
Abstract
Background:
Disparities in the management of coronary artery disease were consistently documented in blacks and women in the 1980s and 1990s. Our objective was to determine if racial/ethnic and sex differences in the use of coronary revascularization persist in a more recent cohort.
Methods:
We examined all 20,604 Medicare beneficiaries admitted for acute coronary syndrome in 2001 from a random sample of 750,000 enrollees that was oversampled for black and Hispanic subjects to assess any cardiac revascularization.
Results:
After controlling for demographics and comorbidities, black men and women (odds ratios [OR] 0.47, 0.40), Hispanic men and women (ORs 0.61, 0.52), and white women (OR 0.67) had lower rates of revascularization compared with white men. Lower revascularization rates persisted for white women (OR 0.67) and black men and women (OR 0.55 and 0.54), controlling for income status and geographic variation, but were no longer present in the Hispanic population.
Conclusion:
The mechanisms by which disparities operate may differ for Hispanic and black populations.
Introduction
Extensive literature has documented disparities in the evaluation and management of coronary artery disease by sex and black race. In the 1980s and 1990s, multiple trials and registries revealed that black populations and women were less likely to receive invasive evaluation and revascularization for acute coronary syndromes. 1 –4 Whether these disparities in care extend to the Hispanic population is unclear, in part because few databases have sufficient power to separately address this population. 5 Moreover, the impact of the widespread use of coronary stents on sex and racial differences in patients undergoing percutaneous coronary intervention (PCI) is unknown. Therefore, using a large database with sufficient Hispanic and black subjects, we sought to learn if previously documented disparities by both sex and race/ethnicity in rates of intervention had declined or persisted into the new millennium.
Methods
To study possible sex and racial/ethnic disparities in Medicare beneficiaries, we used data from a prior study of 750,000 white, black, and Hispanic Medicare enrollees in 2000–2001.
6
Those study subjects had been randomly selected from all traditional (non-Medicare Advantage) beneficiaries who were 65 years of age or older as of January 2000 and alive on January 1, 2001, with oversampling for blacks, Hispanics, and 2001 decedents, to ensured large numbers of blacks and Hispanics. Requiring continuous enrollment during 2000 allowed us to capture patient comorbidities in 2000 (Fig. 1). By design, no subjects were enrolled in HMOs or in Medicare's end stage renal disease program during the selection period, and almost all (99.6%) were enrolled in both Medicare Parts A and B for all 12 months of 2000. For these analyses, we examined the utilization records of those admitted to a hospital in 2001 with a principal or secondary diagnosis of acute coronary syndrome (ACS) in administrative billing records, including all ICD-9-CM codes for acute myocardial infarction (410), intermediate coronary syndrome (4111), or coronary insufficiency (41189) (Supplementary Tables S1 and S2; Supplementary Data are available online at

Data collection timeframe in the 2001 acute coronary syndrome Medicare sample. N=20,604.
We obtained demographic information and data on medical diagnoses and health services utilization from the Centers for Medicare and Medicaid Services (CMS). Patient age, sex, race/ethnicity, state Medicaid buy-in status, and beneficiary zip code of residence were obtained from the Medicare denominator file. Median income for each zip code was obtained from the 2000 National Census, from which we created median income quintiles (coded as 1 through 5, where 5 refers to the 20% of study subjects living in zip codes with the highest median incomes). Revascularization rates were higher for those in higher income quintiles for both white and black, but not Hispanic subjects. Thus, in our model we interacted income quintiles with Hispanic ethnicity.
We used Medicare files in 2001 to capture procedures received using ICD-9-CM diagnosis and procedure codes in the CMS inpatient (hospitalization), outpatient (facility charges other than for hospital inpatient stays), and carrier files (physician Part B services). Using the first ACS hospitalization in 2001 as the “index date,” we categorized patients by the first revascularization procedure they received in 2001 (PCI without stent placement, PCI with stent placement, or coronary artery bypass graft [CABG]). Where two revascularization procedures were present during the same hospitalization, we coded the more invasive one (CABG>PCI with stent>PCI without stent) because the records did not allow us to determine which occurred first.
We used diagnostic codes from Medicare files in 2000 to obtain baseline data on prior comorbidities and procedures (Supplementary Tables S1 and S2). Comorbidity was summarized using the DxCG prospective relative risk score (DxCG version 6.1 for SAS Windows, Verisk Health, Inc.) based on ICD-9-CM diagnoses recorded during the year 2000. 7 The DxCG software is calibrated to associate 1.00 with average expected next-year expenditures among all Medicare beneficiaries observed during a calendar year. We created additional variables to indicate the presence of diagnostic codes for eight comorbid conditions in 2000 that could potentially influence management decisions: diabetes, congestive heart failure (CHF), prior revascularization procedure, peripheral vascular disease, renal failure, stroke, hypertension, and prior acute myocardial infarction (Supplementary Tables S1 and S2).
