
Abstract
Background:
Whether or not cesarean delivery is associated with increased risk of postpartum depression (PPD) remains unclear.
Methods:
We carried out a prospective cohort study between February and September 2007 in Hunan Maternal and Infant Hospital and the First Affiliated and Third Affiliated Hospitals of the Central South University in Changsha, Hunan, People's Republic of China. The Chinese version of the Edinburgh Postnatal Depression Scale (EPDS) was used at 2 weeks postpartum to assess PPD, with a score of ≥13 as the cutoff for PPD.
Results:
A total of 534 women were included in the final analysis, with 415 (77.7%) delivering by cesarean section (the majority of them with no medical indication). The rate of PPD was 21.7% in women who had a cesarean delivery and 10.9% in women who delivered vaginally. The increased risk of PPD in women who had cesarean sections was maintained after we adjusted for potential confounding factors or considered cesarean delivery by social indications.
Conclusions:
Cesarean section is associated with increased risk of PPD in Chinese women with a high cesarean delivery rate.
Introduction
Postpartum depression (PPD)
Previous studies on the association between cesarean delivery and PPD have yielded inconsistent results; some found a positive association, 18 –22 while others did not. 23 –26 All the studies with positive results were observational in nature; thus, one cannot be sure if the onset of PPD was a result of the procedure itself or of the underlying medical condition necessitating the procedure. 17 Only one randomized controlled trial (RCT) examined this issue, but it failed to observe an association between the mode of delivery and PPD. 26 The authors acknowledged that the high cesarean delivery rate in the planned vaginal delivery group may have weakened the association between the mode of delivery and PPD. 26
The rate of cesarean delivery has shown a continuous increase in Canada, the United States, and other industrialized countries in the past decade 27 –29 and has been increasing rapidly in some middle-income countries, such as Brazil and China, reaching the alarming levels of 50%–70%. 30,31 A majority of these surgeries were performed because of social reasons. 31 In 2007, we conducted a prospective study in China to assess the risk factors of PPD in a cohort of Chinese women. We collected data on a number of maternal and infant characteristics, including the mode of delivery. 32 The cesarean delivery rate in this cohort of Chinese women was very high (>70%), and the majority had no medical indication. We thought this cohort would be ideal to examine the association between cesarean delivery and PPD because the result is unlikely to be confounded by underlying medical conditions, as most surgeries were performed with no medical indication.
Materials and Methods
Subjects were recruited between February and September 2007 from Hunan Maternal and Infant Hospital and the First Affiliated and Third Affiliated Hospitals of the Central South University in Changsha, Hunan, People's Republic of China, during their prenatal visits at 30–32 weeks of gestation. Primiparous married women aged 20–45 years seeking prenatal care and planning to stay in Changsha city during the postpartum period were invited to participate in the study. Informed consent was obtained from study participants in accordance with approved protocols of the Research Ethics Board of Central South University.
We excluded women with a multiple pregnancy or with current or past history of bipolar disorder, psychotic disorders, or a major chronic disease or obstetric and pregnancy complication (severe preeclampsia/eclampsia, placenta previa, placental abruption, major postpartum infection, stillbirth, major birth defects, or birth weight <1500 g) as recorded in medical charts because these conditions may increase the risk of PPD 7 and could introduce bias into the study.
Baseline clinical and demographic data were collected at 30–32 weeks of gestation. We followed participating women for 2 weeks after childbirth to collect obstetric data, to measure their social support level, and to screen for PPD. We chose this follow-up period for two reasons. First, in Changsha, women typically have their routine postpartum visit at 2 weeks after childbirth, and we could incorporate our data collection to their routine care, which, we expected, would reduce the women's burden and improve compliance. Second, PPD onset is within 4 weeks after childbirth, 1 and, therefore, our follow-up time was in the window for ascertainment of PPD. Research nurses conducted face-to-face interviews with participating women to collect relevant clinical and demographic data, using a standardized case report form to record demographic and obstetric data. Demographic data collected included maternal age, education, household income, and housing conditions. Obstetric data consisted of planned/unplanned pregnancy, gravidity, mild pregnancy and delivery complications (subjects with major complications were excluded from this study), gestational age at delivery, birth weight, infant sex, mode of delivery, and types and indications of cesarean delivery. Cesarean delivery was divided into two types: elective and emergent. Indications of cesarean delivery were grouped into three categories: medical, social, and medical plus social. No specific reason for social indication for cesarean delivery was collected as data, however.
