
Abstract
Background:
We sought to determine if type 2 diabetes mellitus (T2DM) was associated with accelerated decline in domain-specific measures of cognitive function and fine motor speed.
Methods:
Women aged 65–80 years who were enrolled in a clinical trial of postmenopausal hormone therapy were grouped as having T2DM (n=179) or not (n=1984) and followed for an average of 5 years with annual standardized assessments of domain-specific cognitive function. Mean patterns of cognitive measures over time were contrasted between groups using general linear models and Wald tests, with varying levels of covariate adjustment. The influences of age at onset, use of oral medications, and use of insulin were also examined.
Results:
T2DM was associated with mean deficits of 0.2–0.4 standard deviations (SD) across follow-up in most cognitive domains. Consistent evidence that rates of decline were accelerated among women with T2DM was evident only for verbal knowledge and verbal memory (p<0.05). Decrements in fine motor speed, but no measure of cognitive function, were greater for women with earlier onset T2DM. Use of oral diabetes medications was associated with better relative cognitive function.
Conclusions:
In these women, T2DM was associated with cognitive deficits in most domains. Relative deficits in verbal knowledge and verbal memory may continue to increase after deficits in other domains have stabilized. Relative deficits in fine motor speed may be greater among women with earlier onsets of T2DM. Use of insulin, which may reflect greater T2DM severity, was associated with relatively greater cognitive deficits.
Introduction
Type 2 diabetes mellitus (T2DM) has long been known to increase one's risk for impaired cognitive function and dementia. 1,2 Cognitive deficits have been reported across many domains, including executive function, memory, learning, and processing speed. 3 –7 Despite this, there is not clear evidence that the rate of decline in cognitive function is accelerated among individuals who have T2DM, with some reporting no difference 4,8,9 and others reporting accelerated rates of decline. 10,11
Using data from an annual battery of cognitive tests administered to a large cohort of women who participated in a trial of postmenopausal hormone therapy (HT), we investigated the longitudinal patterns of relative deficits in domain-specific cognitive assessments among women with T2DM. We then examined whether T2DM was associated with an increased rate of cognitive decline across up to 7 years of follow-up. We also examined, among women with T2DM, if the age at T2DM onset and use of T2DM medications influenced these associations. Use of medications, in particular insulin, may serve as a marker of disease severity.
Materials and Methods
The Women's Health Initiative Memory Study (WHIMS) began enrolling its 7479 participants from the parent Women's Health Initiative (WHI) HT trials in May 1996. 12 These women were between 65 and 79 years of age at initial screening and were appropriate candidates for postmenopausal HT. Women without a uterus were randomly assigned with equal probability to take one daily tablet that contained either 0.625 mg of conjugated equine estrogen (CEE) (Premarin™, Wyeth-Ayerst, Philadelphia, PA) or a matching oral placebo in the WHI CEE-Alone trial. In a similar manner, women with a uterus were randomly assigned to take one daily tablet that contained either 0.625 mg CEE with 2.5 mg medroxyprogesterone acetate (MPA) (PremPro™, Wyeth-Ayerst) or placebo in the WHI CEE+MPA trial.
The Women's Health Initiative Study of Cognitive Aging (WHISCA) enrolled 2304 participants from 14 of the WHIMS clinical sites beginning in September 1999. 13 These women had been randomly assigned to WHI treatments an average (standard deviation) [SD]) of 3.0 (0.7) years before enrollment in WHISCA and were free of dementia, according to the WHIMS protocol. Enrollment rates into WHISCA were not related to prior diabetes. 14,15 The National Institutes of Health (NIH) and Institutional Review Boards for all participating institutions approved protocols and consent forms. Informed written consent was obtained from all participants.