To adjust for the oversampling of blacks, Hispanics, and decedents, we used analytic weights in all analyses. This allows us to generalize our findings to the larger Medicare population of whites, blacks, and Hispanics from which the study sample was drawn. We report unweighted data to describe our sample and weighted data to refer back to the Medicare population. We calculated weighted rates for all demographic characteristics and prior comorbidities by race/ethnicity and sex and examined 3×6 tables of weighted rates of no revascularization procedure, PCI, or CABG by sex and race/ethnicity groups.
We used logistic regression models to estimate differences in receipt of procedures by race/ethnicity and sex, controlling for demographics and comorbidities. Because coefficients in a logistic regression using a trichotomous outcome are difficult to interpret, we conducted two sets of dichotomous outcomes for our series of logistic regression models. We first predicted receiving any procedure versus none in the whole study population, and then among those who did not receive the most intensive treatment (CABG) we predicted receiving PCI versus no procedure. To understand the distinct contribution of different types of predictors, we fit four models, incrementally including each of the following covariate sets: (1) race/ethnicity and sex only (Model A); (2) age group, the comorbidity score, diabetes, CHF, and any other comorbid conditions that were significant at the p<0.10 level (Model B); and (3) Medicaid status and, where statistically significant, income quintiles with interaction terms for race/ethnicity interacted on Hispanic ethnicity (Model C). In all models we report a variable as statistically significant if the p value was less than 0.05 for the log likelihood test that its coefficient is different from 0, and C-statistics using Stata's f-weights (Stata/SE 9.0 for Windows, StataCorp LP).
The fourth model (Model D) adjusted for geographic location. To control for geographic effects, we mapped zip code of residence into hospital referral regions (HRRs), which are Dartmouth Atlas–based geographic area units 8 defined to reflect health care utilization patterns. The United States is divided into 306 HRRs. To provide a second level of geographic adjustment, we used resident zip code data to indicate the level of urbanicity using Beale codes. 9 However, because we found HRR fixed effects fully accounted for urbanicity, we dropped the Beale indicators from the final analysis and used fixed effects adjustment by HRRs. The fixed effects analysis drops some observations in a few small HRRs.
Data were analyzed using Stata/SE 9.0 for Windows. Approval for this study was obtained from the Division of Privacy Compliance Data Development of the Centers for Medicare and Medicaid Services (CMS), the Boston University Institutional Review Board, and the Federal Drug Administration Research Involving Human Subjects Committee.
Results
We identified 20,604 subjects who were white, black, or Hispanic and admitted with a principal or secondary diagnosis indicating acute coronary syndrome, which extrapolates to approximately 779,000 individuals in the entire Medicare population in 2001. Table 1 provides the weighted and unweighted distributions by race/ethnicity and sex. By design, the unweighted sample contained a greater proportion of blacks and Hispanics than the overall weighted population. Significant racial and ethnic differences included younger age in the black and Hispanic men and women compared with their white counterparts. Rates of receipt of Medicaid were greater for women than men in every racial category, with the greatest rate of Medicaid receipt seen in Hispanics and the lowest rate seen in whites. Rates of diabetes, hypertension, CHF, and renal failure, as well as overall comorbidity burden, were greater in black and Hispanic men and women compared to whites. Women had higher rates of diabetes, CHF, and hypertension than men of the same race/ethnicity.
Unweighted N=20,604. Percentages are weighted for extrapolation to the estimated 779,000 persons in the Medicare population who had an acute coronary syndrome (ACS) event in 2001.
Illness burden is the relative risk from DxCG's prospective risk adjustment score where a score of 1 is the average illness burden in the entire Medicare population. SD, standard deviation; PVD, peripheral vascular disease; CHF, congestive heart failure; AMI, acute myocardial infarction.
Figure 2 presents weighted, unadjusted rates of revascularization by race/ethnicity and sex. White men had the greatest unadjusted rate of any revascularization (PCI with or without stent, or CABG), compared to all other groups. Black women had the lowest unadjusted rate of any revascularization. Within each racial/ethnic group, men were more likely than women to receive PCI and CABG.