Postnatal social support levels were measured using the Social Support Rating Scale (SSRS) 33 at 2 weeks postpartum. The SSRS consists of 10 items, with three dimensions: subjective support (4 items), objective support (3 items), and support availability (3 items). Higher scores indicate a higher level of support, with a maximum of 66. This scale was based on the unique environmental and cultural conditions in China and has demonstrated high reproducibility (0.92) and internal consistence (0.89–0.94). 33 The Chinese version of the Edinburgh Postnatal Depression Scale (EPDS) was used at 2 weeks postpartum to assess PPD, with a score of ≥13 as the cutoff for PPD. 34 Previous studies have demonstrated the reliability and validity of the EPDS for the identification of depression, and it has been widely applied in both research and clinical settings. 34 The sensitivity (0.82) and specificity (0.86) of the Chinese version of the EPDS are comparable to those of the original scale. 34
Demographics, perinatal characteristics, postnatal social support scores, and PPD rate were compared between women who had cesarean delivery and those who had vaginal delivery. To assess whether and to what extent reasons for cesarean delivery influenced the association between cesarean delivery and PPD, we compared PPD rates between women who had an emergent cesarean delivery and women who had an elective cesarean delivery. We also compared PPD rates among women with different indications for cesarean section. Because of limited sample size, we categorized indications for cesarean section into three groups: medical, social, and social plus medical. Social indication was defined as cesarean section performed at woman's request with no documented medical/obstetric complications that may require a cesarean section; social plus medical indication was defined as cesarean section performed at woman's request but with medical records indicating mild medical/obstetric complications that might require a cesarean section.
Adjusted odds ratio (OR) and 95% confidence interval (CI) were estimated by multiple logistic regression, with PPD as the dependent variable and mode of delivery, maternal age, household income, gestational age at delivery, pregnancy complications, delivery complications, birth weight, infant sex, and total postnatal social support score as the independent variables. All selected independent variables were entered and retained in the final regression model. A combination of preliminary analysis of our data and biologic rationale was used in the selection of the confounding variables to be entered into the multiple logistic regression model. For example, although lack of accompanied delivery and early contacts were associated with PPD, they were both components of the social support network. To avoid overadjustment and a potential collinearity problem, we did not use both variables in the regression model. For the same reason, we chose to include only postnatal social support in our model because in our previous study, we found that the effect of postnatal social support on PPD was much stronger than that of prenatal social support. 32 In our previous study, we found that infant sex was an important determinant of PPD in Chinese women, 6 and in the preliminary analysis, we found a difference in the male/female ratio between vaginal and cesarean delivery groups. Thus, we elected to include infant sex in the regression model to ensure that potential confounding due to sex imbalance would be adequately adjusted for. All analyses were performed using SPSS version 13.0 (SPSS Inc., Chicago, IL).
Results
A total of 666 women were invited to participate in the study, and 634 women consented and completed the prenatal survey. At 2 weeks postpartum, 24 women withdrew, 25 were lost to follow-up, and 10 had missing information for over 20% of the variables. Forty-one other women were excluded because of records of major psychiatric disorders and severe obstetric or pregnancy complications, leaving 534 women (86.8% of the consenting women at 30–32 weeks of gestation) for analysis (Fig. 1). We made a comparison of the baseline characteristics between the 60 women who were lost to follow-up and those who completed the follow-up and found no difference (data available on request). Women who had a cesarean delivery tended to be slightly older, with higher household income, higher rates of low and high birth weight, and higher postnatal social support, than women who had a vaginal delivery (Table 1).