The WHI CEE+MPA trial was terminated earlier than planned, in July 2002, because significantly more noncognitive adverse events occurred among women assigned to HT compared to placebo. In 2004, the WHI CEE-Alone trial was terminated earlier than planned because the excess risk of stroke in the HT group was judged to be unacceptable for healthy women in the absence of benefit for coronary heart disease (CHD), the primary outcome of the WHI HT trials. During 2004–2005, 84% of the women reconsented for extended annual follow-up, which continued until September 2007, at which point 53% of the women were seen within 18 months of the end of follow-up and 4% had died. 16 Results from all cognitive assessments from initial WHISCA enrollment to the end of extended follow-up, a maximum of eight examinations, are presented in this report. Women with T2DM averaged 4.7 (2.0) examinations compared to 5.5 (2.0) for other women (p<0.001). Women with and without T2DM had an average of 2.8 (1.0) visits during the WHI trials. After termination of these trials, 72.1% of the women with T2DM compared to 84.5% of those without T2DM were seen at least once, resulting in an average of 1.8 (1.7) compared to 2.8 (1.7) posttrial visits.
Diabetes
Diabetes status at WHI enrollment was based on self-report of ever being diagnosed by a clinician as having “sugar diabetes” when not pregnant. Age of first diabetes diagnosis was reported only by decade, which did not provide sufficient information for us to analyze diabetes duration. During each semiannual or annual follow-up contact, women were asked about medications, and positive responses to “pills for diabetes” and “insulin shots for diabetes” were used to classify incident diabetes. A confirmation study showed that 80% of self-reported treated diabetes was confirmed by drug inventory. Among a subset of women who had a fasting blood glucose measurement at baseline and self-reported ever having been told by a physician they had “sugar diabetes,” 73% had fasting glucose levels>125 mg/dL. 17
WHISCA enrollees include 179 women with T2DM, of whom 143 reported onset before WHI enrollment and 36 who initiated treatment for T2DM between their dates of WHI and WHISCA enrollment. We eliminated 140 women because their T2DM status at the time of WHI enrollment was not known or because they first reported T2DM during WHISCA follow-up (and may have been undiagnosed at the time of WHISCA enrollment). We contrast the 179 T2DM cases with the remaining 1984 women in WHISCA.
Cognitive assessments
An annual battery of cognitive measures in WHISCA included the Primary Mental Abilities Vocabulary (PMAVoc) test to assess verbal knowledge, letter and semantic fluency tests to assess verbal fluency, the Benton Visual Retention Test (BVRT) to assess short-term figural memory, the California Verbal Learning Test (CVLT) to assess verbal memory, the Digit Span Forward and Backward Test (DigSp) to assess attention and working memory, the Card Rotations Test (CRT) to measure spatial ability, the Finger Tapping Test (FTT) to assess fine motor speed, and the Modified Mini Mental State (3MS) Exam to assess global cognitive function. 13 Quality control was maintained through recertification of test administrators twice during the first year and annually thereafter.
Cognitive risk factors and medications
We consider the following risk factors for cognitive deficits, which were chosen because they may also be related to T2DM. Baseline age, education, race/ethnicity, prior myocardial infarction (MI), and prior stroke were collected via self-report. Symptoms of depression were collected with a validated questionnaire (Burnam score>0.06). 18 Hypertension was defined as a measured systolic blood pressure≥140 mm Hg, a diastolic blood pressure ≥90 mm Hg, or being on antihypertensive drug therapy. Physical activity was determined by a questionnaire that addressed the frequency, duration, and intensity of a woman's participation in different forms of physical activity each week. Total energy expended from recreational physical activity per week per kilogram was calculated by multiplying an assigned energy expenditure level for each category of activity by the hours exercised per week and summing values for all of the types of activities. 19 Anthropometric measures, including body weight, were collected by clinic staff using standardized techniques, with body mass index (BMI) calculated as weight (in kilograms) divided by squared height (in meters).
Statistical methods
We first standardized individual scores on each outcome measure by dividing their difference from the cohort mean at the initial WHISCA examination by their SD. For cognitive domains assessed by more than one outcome measure, we averaged the standardized scores of these outcomes and renormalized these averages to have SDs of 1; this involved averaging the separate phonemic and category verbal fluency tests, the two word lists of the CVLT along with its short-delay and long-delay recall scores, and FTT scores from the dominant and nondominant hands. Scores from the BVRT were subtracted from zero so that higher scores expressed better performance.