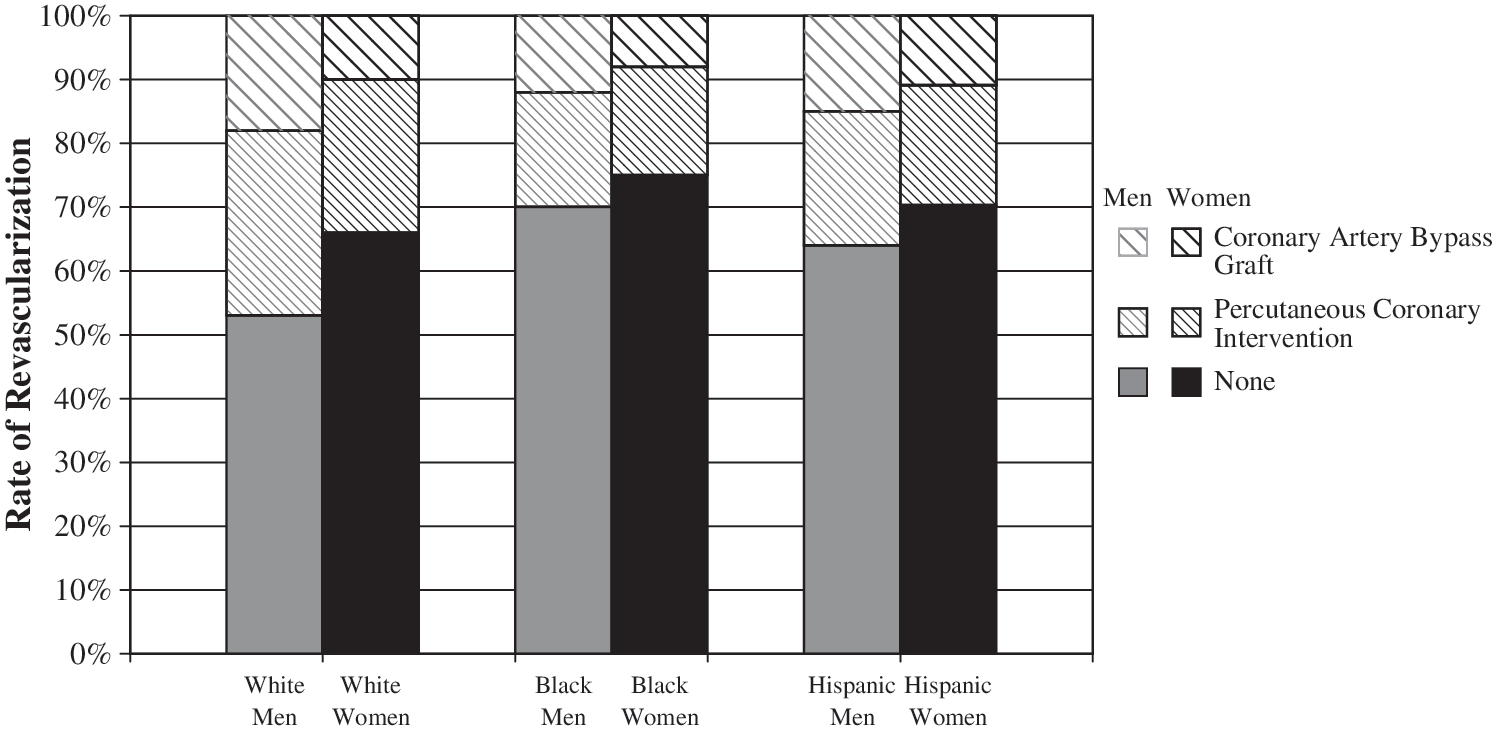
Unadjusted, weighted rates of revascularization procedures in the 2001 acute coronary syndrome medicare sample, by race/ethnicity and sex.
Table 2 shows the effect of modeling to adjust for confounding variables on estimated differences in any revascularization procedure by sex, race, and ethnicity. In the unadjusted Model A, all women, blacks, and Hispanics were seen to be significantly less likely to be revascularized than white men, with odds ratios (ORs) ranging from 0.36 for black women to 0.63 for Hispanic men. Model B adjusted for age and comorbidities, with increased age, higher total comorbidity, and the presence of CHF all significantly reducing the likelihood of revascularization. However, all sex and racial/ethnic differences in revascularization remained large and significant, with ORs ranging from 0.40 for Hispanic women to 0.67 for white women.
Coronary-artery bypass graft and/or percutaneous coronary intervention, with or without stent. Coefficients that are statistically significant at the p=0.05 level are bolded. CI, confidence interval.
