
Abstract
Background:
Much of our understanding of gender differences in chest pain was derived from noncontemporary reports. The aim of the current report was to compare the frequency of chest pain by measures of ischemia in 824 women with suspected myocardial ischemia prospectively enrolled in a clinical trial of exercise testing with electrocardiography (ETT-ECG) alone compared to myocardial perfusion single photon emission computed tomography (SPECT) (ETT-MPS).
Methods:
Women seeking evaluation of chest pain or anginal equivalent symptoms were randomized to ETT-ECG or ETT-MPS with Tc-99m tetrofosmin. The Women's Ischemia Syndrome Evaluation (WISE) and Seattle Angina Questionnaire (SAQ) chest pain and Duke Activity Status Index (DASI) questionnaires were employed in enrolled women. Higher SAQ scores denote improved symptoms or functioning.
Results:
Eight hundred twenty-four women, average age 63 years, at intermediate-high coronary artery disease (CAD) likelihood were enrolled from 43 North American centers. Traditional cardiac risk factors were prevalent, with nearly half of women having a family history of premature coronary disease, hypertension, and hyperlipidemia. Chest pain symptoms occurring at least one to three times per week were reported in 60% of women. An examination of the SAQ domains revealed that although women reported minimal physical limitations (median, interquartile range [IQR] 88, 75–100), there was a greater frequency of stable chest pain symptoms (median, IQR=40, 30–50). The majority of women (79%) reported moderate to heavy physical activity levels at home, with the average ETT and DASI estimated metabolic equivalents (METs) of 8.6±2.6 and 11.5±3.8. Women with more frequent daily episodes of chest pain were more likely to have a lower Duke Treadmill Score (DTS), 1 or mm of ST segment depression, and an abnormal MPS.
Conclusions:
The current report details a contemporary evaluation of female-specific symptomatology and measures of myocardial ischemia. Women reporting frequent angina were more likely to exhibit ischemia and this may characterize a female-specific typical angina pattern.
Introduction
There are nearly 20
Materials and Methods
This multicenter, North American randomized trial enrolled 824 women referred for the evaluation of chest pain or anginal equivalent symptoms at intermediate to high pretest likelihood for CAD, as defined by American College of Cardiology/American Heart Association (ACC/AHA) guidelines for exercise testing. 6 Details of the study were published previously. 12 Women were eligible for trial participation if they met the following criteria: (1) postmenopausal or (2) diabetic women or those with the cardiometabolic syndrome of any age. Women were excluded if they had a prior history of angiographically defined CAD or a prior myocardial infarction (MI). Women were also excluded if they had an abnormal resting electrocardiogram (ECG) (e.g., resting ST-T wave changes) that precluded interpretation of exertional changes. In addition to excluding women not capable of exercising, other exclusion criteria were (1) significant valvular heart disease (i.e., severe aortic stenosis or regurgitation or severe mitral insufficiency), (2) uncontrolled hypertension (blood pressure >210/110 mm Hg) or hypotension (<90/60 mm Hg), (3) history of heart failure or left ventricular ejection fraction <50%, (4) receipt of digoxin therapy, or (5) an inability or unwillingness to complete long-term follow-up or sign informed consent.
Clinical data collection
Comprehensive risk factor data were collected on each patient, including available laboratory measurements of lipids and glucose, body mass index (BMI) (kg/m2), and waist circumference measurements.
Detailed chest pain symptoms were ascertained using the National Institutes of Health–National Heart, Lung, and Blood Institute (NIH-NHLBI)-sponsored Women's Ischemia Syndrome Evaluation (WISE) questionnaire 13 and the Seattle Angina Questionnaire (SAQ). 14 The SAQ is a 19-item questionnaire that quantifies patients' symptoms, function, treatment satisfaction, and quality of life (QOL) measures 14,15 that has been shown to be valid, reliable, and independently prognostic of subsequent cardiac events. 16,17 We also collected self-reported physical functioning using the Duke Activity Status Index (DASI). 18,19 The DASI is a 12-item questionnaire that quantifies patients' activities of daily living (ADL) and recreational time activities. The summed score is estimated peak oxygen consumption. Estimated metabolic equivalents (METs) are derived by dividing peak oxygen consumption estimates by 3.5. The DASI has been shown to be valid, reliable, and independently prognostic of cardiac events in women. 18,19 Finally, women were queried as to their overall rating of life satisfaction and QOL.
