
Abstract
Background:
The impact of high blood pressure (BP) on target organs (TO) in premenopausal women is not well known. The purpose of this study was to describe gender differences in TO involvement in a cohort of young-to-middle-aged subjects screened for stage 1 hypertension and followed for 8.2 years.
Methods:
Participants were 175 women and 451 men with similar age (range 18–45 years). Ambulatory BP at entry was 127.5±12.5/83.7±7.2 mm Hg in women and 131.9±10.3/81.0±7.9 mm Hg in men. Ambulatory BP, albumin excretion rate (AER), and echocardiographic data (n=489) were obtained at entry, every 5 years, and before starting antihypertensive treatment.
Results:
Female gender was an independent predictor of final AER (p=0.01) and left ventricular mass index (LVMI) (p<0.001). At follow-up end, both microalbuminuria (13.7% vs. 6.2%, p=0.002) and left ventricular hypertrophy (LVH) (26.4% vs. 8.8%, p<0.0001) were more common among women than men. In a multivariable Cox analysis, after adjusting for age, lifestyle factors, body mass, ambulatory BP, heart rate, and parental hypertension, female gender was a significant predictor of time to development of microalbuminuria (p=0.002), with a hazard ratio (HR) of 3.06, (95% confidence interval [CI] 1.48-6.34) and of LVH (p=0.004), with an HR of 2.50 (1.33-4.70). Inclusion of systolic and diastolic BP changes over time in the models only marginally affected these associations, with HRs of 3.13 (1.50-6.55) and 3.43 (1.75-6.70), respectively.
Conclusions:
These data indicate that premenopausal women have an increased risk of hypertensive TO damage (TOD) and raise the question about whether early antihypertensive treatment should be considered in these patients.
Introduction
Gender differences in blood pressure (BP) are detectable during adolescence and persist through adulthood. 1,2 In all ethnic groups, young men tend to have higher mean systolic and diastolic BP than age-matched women (by 6–7 and 3–5 mm Hg, respectively), and through middle age, the prevalence of hypertension is higher among men than among women. 1 Recent studies using the technique of 24-hour ambulatory BP monitoring have confirmed that BP is higher in men than in women at similar ages. 3 The higher rate of hypertension may explain why men are generally at greater risk for cardiovascular and renal disease than are age-matched, premenopausal women, a difference that tends to attenuate at older ages. 4,5 It is not known, however, if the gender-related difference in risk persists for the same level of BP in this age range. Compared to normotensive controls, BP is proportionally higher in stage 1 hypertensive premenopausal women than in age-matched men and could, thus, have a greater impact on target organs. Microalbuminuria represents an important marker of end-organ damage in hypertension and is an independent risk factor for morbidity and mortality. 6,7 Left ventricular hypertrophy (LVH), detected by either electrocardiography (ECG) or echocardiography, is a well-recognized risk factor for myocardial infarction (MI), cardiac sudden death, congestive heart failure (CHF), and stroke. 8,9 Hypertensive subjects with left ventricular mass (LVM) in the upper normal range already have increased risk for cardiovascular events. 10 Because cardiovascular disease (CVD) is the leading cause of death in women, 11,12 there is a need to improve our understanding of the factors that influence development of hypertensive complications in women with hypertension. In view of the lack of data in published reports, we examined the development of microalbuminuria and LVH in a cohort of young-to-middle aged subjects initially screened for stage 1 hypertension. We hypothesized that in this age range, albumin excretion rate, (AER) and LVM would increase faster in women than in men with similar BP levels.