All models use logistic regression. Model A is adjusted for ethnicity and sex only; Model B is additionally adjusted for age, total illness burden, diabetes and CHF; Model C is additionally adjusted for Medicaid status and income quintiles interacted with Hispanic ethnicity; Model D is additionally adjusted for geographic location using fixed effects adjustments by hospital referral regions. Additional individual comorbidity variables are not included because they were not significant, even at the p=0.10 level.
Illness burden is a summary measure calculated using DxCG's prospective risk prediction model.
When Medicaid status and income quintile were added to the model (Model C), Medicaid status was a strong predictor of no intervention (OR, 0.56; CI, 0.46–0.68), while income quintile had little or no effect. Adding these variables fully explained the differences between Hispanic men and women and white men, but only explained some of the difference between white women, black men, and black women, compared to white men. For example, the OR for black women shifted from 0.40 (CI, 0.35–0.46) to 0.53 (CI, 0.43–0.62) with Medicaid and income adjustment.
Geographic location did not change the size or statistical significance of any model coefficients, using fixed effects adjustment by HRRs (Model D). In this final model, white women and black women and men remained substantially less likely to receive any revascularization than white men. The c statistic for the final model was 0.79, compared to 0.58 for the unadjusted model.
Table 3 shows the results of modeling to adjust for confounding variables on the racial/ethnic and sex difference in receipt of PCI, excluding from our sample those who received CABG. In the unadjusted model A, all race/ethnicity and sex groups were significantly less likely to receive PCI than white men, with the lowest rates among black men (OR, 0.47; CI, 0.41–0.56) and black women (OR, 0.40; CI, 0.34–0.47). Adjustment for age and comorbidities in Model B once again revealed that increased age, higher total comorbidity, and the presence of CHF all significantly reduced the likelihood of receiving PCI. All racial/ethnic and sex groups maintained significant deficits in comparison to white men in this model. Medicaid status in Model C was strongly associated with no PCI (OR, 0.53; CI, 0.43–0.66). The addition of Medicaid status and income quintile variables accounted for the differences among Hispanic men and women, and white men, and reduced, but did not eliminate, the differences between black men and women and white women, compared to white men.
Population not receiving coronary artery bypass graft surgery during a first ACS admission in 2001 (weighted N ∼674,000). Coefficients that are statistically significant at the p=0.05 level are bolded.
All models use logistic regression. Model A is adjusted for ethnicity and sex only; Model B is additionally adjusted for age, total illness burden, diabetes and CHF; Model C is additionally adjusted for Medicaid status and income quintiles interacted with Hispanic ethnicity; Model D is additionally adjusted for geographic location using fixed effects adjustments by hospital referral regions. Additional individual comorbidity variables are not included because they were not significant, even at the p=0.10 level.
Illness burden is a summary measure calculated using DxCG's prospective risk prediction model.
Discussion
We found racial, ethnic, and sex differences in receipt of all cardiac interventions for Medicare beneficiaries admitted with ACS in 2001. Using a sample from all Medicare beneficiaries with ACS in 2001, we determined that female, Hispanic, and black Medicare beneficiaries received cardiac intervention at lower rates than their white and male counterparts. Removing the individuals who received CABG, we found racial, ethnic, and sex disparities in the receipt of PCI procedures for those admitted with ACS. Our findings contribute two significant additions to this literature. While these disparities have been well described in older datasets, our findings demonstrate that these disparities by sex and race/ ethnicity persist in a more recent cohort. The second addition to the literature by our study, which strategically oversampled the Hispanic Medicare population, is to document disparities within the Hispanic population. We found that previously gender differences within the Hispanic population and racial/ethnic difference between Hispanic and white populations can be accounted for by adjusting for Medicaid receipt.
Our findings are significant in that there were differences seen among and between racial and ethnic groups. The most notable disparities were in black men and women, where the magnitude of the differences was greatest in the unadjusted analyses and the disparities were not corrected with controlling for clinical variables, economic variables, or geographic location. Once other variables were controlled, black men and women had only half the odds of receiving either any cardiac intervention or PCI than white men. Disparities persisted among black men and women, even after controlling for geographic location of care and economic status. This is in contradistinction to the Hispanic population, where we found that including Medicaid and median income in the zip code of residence, as a proxy for economic status, accounted for most of the disparities in revascularization rates. This finding suggests that the disparities in care in the Hispanic population are mediated through economic status, which alone does not account for the differences in the black population. Our findings support a study of nine states for admissions with acute myocardial infarction, in which Cram and colleagues 10 found that disparities in the use in revascularization procedures were greater for black than Hispanic populations, but provided no assessment of the role of gender. We have added to these findings by addressing the gender differences among these populations.