Exercise testing protocols
All exercise stress testing was performed in accordance with the most recent ACC/AHA guidelines; an exercise ECG was considered abnormal as defined by these ACC/AHA guidelines. 20 Women exercised according to the Bruce protocol until volitional fatigue or at the occurrence of significant ST segment depression or worsening chest pain symptoms. Heart rate, blood pressure, symptoms, and ECG measurements were reviewed throughout testing and for 5 minutes into recovery.
SPECT image acquisition
Imaging for the gated myocardial perfusion single photon emission computed tomography (SPECT) study began 15–60 minutes after administration of the radiopharmaceutical, Tc-99m tetrofosmin. SPECT images were obtained in the usual manner for each laboratory in accordance with the imaging guidelines of the American Society of Nuclear Cardiology. 21 SPECT images were interpreted to be normal for a summed stress score <4 or abnormal for a summed stress score of ≥4.
Statistical analysis
Comparison of categorical differences by randomization status was performed with a chi-square test using the linear association or likelihood ratio statistic where appropriate. A comparison of continuous measures, such as age, by randomization status was performed using a t statistic. SAQ subscale scores for physical limitations, chest pain stability, chest pain frequency, treatment satisfaction, and QOL were compared using nonparametric statistics (Wilcoxon rank sum test or chi-square statistic) because of nonlinearity. Median and interquartile range (IQR) scores for each of the SAQ subscales were plotted. A cumulative frequency distribution of exercise and DASI METs was plotted. Average and 95% confidence interval (CI) Duke Treadmill Scores (DTS) within angina frequency subsets of women were calculated using analysis of variance (ANOVA) statistics. Additional comparison of angina frequency subsets by the frequency of significant ECG changes (i.e., ≥1 mm of ST depression) or high-risk DTS were compared using chi-square statistics. Spearman's rho correlations were used to correlate SAQ subscales with angina frequency.
Results
Clinical characteristics
Women enrolled in this trial were on average 63 years of age, with the majority being postmenopausal (Table 1). Traditional cardiac risk factors were prevalent, with nearly half of the women being hypertensive or hyperlipidemic, having the cardiometabolic syndrome, and with a family history of premature coronary heart disease. Nearly 1 in 5 women were diabetic. Comorbid conditions were also notable, with approximately one third of women being obese or having had a prior diagnosis of esophageal reflux. A history of migraine headaches was present in 18% of women.
Age and body mass index are presented as median and interquartile range measurements.
ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker; CAD, coronary artery disease; GI, gastrointestinal; HDL-C, high-density lipoprotein cholesterol; PCOS, polycystic ovary syndrome.
Chest pain quality and characteristics
Angina or dyspnea was reported in all women (Table 2). Stress was noted as a provocative stimulus for pain in the majority of subjects (∼69%). Of note, >70% of women noted resolution of chest pain with rest, as traditionally used to define typical angina pectoris. Sixty percent of women reported frequent episodes of chest pain that occurred at least one to three times per week and that the symptoms were increasing in frequency before testing (Table 3). As a result, women frequently noted that their symptoms often precipitated life dissatisfaction (∼36% of women).
Comparison is by chi-square likelihood ratio statistic, with the exception that chest pain frequency=chi-square linear-by-linear association statistic. Time to relief with rest comparison using analysis of variance statistic; comparison using nonparametric statistic did not change the result; all p>0.20.
SPECT, single photon emission computed tomography.
Comparison by chi-square likelihood ratio statistic; all p>0.20.
Health status and QOL measures
Despite this symptom burden, women often reported their QOL as good/very good (74%), with only 11% noting a fair poor rating (Table 4). Additionally, women frequently reported engaging in moderate to heavy physical activity at home (79%) and during their leisure time (65%) (Table 5).
Comparison by chi-square linear-by-linear association statistic; all p>0.20.
Comparison by chi-square likelihood ratio statistic; all p>0.20.
Figure 1 plots the cumulative frequency of estimated METs by the DASI and exercise test. Importantly, the DASI noted a greater frequency of women with higher estimated METs. On the DASI, nearly half of the women reported physical functioning up to 12 METs. Within the DASI, women reported some difficulty in running even a short distance (34.1%), doing heavy work around the house, such as scrubbing floors (31.1%), and participating in strenuous sports (36.9%), yet many noted no difficulties in performing moderate work around the house (96.9%) or in participating in recreational activities, such as golf or bowling (82%).