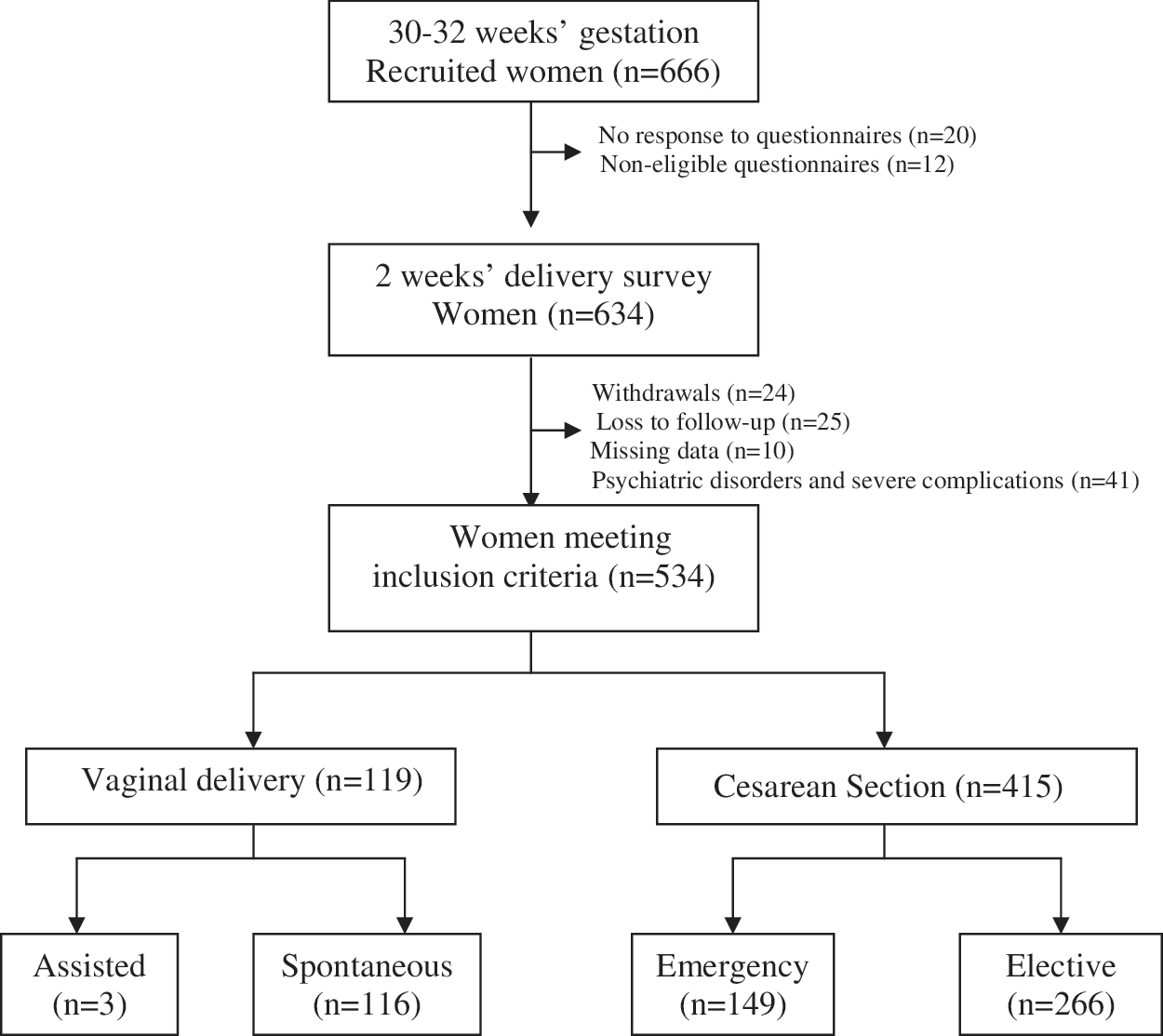
Recruitment and follow-up of study subjects.