Materials and Methods
Study subjects
The present analysis was carried out in 626 white subjects taking part in the Hypertension and Ambulatory Recording VEnetia STudy (HARVEST) who had urinary albumin and 24-hour ambulatory BP monitoring data at baseline and at the end of the follow-up. 13,14 Subjects with baseline diastolic clinic BP between 90 and 99 mm Hg or systolic BP between 140 and 159 mm Hg or both were enrolled. None of the subjects had received antihypertensive treatment before the study. Patients with diabetes mellitus, nephropathy, and CVD were excluded. Consecutive patients with the noted clinical characteristics seen in the offices of the general practitioners and willing to participate in the study were eligible for recruitment and were sent to 17 referral centers in northeast Italy. The higher prevalence of men among our study participants (72%) confirms previous observations of a much higher prevalence of men in the young segment of the hypertensive population. 15
Patients files, ECG and echocardiographic tracings, and blood and urine samples were periodically collected by five monitors and taken to the coordinating office in Padova, where they were processed. At baseline, all subjects underwent physical examination, anthropometry, blood and urine sampling, office BP and 24-hour BP measurements, ECG, echocardiography, and 24-hour urinary albumin measurement. Body mass index (BMI) was used as an index of obesity (kg/m2). The data included a medical and family history and a questionnaire of current use of alcoholic beverages and tobacco and physical activity habits. 13 Clinic BP of the participants at baseline was compared with that of 281 normotensive control subjects of similar age and sex distribution (67% men). The normotensive subjects were recruited from the hospital staff and their relatives; all were asymptomatic and normal at physical examination. Standard ECG, blood chemistry, and urinalysis were normal in all subjects.
The study was approved by the Ethics Committee of the University of Padova, and written informed consent was given by the participants. The procedures followed were in accordance with institutional guidelines.
BP measurement
The mean of six readings taken in the supine position during two separate visits was defined as baseline clinic BP.
14
Twenty-four hour BP monitoring was performed with A&D TM2420 model 7 (A&D Co., Tokyo, Japan) or ICR Spacelabs 90207 monitor (Spacelabs Inc., Redmond, WA). Both devices were previously validated.
14
Measurements were taken every 10 minutes during the day (6
Twenty-four hour urine collection
During the 24-hour recordings, urine was collected for AER measurement. Immediately after completion, volumes were measured, and urine specimens were frozen (−20°C) and sent to the coordinating office in Padova. 16 The urinary albumin level was measured using a commercially available radioimmunoassay (RIA) kit (H ALB kit-double antibody, Sclavo SpA, Cinisello Balsamo, Italy). Results were expressed as mg/24 h and were transformed logarithmically to correct for skewing in distribution. Microalbuminuria was defined as an AER rate ≥30 mg/24 h. Microalbuminuria detected in two consecutive measurements was used as the outcome variable.
Echocardiography