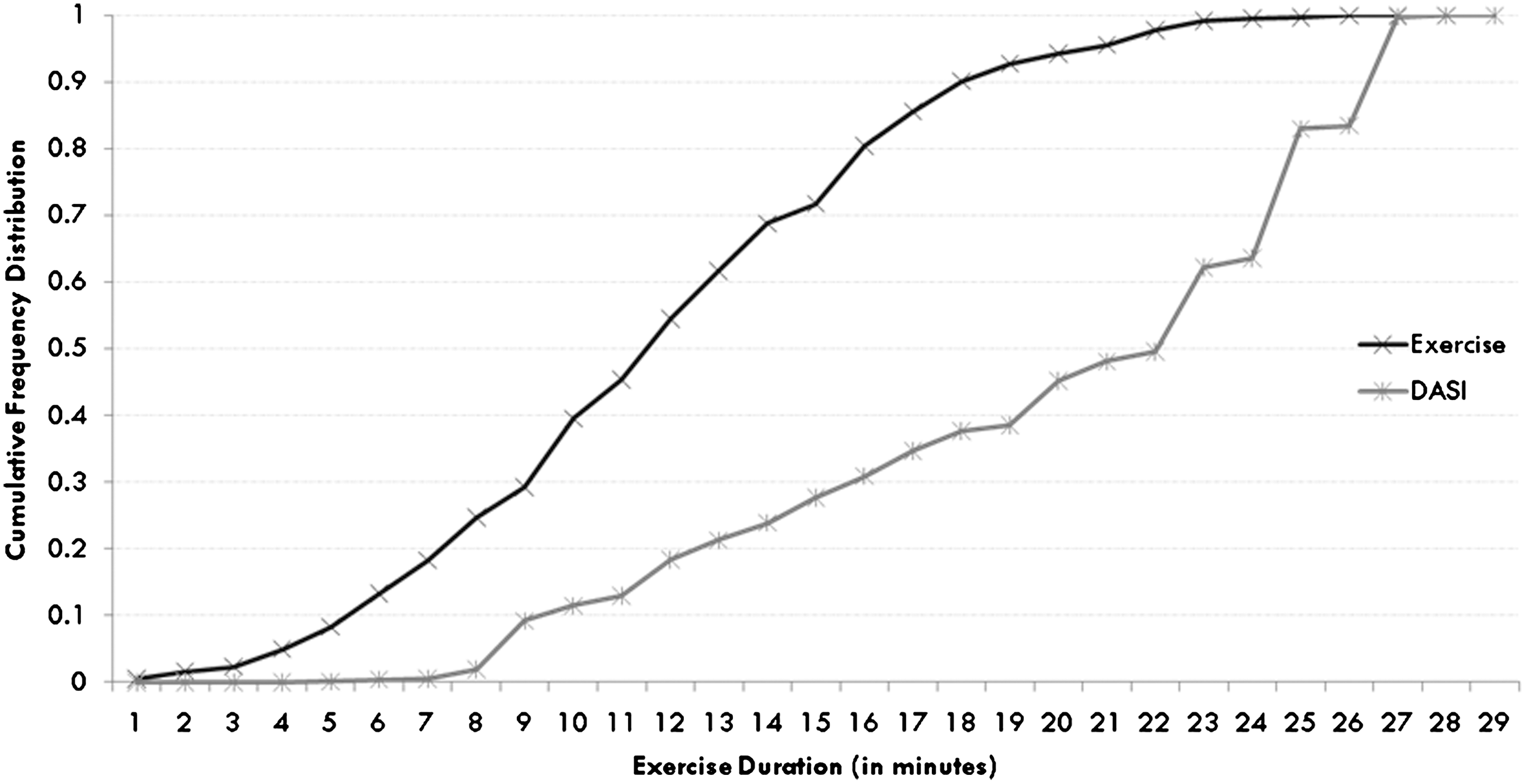
Cumulative frequency distribution of estimated Duke Activity Status Index (DASI) for the determination of metabolic equivalents (METs).
SAQ subscales
Median and IQR scores for the SAQ subscales are reported in Figure 2. Women reported a high physical functioning (median score=88) and stable chest pain symptoms (median score=75), denoting very good functioning and stability.