One hundred three women (19.3%) were screened positive for PPD. The rate of PPD was significantly higher in women who had a cesarean delivery than in those who delivered vaginally (Table 2). Table 3 shows that the PPD rate was higher in the group who had elective cesarean delivery than in the group who had emergent cesarean delivery. The rate of PPD in the group with both medical and social indications was slightly higher than that in those with either a medical or a social indication alone, although the differences were not statistically significant (Table 3).
Adjusted factors: maternal age, household income, gravidity, gestational age, pregnancy complications, delivery complications, birth weight, infant sex, and postnatal social support score.
CI, confidence interval; OR, odds ratio.
Adjusted factors: maternal age, household income, gravidity, gestational age, pregnancy complications, delivery complications, birth weight, infant sex, and postnatal social support score.
Discussion
Our study of a cohort of Chinese women found that PPD occurred in about 19% of the parturient women. This rate is similar to that in previous studies conducted in China. 6,8 –11 The distribution of demographic characteristics in our study population, such as exceptionally high cesarean delivery rate, is consistent with the demographic characteristics of Chinese pregnant women reported in earlier Chinese literature. 6,35,36 Our study findings also concur with earlier studies in that cesarean delivery was significantly associated with a greater risk for developing PPD; women who had cesarean delivery had >2-fold increased risk compared to women who delivered vaginally. 18 –22
Our study compares favorably with previous studies in the field. Although women who had a cesarean delivery tended to be older, with slightly higher household income, higher rates of low and high birth weight, and higher postnatal social support, these differences were clinically small. In addition, we used multiple logistic regression to adjust the potential confounding by these factors. Social support is an important risk factor for PPD, 7,32 which has seldom been adjusted for in previous studies on the association between cesarean delivery and PPD. 17 –26 Most women who had a cesarean delivery did it for a social reason rather than for a medical indication. We excluded women with severe maternal and neonatal complications; thus, women with a medical indication for cesarean section may have had mild rather than severe conditions.
In our study, most of the medical indications for cesarean delivery recorded (>90%) were mild conditions, such as fetal distress, lack of progress, dystocia, and oligohydramnios (data available on request), suggesting that confounding by indication may not have played an important role in the increased risk of PPD in women having a cesarean section. The large number of cesarean delivery cases with no medical indication allowed for a comparison of PPD rates between cesarean delivery cases with medical indications and those with nonmedical indications, as well as an assessment of whether the observed effect of cesarean delivery on PPD should be attributed to the procedure itself or to the conditions requiring the procedure. For example, the PPD rate was higher in women with an elective cesarean delivery, most of whom had a social indication, than in women with an emergent cesarean delivery, all of whom had a medical indication. This further confirms that confounding by indication was not an important problem in our study. One RCT found no association between mode of delivery and PPD. 26 This was a two-armed parallel trial comparing planned vaginal delivery with planned cesarean delivery in women with breech presentation. 26 More than half of the planned vaginal delivery subjects were switched to cesarean delivery because of safety concerns. 37 The high cesarean delivery rate in the planned vaginal delivery group may have weakened the association between mode of delivery and PPD, as the authors analyzed the data using an intention-to-treat approach. 26
These are some limitations. We used the EPDS and a demanding cutoff point to classify women as depressed or not. It should be noted that the EPDS is a screening measure and does not constitute a diagnosis for depression. As a result, we cannot be certain that our findings would be directly transferable to patients meeting the DSM-IV criteria for depression. The study sample was not sufficiently large, especially regarding the need to analyze the effects of specific types or indications of cesarean delivery. For example, the rate of PPD in the group with both medical and social indications was higher than in those with either medical or social indication alone, but because the number of women with both medical and social indications was small, the differences were not statistically significant. Even for results that were statistically significant, the CIs tended to be wide, suggesting that our study may have been underpowered. Also, we did not collect data on some important confounding factors, such as history of depression and mental health, anxiety during pregnancy, postpartum bleeding, length of hospital stay, and costs of hospital stay. As a result, we were not able to examine the impact of these factors on the results of our study. In addition, selection bias might have occurred during the recruitment process (i.e., patients at either end of the emotional spectrum might not be inclined to participate). We do not know how representative of the general population the women in this study were, and this may affect the generalizability of the study.