Differences in risk factors for cognitive impairment collected at WHI enrollment between women in the T2DM and no T2DM groups were assessed with chi-square tests. Mean scores from cognitive tests at WHISCA enrollment were compared between groups with t tests. Comparisons between average standardized scores collected over follow-up between groups (i.e., the relative deficit associated with T2DM) were based on general linear models fitted by maximum likelihood estimation. 20 We used a first-order autocorrelation model for repeated measures over time. Two levels of covariate adjustment were made: limited adjustment (for age and WHI treatment assignment) and full adjustment (in addition, all other risk factors). Within the cohort of women with T2DM, parallel approaches were used to examine mean differences associated with age when T2DM was first diagnosed and use of oral diabetes medications or insulin. To summarize these relationships, a composite score was formed by averaging the standardized scores from the individual domains and norming this average to have SD equal to 1.
To assess whether cognitive function was declining more rapidly among women with T2DM, we again used linear mixed models but reparameterized these to compare fitted slopes between women with and without T2DM using a test of interaction, with covariate adjustment for other risk factors. The incompleteness of follow-up required a cautious approach to analysis and interpretation, particularly for comparing rates of change. These analyses, based on maximum likelihood and incorporating covariate adjustment for factors that are related to both outcomes and missing data, provided some adjustment for potential bias related to missing outcomes, but because poorer health (including T2DM and poorer cognitive function) is often related to increased loss to follow-up, these statistical methods are not likely to capture cognitive decline fully and may lead to bias in estimating how T2DM is associated with rates of decline. To support these analyses, we used the initial WHISCA cognitive test scores as covariates and examined whether rates of decline across subsequent visits varied by T2DM status after controlling for cognitive function at the initial visit. This approach would be expected to reduce statistical power (shortening the span of follow-up that participants contributed to follow-up by 1 year) but would adjust for baseline cognitive function as a potential predictor of missing data. As noted, T2DM status was not related to on-trial retention rates; we, therefore, also conducted supplemental analyses limited to this period of time.
Results
Table 1 describes characteristics of the women included in our analyses as they were recorded at enrollment into the WHI. Women with T2DM were more likely to be African American, heavier, and less physically active, to have histories of hypertension, MI, and stroke, and to have symptoms of depression. Also in Table 1 are mean scores from the tests of cognitive function and fine motor speed at WHISCA enrollment, an average of 3.0 years later. Women with T2DM had significantly (p<0.05) lower raw scores at this time on all tests except those for attention and working memory and spatial ability.
Symptoms of depression are defined by a Burnam score>0.06.
Higher score reflects poorer function.
BVRT, Benton Visual Retention Test; CVLT, California Verbal Learning Test; METs, metabolic equivalents; MI, myocardial infarction; PMAVoc, Primary Mental Abilities Vocabulary; 3MS, Modified Mini Mental State.
Table 2 presents results from analyses to assess mean differences in test scores over follow-up (i.e., averaged across all visits from general linear models) between women with and without T2DM. T2DM was associated with relative deficits in all mean scores, with all but attention and working memory and spatial ability reaching nominal statistical significance (p<0.05) in both minimally and fully adjusted models. The magnitudes of the significant mean deficits ranged from 0.17 to 0.39 SD units across models. Table 2 also presents results from examining whether relative rates of decline in cognitive function tended to be accelerated among women with T2DM. In models adjusted for all covariates in Table 1, relative deficits between women with T2DM compared to those without increased over time for verbal knowledge (p=0.002), attention and working memory (p=0.007), and verbal memory (p=0.04) at rates slightly greater than 0.02 SD per year. The more conservative analyses (Table 2, right columns) found statistically increased rates of decline for verbal memory (p=0.005) and verbal knowledge (p=0.04) but not for attention and working memory. Figure 1 presents fully covariate-adjusted mean verbal knowledge scores over time for women grouped by T2DM status to portray the pattern of increasing deficits over time (the patterns for verbal memory deficits were similar). Because race was a potential confounder, we repeated the analyses on the subset of Caucasian women and found comparable results (data not shown). We found significant deficits in all cognitive domains when analyses were limited to the data collected during the WHI trials; however, this shorter time frame hampered our ability to determine if these were changing over time.