Echocardiography at baseline and at the end of the study was obtained in 573 of the 626 subjects in eight hospital echocardiography laboratories. All sonographers followed the same protocol, which was devised by the study coordinator (PP) and was illustrated during ad-hoc meetings. In 489 participants, M-mode images were technically satisfactory and were used for analysis. All measurements were made blind by two observers according to the American Society of Echocardiography at the coordinating center at the University of Padova laboratory following previously published procedures. 16 All linear echocardiographic data were indexed by height, and LVM was indexed by height (LVMI) to the allometric power of 2.7. 17 LVH was defined as a LVM≥50 g/m 2.7 in men and ≥47 g/m 2.7 in women. In Cox regression analyses, the LVM≥51 g/m 2.7 partition value for both genders also was tested. 17 Relative wall thickness was defined as the ratio of wall thickness/end-diameter in diastole. Data on the reproducibility of echocardiographic measurements in our sample have been reported previously. 18
Follow-up
After baseline examination, follow-up visits were scheduled at 1, 2, and 3 months, 13,14,16 and thereafter every 6 months. Ambulatory BP monitoring was performed at baseline and at 3 months, 5 years, 10 years, or just before starting antihypertensive treatment in patients who needed antihypertensive treatment. Patients dropped out of the study if they developed sustained hypertension needing antihypertensive medication, in accordance with current guidelines. 13,14,16 At this point, they received a final 24-hour BP measurement and target organ (TO) assessment before starting therapy. In the patients who remained untreated, the last available BP monitoring, urinary albumin measurement, and echocardiographic data were used to calculate final ambulatory BP, AER, and echocardiographic parameters, respectively. Median follow-up for the 626 participants was 8.2 years (interquartile range [IQR] 5.0–11.1 years). For patients lost to follow-up, data available at the date of latest contact were used. Other details on follow-up procedures were reported elsewhere. 13,14,16
Data analysis
Data are presented as mean±standard deviation (SD) unless otherwise specified. To compare the hypertensive participants with the normotensive control subjects, a general linear model was used, using BP as the dependent variable and BP group (normotensive or hypertensive), gender, age, and BMI as independent variables. The key variable in this model was the group-by-gender interaction (Fig. 1). Within the normotensive and hypertensive groups, between-sex differences were assessed with the t test for the variables normally distributed. Data were adjusted for age by the use of linear regression analysis. Follow-up changes in clinical variables were evaluated using a general linear model, with the value for the measurement of interest serving as the dependent variable and gender, age, time to final assessment, and baseline data serving as independent variables. Nonnormally distributed data, presented as median and IQR, were analyzed using the Mann-Whitney test. The significance of differences in categorical variables was assessed with the chi-square test. To explore