The reasons for the differential findings between Hispanic and black populations warrant further investigation. Given that Medicare eligibility requires 10 quarters of employment with payments into Social Security, the Hispanic population under study may not be representative of younger Hispanic cohorts or of Hispanic populations who do not meet the employment eligibility. Another hypothesis to consider for future work is whether certain patients are perceived as being of a racial or ethnic minority group. Racial and ethnic classification is by self-report in Medicare. However, it is possible that provider or system attribution of race or ethnicity may differ. There are data to suggest that patients of Hispanic descent are misidentified as white, especially if they speak English, 11,12 and that the rate of misclassification of Hispanic persons is greater than that in African Americans. 13 If the mechanism of these disparities is based on the interaction of the individual patient with health-care providers or the health-care system, then differences in minority attribution by the health-care system could account for some of the differences we have found in this study.
Sex differences in revascularization were present in all unadjusted models. However, for Hispanic and black women, differences by sex within race/ethnicity were almost completely accounted for when controlling for clinical factors (Model B) and there were no residual differences once controlling for Medicaid status (Model C).
Our findings concerning sex are consistent with previous studies, which have shown that women who present with AMI are less likely to undergo any coronary interventions, compared with their male counterparts. 4,14,15 This is true in registry studies that were able to control for additional clinical factors, such as ST-elevation and ejection fraction, 4,14 as well as other analyses from administrative data that, like our dataset, do not allow us to control for angiographic and catheterization data. Vaccarino and colleagues 14 revealed that even after adjusting for clinical factors, such as a longer delay between onset of symptoms and initiation of treatment in women, sex disparities in receipt of cardiac interventions persisted. The reasons for sex disparity in receipt of revascularization are not fully understood. Although differences in age and comorbidities between men and women seem to account for part of this discrepancy, adjustment for these factors does not eliminate all sex differences. Sex bias in use of aggressive treatment may also play a role. 16 Our data were collected at a time when aggressive intervention at the time of presentation of any acute coronary syndrome was recommended for women and men, without sex differences in recommendations for care that now exist. 17 More recent data suggest that low-risk women with acute coronary syndromes, including unstable angina and ST and non-ST segment elevation myocardial infarction, may not benefit from early intervention, while an invasive strategy in high-risk men and women results in similar benefit. 18 Therefore, while future analyses might find sex differences based upon guideline recommendations, 19 this was not the case in 2000–2001 within this database.
The work of others has suggested that geographic variation in care can account for most racial and ethnic differences in procedure rates. 20 –22 In contrast to other publications, 23,24 adjustment by geographic location did not account for the persistent disparities seen in the black population. It is possible that the wide dissemination of these procedures, and the interest of medical facilities to offer them due to their favorable reimbursement, accounts for the more recent lack of geographic variability that was seen in the past.
Our study benefits from the broad generalizability to the entire Medicare population. The database did have information on whether individuals had CHF, as well as complete coding data on comorbidities that relate to decision-making around revascularization. 25 However, our administrative database did not include specific clinical information, such as ejection fraction or vessel anatomy, which might be relevant in understanding these differences. The lack of specific anatomic data makes comparisons across sex more difficult, since previous studies have shown that differences in left ventricular function and vessel size, discrete versus diffuse disease, and other anatomic variables make sex comparisons challenging. 26 Furthermore, for patients with ACS, it has been shown that women are more likely than men to have normal coronary arteries. 16 However, no prior research has shown anatomic differences by racial or ethnic group to account for the differences in procedure rates found in this analysis. Our data are limited to a time period before drug-eluting stents were in common usage, and therefore, cannot provide information about disparities in use or outcomes of these stents.
Our data do challenge us to consider the reason for large utilization differences in revascularization by race, ethnicity, and sex. It is of note that the disparities for Hispanic men and women are accounted for by economic variables, while the disparities for black men and women persist even after controlling for these variables. The racial and ethnic differences we identified require further exploration, looking at both patient and physician decision-making, if we are to understand the large and persistent disparities in cardiovascular outcomes in this country by race and ethnicity.
Footnotes
Acknowledgments
This study was supported by the Food and Drug Administration, Office of Women's Health, under contract 223-03-8720.
Disclosure Statement
The authors have no conflicts of interest to report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.