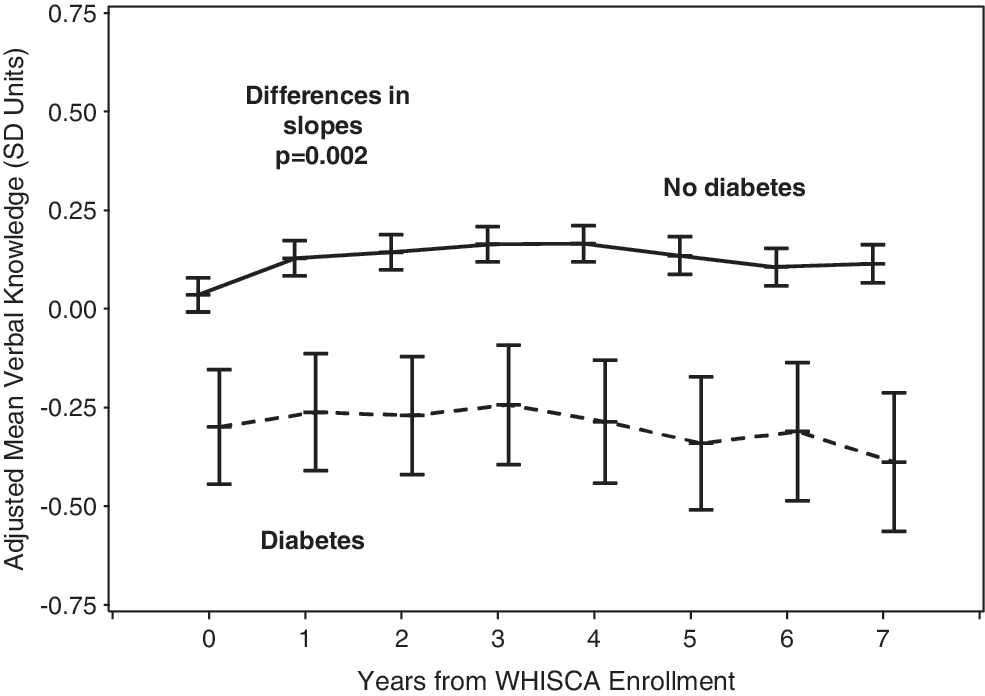
Fitted mean (95% confidence interval) verbal knowledge scores (in standard deviation [SD] units) after covariate adjustment for all factors in Table 1.
Analyses to examine whether relative deficits expanded over follow-up by comparing slopes also are included.
Limited to rates of change beginning at visit 2.
SD, standard deviation; SE, standard error.
Within the cohort of 179 women with T2DM, we fitted a regression model to examine whether any of the factors in Table 1 had independent associations with test scores across follow-up. After controlling for education, age, and race/ethnicity, none of the other factors had significant consistent relationships. We then examined whether age at reported T2DM diagnosis was associated with test scores, with adjustment for the risk factors in Table 1 (including age of WHI enrollment). The 55 (30.7%) women who reported being diagnosed with T2DM before the age of 60 tended to have lower covariate-adjusted mean test scores for most domains; however, only those for fine motor speed reached nominal statistical significance (p=0.003). The magnitude of this mean deficit averaged 0.41 (0.31) SD units across follow-up.
Women were grouped according to whether they used both insulin and oral medications at some time during follow-up (n=26), only used oral medications (n=88), only used insulin (n=25), or never used medications (n=40). Table 3 presents the relative differences in mean cognitive function tests over time associated with use of oral medications and insulin and tests of interactions. All risk factors in Table 1 were included as covariates, and we report p values from marginal comparisons. Use of oral medications was associated with a 0.2–0.4 SD unit better cognitive performance in most domains; however, these differences did not reach nominal statistical significance except for verbal knowledge (p=0.01). Use of insulin was associated with mean relative deficits of 0.1–0.3 SD units in most domains, with the largest deficit for fine motor speed (p=0.04). There was little evidence for an interaction between the use of oral medications and insulin (however, power was low). To describe these findings more succinctly, we created a composite score by averaging the eight domain-specific scores and norming this average to have an SD of 1. In a parallel analysis, use of oral medications was associated with a mean (standard error [SE]) relative better performance of 0.34 (0.17) units (p=0.04). Use of insulin was associated with a nonsignificant mean relative worse performance of 0.28 (0.18) units (p=0.12). Figure 2 portrays the longitudinal trajectory of mean composite scores for women grouped by medication use. An omnibus test for mean differences over time yielded p=0.03; an omnibus test of mean differences among slopes yielded p=0.10.
