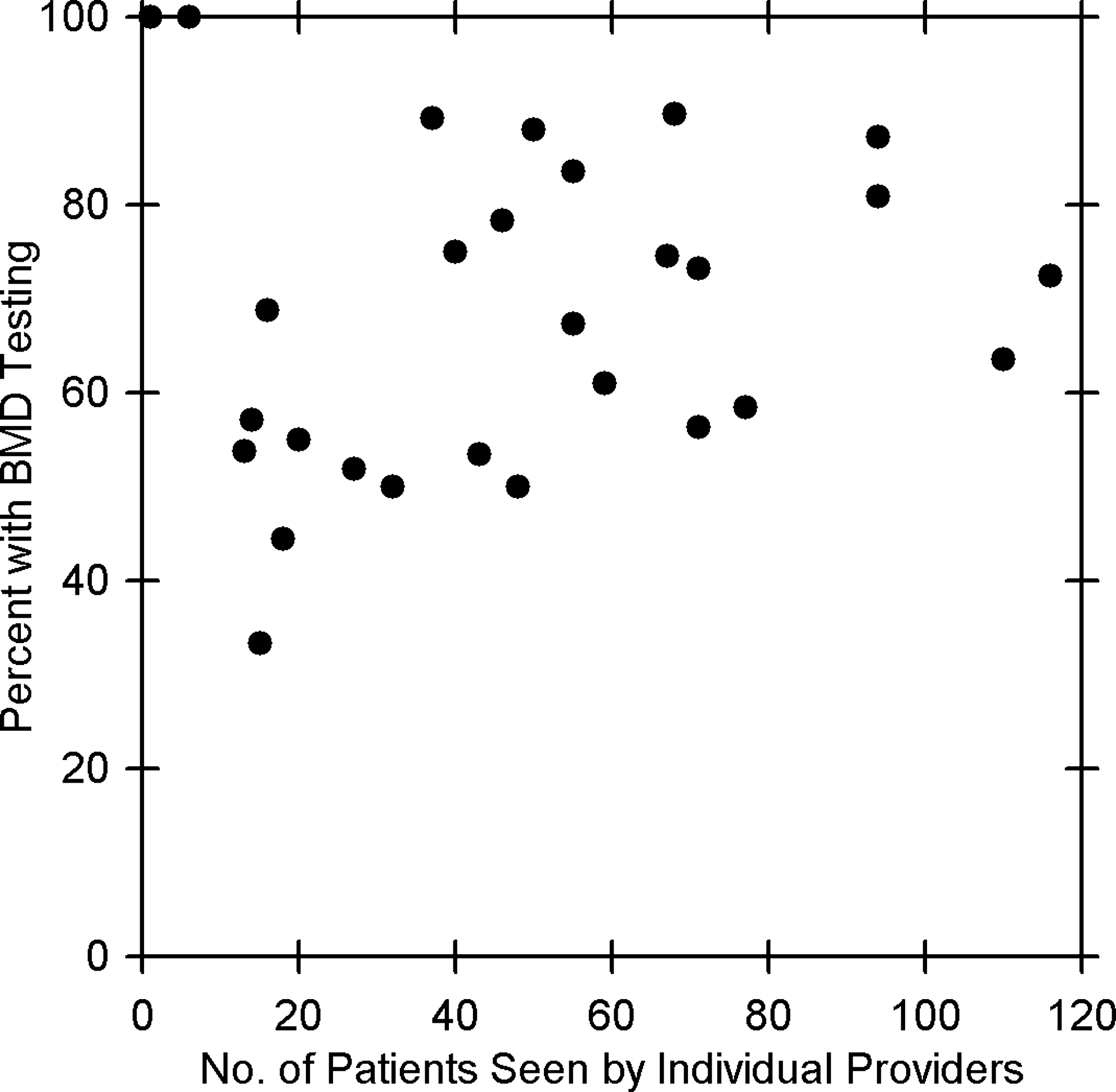
Percent of patients screened by individual providers (r=0.157). BMD, bone mineral density.
Results
The overall rate of screening of women aged ≥65 years with BMD testing was significantly higher in the WHCC, at 79.2%, than in the GIMC, at 66.7% (p<0.001) (Table 1). The rates of screening based on gender of the physician were 72.2% for female physicians (including female physicians in the GIMC and WHCC) and 66.1% for male physicians (p=0.023) (Table 2).
BMD, bone mineral density; GIMC, General Internal Medicine Center; WHCC, Women's Health Care Center.
When the screening rates of the female providers in the GIMC and WHCC were compared, the providers in WHCC screened at a significantly higher rate of 79.2% compared to 67.3% in the GIMC (p<0.001). The number of study patients seen by an individual provider during the study period ranged widely, from 1 to 116. The proportion of patients screened by an individual provider varied from 33% to 100%. There was no correlation (r=0.157) between the number of patients seen by individual physicians and the percentage of patients they screened (Fig. 1).