the predictors of evolution of AER and LVMI, multivariable linear regression analyses were performed, with final AER or LVMI as the dependent variable and risk factors measured at baseline or their changes from baseline to study end as the independent variables. Multivariable time-dependent Cox proportional hazards analyses were used to regress time until development of microalbuminuria or LVH against gender. Other variables included in the models were sex, age, BMI, ambulatory systolic and diastolic BP, ambulatory heart rate, parental hypertension, smoking status, alcohol consumption, physical activity, changes in ambulatory BP over time, and baseline AER or baseline LVMI. A 2-tailed probability value <0.05 was considered significant. All analyses were performed using Statistica version 6 (Stat Soft, Inc, Tulsa, OK) and Systat versions 10 and 11 (SPSS Inc., Evanston, IL).
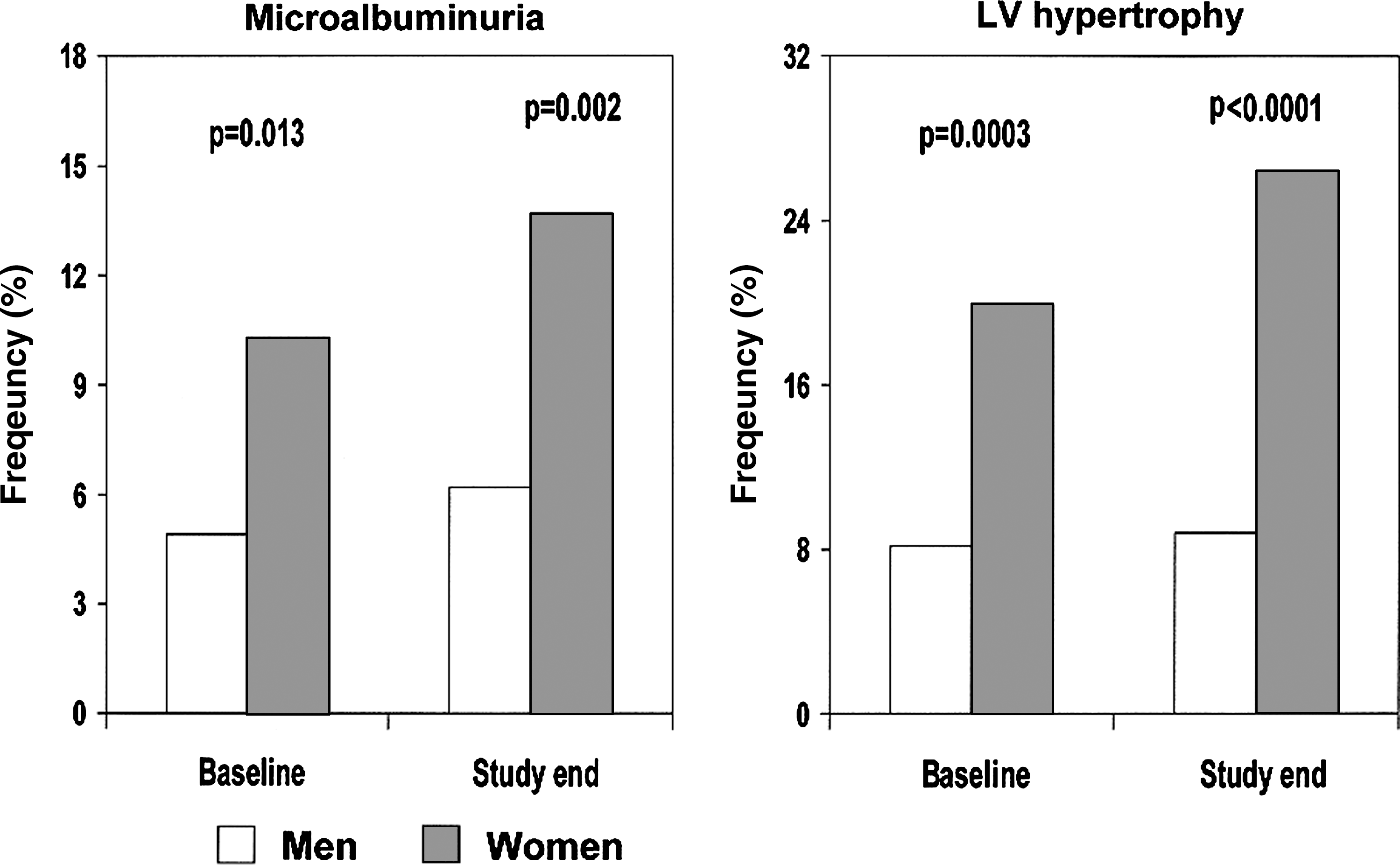
Sex-specific prevalence of microalbuminuria (n=626) and of left ventricular (LV) hypertrophy (n=489) at baseline and after 8.2 years of observation in a population of subjects screened for stage 1 hypertension. Microalbuminuria was defined as an albumin excretion rate ≥30 mg/24 h in two consecutive measurements, and LV hypertrophy as an LV mass ≥50g/m2.7 in men and ≥47g/m2.7 in women.
Results
Among the normotensive subjects, mean±SD systolic BP (124.0±10.5 vs. 118.1±9.8 mm Hg, p<0.001) and diastolic BP (75.8±8.4 vs. 72.1±7.1 mm Hg, p<0.001) were higher in men than in women. In a general linear model, a significant interaction was found between gender and BP status on the BP level for both systolic BP (BP group, p<0.001; sex, p<0.001; group×sex interaction, p<0.001) and diastolic BP (BP group, p<0.001; sex, p=0.005; group×sex interaction, p<0.001). Among the hypertensive participants, women were older and had a lower BMI than men (Table 1). Their clinic and ambulatory systolic BPs were lower than those in men, whereas clinic and ambulatory diastolic BPs were higher. As a result, ambulatory mean BP was almost identical in the two groups, and ambulatory pulse pressure was lower in women than in men. Women were less likely to drink alcohol or to be physically active than men, whereas the percent of smokers did not differ between genders (Table 1). Plasma glucose, high-density lipoprotein cholesterol (HDL-C), and triglyceride concentrations were significantly lower in women compared with men at both baseline and study end (all p<0.01), whereas total cholesterol did not differ between genders (p>0.42) (data not shown). In the subset of 489 subjects with valid echocardiographic data, similar characteristics to those of the whole group were found. In particular, the percent of women was 28.6% (p=nonsignificant vs. rest of group). In addition, age, BMI, clinic and ambulatory BPs and heart rates, and lifestyle factors did not differ significantly from the rest of the population (data not shown).
Unless otherwise indicated, data are expressed as mean (standard deviation [SD]) or percent.
Unadjusted.
p value for log-transformed data.
Median (interquartile range).
Adjusted also for baseline value.
p value from Mann-Whitney U-test.
AER, albumin excretion rate; BMI, body mass index; BP, blood pressure; bpm, beats/minute.