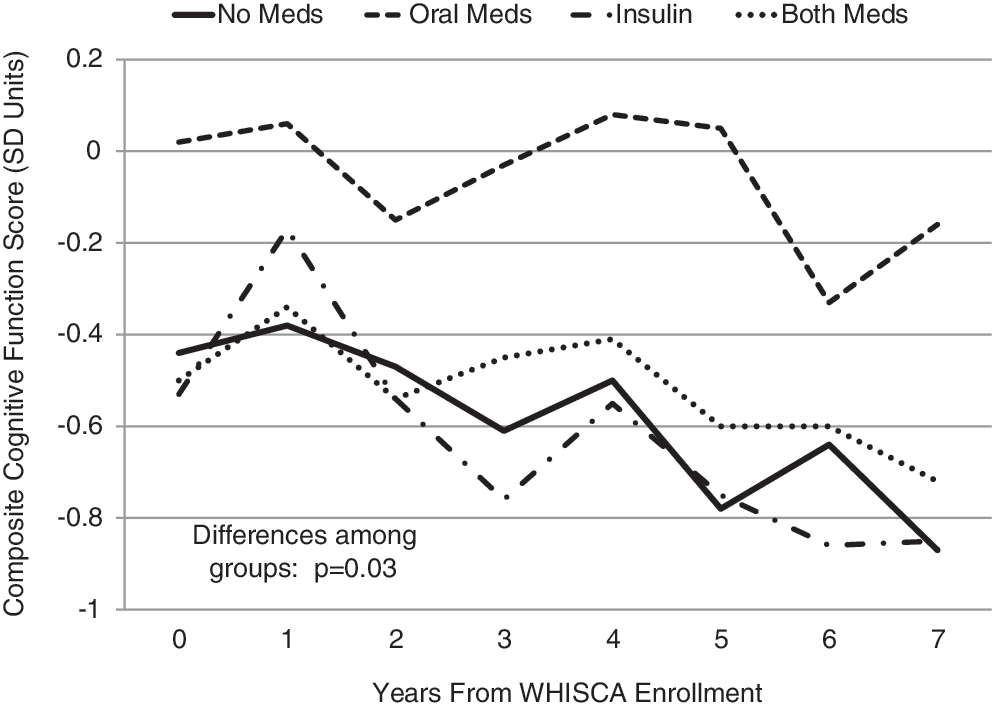
Mean composite of standardized scores through 7 years for women with diabetes who are grouped by use of oral medications with (n=26) or without (n=88) insulin (n=114), insulin use only (n=25), or no medications (n=40) at any time during follow-up, with adjustment for current age and all risk factors in Table 1. The p value (p=0.03) represents a test of differences among means over time. A test of differences among slopes yielded p=0.10. WHISCA, Women's Health Initiative Study of Cognitive Aging.
Results from repeated measures with adjustments for all factors in Table 1.
Discussion
T2DM adversely affects many aspects of brain health, increasing individuals' risk for cognitive deficits, cognitive impairment, Alzheimer's disease, stroke, diminished brain function, and brain atrophy. 21 –24 Known consequences of T2DM, including vascular disease, oxidative stress, dysregulated glucose metabolism, formation of advanced glycation end products, and chronic inflammation, are each associated with adverse brain health. 7,24 –27 T2DM is also associated with many other conditions that adversely influence cognition and brain function, including obesity, hypertension, dyslipidemia, and depression. 8,22,28,29 How well glucose levels are managed during T2DM may also affect cognition. 30 Jointly, these factors may be expected to induce a broad-based and sustained spectrum of cognitive deficits, with much heterogeneity from individual to individual.
Our analyses yielded four principal findings. First, on entry into a clinical trial of postmenopausal HT, women with T2DM had detectable deficits in many domain-specific cognitive functions that withstood extensive covariate adjustment. Second, we found consistent evidence that T2DM-related deficits in verbal knowledge and verbal memory were expanding over time. Third, the magnitude of cognitive deficits did not appear to be related to the age of T2DM onset, although deficits in fine motor speed were larger among women with earlier onset of disease. Finally, among women with T2DM, use of oral medications appeared to provide some benefit on a composite measure of cognitive function.