Discussion
We found that our screening rates for osteoporosis in women aged ≥65 were higher than reported in previous studies and ranged from 66.7% in the GIMC to 79.2% in the WHCC. These high rates of screening may be due to the academic setting, as both the GIMC and WHCC are teaching sites for residents and medical students. In the GIMC, attending physicians participate in weekly, 30-minute, preclinic didactic sessions, which address important topics in primary care. Osteoporosis prevention, screening, and treatment are discussed once every 2–3 years. Also, two faculty members, one in GIMC and one in WHCC, are editors of an educational osteoporosis website, which may have increased awareness of osteoporosis. Our higher screening rates may also be a result of changes in perceived standard of care among primary care providers in general. Many previously published screening studies were done before publication of the 2002 USPSTF guidelines. Although some earlier guidelines recommended screening for asymptomatic women ≥65 years, the USPSTF may be more influential in affecting clinical practice for primary care physicians.
We did not review individual records to determine why women did not have a DEXA study (in our database), but there may be several reasons for this. First, BMD testing may have been recommended by the patient's physician, but the patient declined. The patient may have agreed to have it done but never had it scheduled or did not show up for a scheduled test. In one study, it was found that physicians ordered BMD tests in 76% of patients, but 12% of these patients did not undergo testing despite having a radiology unit at the clinic site. 26 Second, patients with multiple comorbidities may not have been considered candidates for screening. McNally et al. 26 found that in a geriatrics clinic, BMD testing rates were inversely associated with cognitive and functional status. Third, patients may have had BMD testing at an outside facility, so it was not in our database. There are several reasons for this scenario: (1) patients at high risk for osteoporosis (taking corticosteroids) may be followed by subspecialists in the community, (2) women may receive their preventive care from a gynecologist, internist, or family physician in the community, or (3) the patient may have found it was more convenient to have the study in the community rather than at UWMC.
Other reasons for not screening patients may be that BMD testing would not change the patient's management. Examples include (1) women who have had a fragility fracture or a compression fracture and are already being treated for osteoporosis, (2) women who are being treated based on multiple risk factors alone, (3) women who have contraindications to medications for treatment of osteoporosis, (4) women who could not afford medication, (5) women who do not want to take medication due to fear of polypharmacy, drug interactions, or adverse side effects, and (6) women with stage 4 or 5 kidney disease.
We found it interesting that the physicians in the WHCC had significantly higher screening rates than either the female or male physicians in the GIMC. The reason for this is unclear, but it may be that physicians in the WHCC have a greater proportion of postmenopausal women in their practices, and screening for osteoporosis is more likely to be on their agenda. The WHCC may attract women who are more proactive when it comes to preventive services compared to women who are seen in the GIMC. A study designed to identify physician characteristics associated with use of bone densitometry in a health maintenance organization (HMO) found that female provider gender and a greater percentage of women >age 50 in a practice were independent predictors of BMD use. 27 Another study of 10 primary care practices affiliated with a large academic center found that there was a wide variation in guideline adherence by practice site. The clinic site that specialized in women's health had the highest adherence to BMD testing. 24 The study also found that patients seen by female physicians were more likely to have had BMD testing. A cross-sectional survey of primary care physicians in New England found that one of the physician characteristics associated with lower rates of screening was physicians who see a low proportion of postmenopausal women. 29
We also speculate that the women seen in the GIMC have more comorbidities and may be a sicker population than the women seen in the WHCC. This may result in less testing in the GIMC for the multiple reasons discussed on why physicians may not have ordered a DEXA. Another possible reason why screening rates were lower in the GIMC than in the WHCC is that many women in the GIMC continue to get preventive care by a gynecologist in the community. Women who receive care from an internist at the WHCC expect the internist to provide both primary care and preventive care.
Conclusions
We found fairly good adherence to the USPSTF 2002 guidelines for osteoporosis screening in women aged ≥65 years in a large urban academic GIMC and WHCC. We do not know what an optimal screening rate is, as no organizations have provided or recommended benchmark or target goals. We found that the practice site and not the gender of the provider caused significantly different screening rates. There was a higher rate of screening by internal medicine physicians in the WHCC compared to the physicians in the GIMC. Futures studies are needed to determine what factors influence BMD testing of postmenopausal women by physicians and how these can be addressed to improve diagnosing and treating osteoporosis. As healthcare reform places more emphasis on preventive care, there is hope that screening for this important disease will continue to improve.
Footnotes
Acknowledgments
We thank David Rankin and Steve Clements, Senior Computer Specialists at UW Medicine IT services, for helping us extract the data from the Medical Information Network Database. We also thank Doug Schaad, Professor and Divisional Head of Medical Education and Biomedical Informatics at UW, for performing the statistical analyses.
Disclosure Statement
No competing financial interests exist.