The mechanisms of the effect of cesarean section on PPD, if they exist, would be complex. Although our study benefitted from a high proportion of no medical indication for cesarean delivery, making confounding by indication less of a concern, many other unmeasured factors, such as complications of the surgery and patient's personal experience/preference, may have played a role in the increased risk of PPD. Wound infection, hemorrhage, and anesthetic complications may have adverse effects on women's mental health, whereas surgery without complications may have no such effects. On the other hand, the attitude toward childbirth in women who requested a cesarean section may be different from the attitude of women who did not make such a request. Saisto et al. 24 observed that the more anxiety, neuroticism, vulnerability, depression, low self-esteem, dissatisfaction with partnership, and lack of social support the women reported, the more they showed pregnancy-related anxiety and fear of vaginal delivery. 24
We have not been able to collect information on surgical complications or specific reasons for social indications for cesarean delivery. According to the Chinese literature, the reasons most frequently provided for women who had no medical indication but chose cesarean delivery included the following: a particular date of delivery could bring fortune to the baby, vaginal delivery may do physical harm to the baby, and vaginal delivery may affect the intellectual development of the baby. 31,38,39 We speculate that the anxiety for a healthy and intelligent baby rather than the surgical procedure or the underlying medical complication requiring the surgical procedure may have played an important role in increasing the risk of PPD in women who underwent a cesarean delivery. The hypothesis that cesarean section may have greater impact on PPD in certain ethnic/cultural populations is consistent with the study findings on the association of infant sex and PPD. The risk for PPD was much higher in women who gave birth to a female infant compared with those who gave birth to a male infant in studies from India 40 and China, 6,8,41,42 but no such an gender-PPD association was observed in studies from Western societies, 7 suggesting that some risk factors may have greater impact on PPD in certain culturally vulnerable populations.
In summary, our prospective cohort study found that cesarean delivery was associated with increased risk of PPD in a cohort of Chinese women with high rates of nonmedically indicated cesarean sections. We do not know why these women were at increased risk of PPD. Regardless of the mechanisms, however, the possible negative impact of cesarean delivery on women's long-term mental health can be used as a red flag for healthcare providers. They should discuss with pregnant women both the short-term and long-term risks and benefits of a cesarean section, especially with women who have no evident medical indication for the surgery. Our findings may have important implications for development of measures/policies to control the ever increasing cesarean delivery rate observed in recent years in both industrialized and developing countries. Although cesarean section with no medical indication is rare in industrialized countries, healthcare providers and pregnant women may sometimes take the potential harm of cesarean section too lightly and make the decision too easily, causing the performance of unnecessary surgeries for mild conditions.
Footnotes
Acknowledgments
This study was supported by grants from the Hunan Provincial Natural Science Foundation (06JJ4055), Hunan Ministry of Science and Technology (06FJ4103), and Hunan Ministry of Education (06C072) of the People's Republic of China. R.-h. X is an Ontario-University of Ottawa Vision 2010 Postdoctoral Fellow. S.W.W. is a recipient of the Ontario Women's Health Council-Institute of Gender and Health of Canadian Institutes of Health Research (CIHR) Mid Career Award. M.W. is a new investigator of CIHR. We thank the pregnant women and the staff of the participating hospitals in Changsha, China, for their support.
Disclosure Statement
No competing financial interests exist for any authors related in this work.