Cognitive deficits associated with T2DM
Many authors have found T2DM to be associated with a broad spectrum of cognitive deficits. Our analyses revealed mean deficits of 0.2–0.4 SD units in global cognitive function, verbal knowledge, verbal fluency, figural memory, verbal memory, and fine motor speed, which remained statistically significant, although reduced in magnitude, after extensive covariate adjustment. Although the affected domains vary from study to study, the magnitude of decrements, when detected, are generally consistent with our observations. 5,8,11,31,32
Some mechanisms through which T2DM may adversely affect cognition might be expected to produce diffuse and general impairments. One example is impaired vascular function and perfusion leading to cerebral infarcts, which although localized for individuals, may not be organized to produce characteristic patterns of deficits across domains. Other mechanisms may be more likely to differentially influence particular cognitive domains. The impairment of glucose transport across the blood-brain barrier that is associated with T2DM may affect tasks that require greater amounts of glucose uptake. 33 Insulin receptors are not uniformly distributed across the brain and are more concentrated, for example, in the hippocampus, so that mechanisms related to insulin resistance and insulin transport may differentially affect cognitive functions, such as memory, that are dependent on hippocampal integrity. 33 –35 The hippocampus has been reported to be particularly sensitive to hypoglycemia and T2DM-related atrophy. 36,37 However, the magnitudes of measured deficits and the affected domains may also be influenced by differences in the sensitivities of test and time courses of declines. 38
Rates of domain-specific cognitive decline
To determine if T2DM increases the rates of decline of domain-specific cognitive function, it is useful to have extended longitudinal series of measurements. In our analyses, T2DM was consistently associated with accelerated declines in verbal memory and verbal knowledge, after adjustment for covariates related to cognition and lost follow-up. Verbal memory has been reported elsewhere to be among the cognitive tasks most affected by poor glucose tolerance and insulin resistance, 33,34 so that the accelerated declines we see may be a continuing effect of the dysregulation of glucose metabolism. This is of particular concern because decrements in verbal memory can serve as early markers of underlying cognitive impairment. 39 Our inability to factor in diabetes duration and the potential nonlinearity in time courses of declines may have hampered our ability to detect differences in other cognitive domains.
We did not find evidence of accelerating rates of decline among women with T2DM for most cognitive domains, even when overall mean decrements were evident. This may mean that these declines occurred earlier in the disease, perhaps during prediabetes states when insulin resistance in the brain may first develop. 34,40 Separately from cerebrovascular disease, insulin resistance may accelerate the initial development of amyloid pathology, but not the later progression of Alzheimer's disease, 41,42 and thus may be tied to earlier expressions of deficits. Decrements in verbal knowledge tend to occur relatively late in the course of cognitive impairment, 38 so that the accelerated declines that we saw for verbal knowledge may reflect a trailing expression of these initial effects.
Associations between cognitive deficits and markers of T2DM severity
Overall, we found only weak and generally nonsignificant associations between age of T2DM onset and domain-specific cognitive function and decline. Stronger relationships were found for our test of fine motor speed. Deficits in this ability may reflect poorer brain health but also may arise from local neuropathy and more general declines in physical function, each of which has been linked to T2DM severity. Among individuals with type 1 diabetes, poorer glycemic control is associated with decrements in psychomotor efficiency and motor speed, 43 which may parallel our findings.
Use of diabetes medications
Evidence that oral medications and insulin therapy have direct effects on cognition among individuals with T2DM is scant and based on short-term trials or observational studies. 44,45 Adequately powered randomized clinical trials are needed to establish long-term effects. In our analyses, women who used oral medications to treat their T2DM appeared to have relatively better cognitive test scores compared to those who did not. This effect appeared to be strongest for the domain of verbal knowledge but may have been evident to a lesser (albeit nonsignificant) degree for the other cognitive tests except for attention and working memory and fine motor speed. Use of insulin, however, was associated with a relative mean deficit in cognitive function in all domains except verbal memory; these relative deficits were slightly smaller in magnitude than the improvements associated with oral medications and did not reach nominal significance expect for fine motor speed. When we averaged domain-specific test scores to form a composite, we found that women using only oral medications appeared to outperform women using no medications or insulin (with or without oral medications). Insulin therapy is usually used when lifestyle interventions or oral medications do not achieve target glycemic control and, thus, may be a marker of disease severity, that is, reflective of women who have poorly controlled or severe and uncontrolled T2DM who may be at higher risk for cognitive decline and future development of dementia. Women who were on no therapy likely were a heterogeneous group that included both those with mild T2DM and those who were inadequately treated.