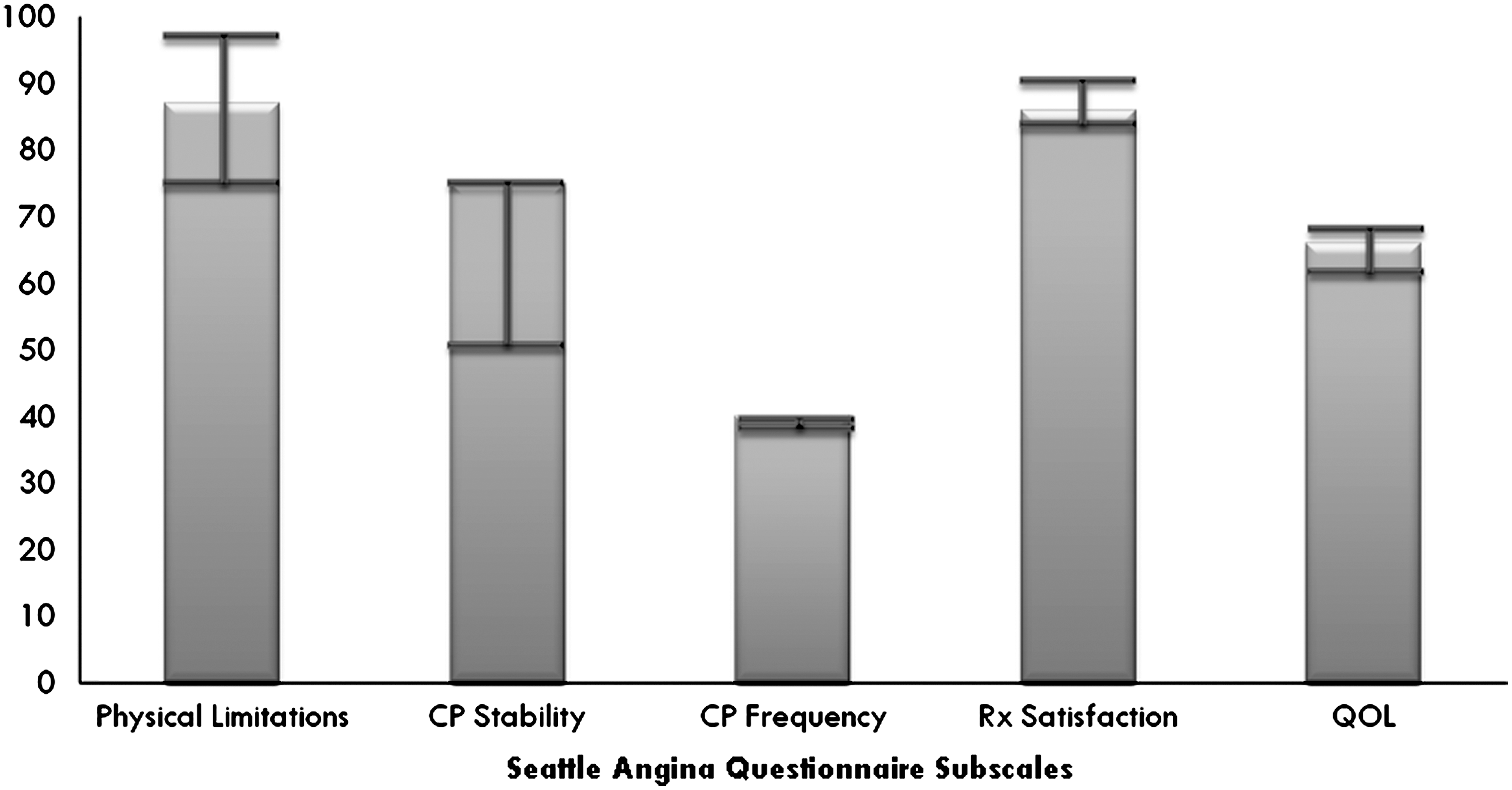
Comparison of median and interquartile range scores on subscales of the Seattle Angina Questionnaire by randomized testing strategy (exercise electrography vs. exercise myocardial perfusion imaging). Rx=Treatment; A higher score indicates better physical functioning or quality of life (QOL) or lower angina (CP) burden/stability. Rx, treatment. Two independent sample nonparametric Mann-Whitney U tests: Physical Limitations, p=0.30; CP Stability, p=0.57; CP Frequency, p=0.69; Rx Satisfaction, p=0.36; QOL, p=0.93.