Follow-up changes in BP in participants
In both genders, there was a substantial decline in clinic systolic and diastolic BP during the first 6 months of observation, without significant differences between the groups (Table 1). During a median follow-up of 8.2 years, 61.0% of men and 63.4% of women developed hypertension, needing antihypertensive treatment according to current guidelines (p not significant). After adjustment for age and baseline BP value, 24-hour systolic BP increased to a similar degree in men and women, whereas 24-hour diastolic BP increased more in men.
Microalbuminuria in participants
Age-adjusted AER was higher in women than in men at baseline (Table 2), and the between-gender difference remained significant during follow-up. In multivariable linear regression, female gender was a significant predictor of log-AER at the end of the study (Table 2). This association was attenuated when baseline AER was accounted for in the model (p=0.057). Microalbuminuria was more common in women than in men at both baseline and study end (Fig. 1). In a multivariable Cox regression model, female gender was a significant predictor of final microalbuminuria (Table 3). This association did not change when follow-up changes in 24-hour BP were incorporated in the model and was no longer significant when baseline AER also was included.
Data from multiple regression analyses in which albumin excretion rate or left ventricular mass index was the dependent variable.
SBP, systolic blood pressure; CI, confidence interval; DBP, diastolic blood pressure; HR, hazard ratio; HT, hypertension; LVM, left ventricular mass; LVMI, left ventricular mass index; SBP, systolic blood pressure.
Echocardiographic data in participants
At baseline, LV dimensional parameters did not differ between genders (Table 4). During follow-up, there was a greater increase in interventricular septum thickness, LV posterior wall thickness, LV end-diastolic diameter, and LVMI among the women than the men, and at study end, LV wall thickness and LVMI were greater among the women than the men (Table 4). In a multivariable linear regression, female gender was a significant predictor of LVMI at the end of the study (Table 2). This association remained robust on additional adjustment for baseline LVMI (p=0.009). LVH was more common in women than in men both at baseline and at study end (Fig. 1). In a multivariable Cox model, female gender was a significant predictor of final LVH also when follow-up changes in 24-hour BP were incorporated in the model (Table 3), and this association remained highly significant when baseline LVMI was also included. The association of female gender with LVH development was statistically significant for both the sex-specific and the gender-independent definition of LVH (Table 3).
Data are given as mean (SD).
p values are adjusted for age.
p≤0.01 and c p<0.05 vs. follow-up changes in men adjusted for age, time, and baseline value.
IVSd, interventricular septum thickness in diastole; LVDD, left ventricular end-diastolic diameter; PWd, left ventricular posterior wall thickness in diastole; RWT, relative wall thickness.
Discussion
Our results show that premenopausal women are at increased risk of developing hypertensive TO damage (TOD) compared with hypertensive men of similar age. Both microalbuminuria and LVH were more common in our women participants already at baseline, and the between-gender differences increased after 8 years. The associations found in this investigation were obtained from a randomly selected nondiabetic population of subjects screened for stage 1 hypertension who were largely asymptomatic for clinical manifestations of CVD. To our knowledge, this is the first long-term prospective study to evaluate the association between gender and development of hypertensive complications in untreated young-to-middle-aged subjects. The risk of developing CVD is considerably less in premenopausal women than in age-matched men. 4,5 Among normotensive women <45 years of age, the prevalence of CVD is one third lower than in men of the same age, 19 and coronary artery disease is delayed by approximately 10–15 years. 20 It is not known, however, if this is due to the lower BP among women in this age range.
Gender differences in BP
After the onset of puberty, boys have higher BP than do age-matched girls, 1,2 a difference that persists into adulthood until menopause. 21 In 352 Danish men and women, Wiinber et al. 3 showed that 24-hour ambulatory mean BP is lower in premenopausal women than in men at similar ages by approximately 6–10 mm Hg. Findings were similar in a meta-analysis performed by Staessen et al. 22 The mechanisms underlying this gender difference in BP are unclear. It has been suggested that the Y chromosome 23 and gonadal hormones 24,25 are contributing factors. The present results confirm that BP is lower in normotensive premenopausal women than in men of similar age and that hypertension is less frequent in females. As a result of screening, women with BP in the stage 1 hypertension range comprised 30% of our sample, although they were 3 years older than the men.