Limitations
As volunteers who were eligible for a clinical trial of postmenopausal HT, these women do not reflect more general populations, and it is likely that the levels of cognitive function were compressed, particularly at baseline. The definition of T2DM we used was based on treatment and self-report and may, in some cases, be inaccurate; however, its validity has been established in the WHI cohort. 17 We are not able to address diabetes duration or glucose control. In general, differences in the rates of change of our cognitive measures may vary depending on the psychometric properties of these measures. For example, how a 1 unit of change in a test score relates to a meaningful change in cognitive function may vary depending on the initial level. The associations we found between cognitive function and medication use fall far short of the evidence that a randomized clinical trial would provide and did not take into account medication adherence, the number or doses of medication, or specific medication types. Our approach is descriptive; results from many inferences are presented without control of type 1 error.
Conclusions
T2DM was associated with mean deficits of 0.2–0.4 SD during follow-up in most cognitive domains. Deficits in verbal knowledge and verbal memory continued to expand during the course of T2DM, although other cognitive domains did not show significant T2DM-associated acceleration in cognitive decline. Greater deficits in fine motor speed were associated with earlier onset of T2DM. Use of insulin, which may mark T2DM severity, was associated with poorer performance.
Footnotes
Acknowledgments
The Women's Health Initiative Study of Cognitive Aging was supported by the Department of Health and Human Services and the National Institute on Aging (NO1-AG-1-2106). The Women's Health Initiative program is funded by the National Heart, Lung, and Blood Institute. Wyeth Pharmaceuticals provided the study drug and the placebo to the WHI trial. The Women's Health Initiative Memory Study was funded by Wyeth Pharmaceuticals, Wake Forest University, and the National Heart, Lung, and Blood Institute. S.M.R. is supported by the Intramural Research Program, National Institute on Aging, and National Institutes of Health.
National Institute of Aging, Baltimore, MD: Alan Zonderman, Susan M. Resnick.
Wake Forest School of Medicine, Winston-Salem, NC: Sally Shumaker, Principal Investigator; Stephen Rapp, Mark Espeland, Laura Coker, Deborah Farmer, Anita Hege, Patricia Hogan, Darrin Harris, Cynthia McQuellon, Anne Safrit, Lee Ann Gleiser, Candace Goode, Mary Barr, Carolyn Bell, Linda Allred, Sonya Ashburn.
Women's Health Initiative, Durham, NC: Carol Murphy; Rush Presbyterian-St. Luke's Medical Center, Chicago, IL: Linda Powell; Ohio State University Medical Center, Columbus, OH: Rebecca Jackson; University of California at Davis, Sacramento, CA: John Robbins; University of Iowa College of Medicine, Des Moines: Robert Wallace; University of Florida, Gainesville/Jacksonville: Marian Limacher; University of California at Los Angeles: Howard Judd (deceased); Medical College of Wisconsin, Milwaukee: Jane Kotchen; The Berman Center for Outcomes and Clinical Research, Minneapolis, MN: Karen Margolis; University of Nevada School of Medicine, Reno: Robert Brunner; Albert Einstein College of Medicine, Bronx, NY: Sylvia Smoller; The Leland Stanford Junior University, San Jose, CA: Marcia Stefanick; The State University of New York, Stony Brook: Dorothy Lane; University of Massachusetts/Fallon Clinic, Worcester: Judith Ockene.
The following investigators were the original investigators for these sites: Mary Haan, Davis; Richard Grimm, Minneapolis; Sandra Daugherty (deceased), Nevada.
National Heart, Lung, and Blood Institute: Barbara Alving, Jacques Rossouw, Linda Pottern.
Fred Hutchinson Cancer Research Center, Seattle, WA: Deborah Bowen, Gretchen Van Lom, Carolyn Burns.
Disclosure Statement
No competing financial interests exist.