Exercise Treadmill Testing (ETT) results
Women exercised to an average of 8.6±2.6 METs. Nearly 45% of women exercised beyond 9 METs, with only 10% of women being incapable of performing >5 METs of exercise (Fig. 1). During exercise testing, 17.8% of women reported chest pain.
Correlative results between chest pain and test results
Examining the relationship between chest pain frequency and abnormal ETT or MPS findings reveals an interesting pattern of results (Fig. 3). Women with more frequent daily episodes of chest pain were more likely to have a lower DTS, ≥1 mm of ST segment depression, and an abnormal MPS. Similar results were noted when comparing the SAQ angina frequency subscale to test abnormalities. In fact, all the women with an abnormal MPS had an angina frequency score of ≤60. Similarly, 96.3% and 84.6% of women with significant ST segment depression and a high-risk DTS had an SAQ score in the angina frequency domain ≤60.

Average Duke Treadmill Score (DTS) with 95% confidence intervals, by angina frequency. The frequency of a high-risk DTS, abnormal ST segment depression (≥1 mm), and abnormal myocardial perfusion SPECT (MPS) is also reported.
There was a modest correlation between the SAQ physical limitations subscale and angina frequency (Spearman's rho=0.33, p<0.0001), suggesting a trend toward women with frequent symptoms having lower levels of physical functioning. Further analysis revealed that women having chest pain at least three times per week more often had reduced physical functioning, defined as ≤7.4 DASI METs (26.3% vs. 17.8% for those with pain less often, p=0.025). Of the DASI questions, women with frequent chest pain more often could not perform heavy household work (p=0.002) or participate in moderate/strenuous recreational activities (p>0.064). It should be noted that with this relationship, although exhibiting a trend, all women had preserved physical work capacity; that is, for those with chest pain at least three times per week, average DASI and ETT METs were 11.1±3.8 and 8.5±2.7 compared to 11.7±3.7 and 8.8±2.6 (p=0.029 and p=0.163). With regards to other factors, the frequency of an increase in diastolic BP of 10 mmHg or higher occurred in approximately 25-40% of women but was similar by chest pain frequency (p=0.32).
Discussion
In this multicenter, prospective trial, a detailed description of clinical signs and symptoms of suspected CAD provides insight into the contemporary pattern of female-specific symptomatology. This evidence is important because of the paucity of data from high-quality clinical trials on a woman's symptom burden and its relationship to objective evidence of myocardial ischemia. Our results show that women at intermediate to high pretest CAD risk with an average risk factor burden generally have durability in both physical functioning (median DASI≈12 METs) and QOL, perhaps as a result of requirements for their routine daily activities. This high level of functioning was confirmed by exercise testing, where half of women were able to perform ≥8 METs of exercise. Despite high physical functioning, women reporting more frequent chest pain symptoms had prevalent ischemia. In fact, nearly half of the women with frequent daily symptoms had ECG changes during exercise testing, with a prevalent high-risk DTS or abnormal MPS.
For many decades, it has been known that women report a greater frequency of nonspecific or atypical chest pain symptoms. 3,22 However, our success in differentiating other female-specific patterns for chest pain symptoms has been poor. Emerging data reveal that our understanding of risk in symptomatic women, regardless of the typicality of pain, now appears at the precipice of unfolding an emerging gender-specific pattern. One key factor is that the mere presence of symptoms should not be considered benign. Recent data from the NIH-NHLBI-sponsored WISE confirmed that women with symptoms in the setting of nonobstructive CAD have an elevated risk of major cardiovascular events. 8,23,24 Also, recent data from the Women's Health Initiative (WHI) show that women with nonspecific chest pain have a 2-fold higher risk of incident MI. 9 These recent data indicate that the mere presence of symptoms indicates an elevated risk in women. Our data extend these findings, noting that more frequent symptoms may be an additional parameter in defining a female-specific typical angina pattern. These data require validation in larger female cohorts but suggest that ischemia is more prevalent in women with a greater symptom burden.