Gender differences in hypertensive TOD
The pathogenetic mechanisms leading to a greater rate of hypertensive complications in premenopausal women than age-matched men are unclear. Hypertension in premenopausal women might be associated with a poorer cardiovascular risk profile. In the present study, however, women were less likely to smoke or drink alcohol, were leaner, and had a more favorable metabolic profile than men. In addition, among the women, BP did not have a worse time course, and the follow-up increase in BMI was even smaller. Although a biologic mechanism is not readily apparent, the gender difference in the association of hypertension with severity of TOD found in the present study may be due to a proportionally greater hemodynamic load imposed on the heart and the kidney in young-to-middle-aged women compared to men. As mentioned, in the general population, BP is much lower in premenopausal women than in age-matched men; thus, a BP in the hypertensive range may have a more deleterious impact in women. In the present study, the BP difference between the hypertensive and the normotensive women was greater than that seen in men (27.8/23.2 mm Hg vs. 23.1/17.9 mm Hg), with a highly significant group×sex interaction. However, we cannot exclude that other mechanisms are also operative. In a study by Wallen et al. 26 performed in rats, females showed a larger cardiac mass adjusted for body weight than did males in both normotensive and hypertensive rats. In that study, for any given diastolic BP, females had a greater heart weight/body weight ratio than males. This relationship was influenced by the presence of sex steroids because in the absence of estrogen (neutered females), the heart weight/body weight ratio was lower, and this was restored to intact levels in neutered females that received estrogens. As sex is a strong correlate of LVM, identification of appropriate upper normal limits for LVM must account for the effect of sex. Although different cutoff levels are used for men and women to identify subjects with LVH, the use of the 50 g/m2.7 cutoff in men and the 47 g/m2.7 cutoff in women has recently been criticized. 27 According to some authors, an LVM≥51 g/m2.7 partition value for both genders represents a more appropriate definition of LVH. 17,28 For this reason, in the present study, we used both sex-specific and gender-independent partition values that have been prognostically validated in the current literature as obtaining consistent results.
Little is known of gender-related differences in development of microalbuminuria in young-to-middle-aged subjects with hypertension. In some cross-sectional studies, microalbuminuria has been reported to be more common in hypertensive men than women, 29,30 whereas in other studies, no gender-related differences in microalbuminuria were reported. 31,32 However, the results of those studies were obtained from populations of older subjects, and little or no information is available on the longitudinal association of hypertension with microalbuminuria in subjects <45 years of age. The present results suggest that in nondiabetic premenopausal women, subclinical kidney damage develops more frequently than in age-matched men with the same BP level.
Limitations
A limitation of this study may be the higher proportion of men compared to women. However, this was the result of the screening procedure. Most subjects were recruited in the years1990–1993, and until 1999, European guidelines did not consider microalbuminuria or LVH as criteria for initiating antihypertensive treatment in subjects with BP<160/100 mm Hg. However, the same guidelines were applied to men and women, and median follow-up did not differ between genders. Another possible limitation is that we did not measure the level of estradiol in our female participants. This would have allowed us to ascertain whether the high rate of TOD in the hypertensive women was due to levels of estradiol different from those in normotensive women.
Conclusions
This analysis highlights important differences in end-organ involvement between premenopausal women and age-matched men in the early stage of hypertension. Although the men and women had similar initial BP levels and a similar susceptibility to develop hypertension needing antihypertensive treatment, women showed a tendency to a faster deterioration of TOs during follow-up. The increased risk of developing hypertensive complications may reduce or even reverse the sex differential seen in the general population, in which women appear to be relatively protected from CVD until menopausal age. These findings warrant further investigation and may have important implications for future preventive and therapeutic measures in hypertensive premenopausal women.
Footnotes
Disclosure Statement
No competing financial interests exist.
Acknowledgments
This study was funded by the University of Padova, Padova, Italy, and by the Associazione “18 Maggio 1370,” San Daniele del Friuli, Italy.