It is important to relate our findings of a symptom pattern within the context of the high level of physical functioning in these women. This piece of evidence is crucial to understanding their level of risk and may explain the less intensive management of women. Adequate physical functioning beyond the requirements of ADL signifies good health status and portends a reasonable clinical outcome; at least in the near term. 24 –26 Thus, it may be more precise to note that ischemia in the setting of a frequent symptom burden and adequate physical functioning places a woman at elevated risk, requiring additional evaluation. Moreover, it may be that household chores require women to perform higher levels of tasks despite their burden of chest pain. It may also be possible that household activities and their associated metabolic requirements may not provoke symptoms at the same threshold as that achieved during exercise testing or that of their male counterparts. This discordance between a symptom burden and physical capacity may also reflect a woman's role functioning that differs from that of a man.
Our findings reveal a relationship between the frequency of chest pain symptoms and evidence of ischemia either by ECG or MPS. In patients reporting four or more episodes per day of angina, 11.1% had a high risk DTS, and 14.6% had an abnormal MPS, a rate 5–8-fold higher than that for women noting a minimal burden of symptoms. The greater frequency of symptoms may be a harbinger of underlying endothelial dysfunction and microvascular disease, both of which have been implicated as more important components of coronary disease risk in women than men. 24,27 –29 Moreover, the greater frequency of angina symptoms may more closely correlate to alterations in vascular tone that fluctuate throughout the day. Combine vascular dysfunction as a precipitator with the lower pain threshold noted in women, the current results provide a framework for understanding female-specific differences in chest pain. 29 This is supported by reports linking evidence of vascular dysfunction with worsening clinical outcomes in women. 30,31 It is important for women of all ages, such as those enrolled in the current trial, that chest pain symptoms coupled with evidence of ischemia are associated with a higher coronary standardized mortality ratio. 10 Thus, our findings appear to be coalescing a greater understanding of pain symptoms in women yet require more focused research to fully elucidate a meaningful pattern of symptoms that may be applied in daily clinical practice.
Another factor worth noting is that confirmatory evidence of ischemia, should it be linked to vascular dysfunction, is associated with an underlying burden of coronary atherosclerosis. This provides a focused path forward for targeted treatments and symptom control. This report is part of unfolding female-specific research that aims to provide a positive platform on which to guide clinical decision making in order to circumvent the frequently reported underuse of guideline-indicated care in women. 32 –38 In one recent report, a failure to refer women with signs and symptoms of myocardial ischemia, similar to that in the WOMEN trial, for coronary angiography was associated with a nearly 3-fold higher risk of major coronary disease events, 11 suggesting that undetected risk remains in our female patients.
Study limitations
The inclusion of prognostic data may have altered our findings, including the relationship among chest pain symptoms, ischemia, and outcome. Women were generally of above average exercise abilities and enrolled in a clinical trial. Although all women were clinically referred for evaluation of suspected myocardial ischemia, the appropriateness of this referral decision was not evaluated as part of this trial and, thus, represents a selected intermediate risk group. The current results cannot be extrapolated to the acute chest pain setting. The potential for recall bias to influence the current results should be considered. This study enrollment is completed, and the outcome data being analyzed will add to our interpretation of ischemic findings in at-risk women. This analysis was not the primary aim of this trial but was a prespecified (exploratory) secondary analysis. It was not powered because of our limited a priori understanding of the relationship between symptom frequency and ischemic risk in women. The use of MPS requires exposure to ionizing radiation and should be applied only where the benefit of information gained exceeds the risk. Other, as yet, defined symptom characteristics may provide more information as to CAD risk in women. Importantly, we applied the DASI and exercise test estimates of METs. Estimates of functional capacity may vary from observed maximal oxygen consumption measurements. Estimates of METs by means of the Bruce protocol overestimate observed peak oxygen consumption measurements.
Conclusions
Of women enrolled in the WOMEN trial, those with chest pain benefit from a more detailed evaluation of their symptom burden. Despite a woman's level of physical functioning, the presence of frequent chest pain signifies an elevated ischemic risk. This evidence is important because of the paucity of data from prospective clinical trials about a woman's symptom burden and its relationship to provocative ischemia. Nearly half of the women with frequent daily symptoms had ECG changes during ETT, with a 5–8-fold greater frequency of a high-risk DTS or abnormal MPS. These preliminary findings require validation in a larger cohort of women yet support further exploration on female-specific research targeted to our understanding of the role of symptoms, ischemia, and CAD risk in women.
Footnotes
Acknowledgments
An unrestricted grant for this investigator-initiated trial was provided by GE Healthcare, Princeton, New Jersey.
Disclosure Statement
The authors have no conflicts of interest to report.