
Abstract
Background:
Hypoactive sexual desire disorder (HSDD) has been estimated to occur in 10%–15% of adult women in large population-representative and community-based studies. However, none of these studies have used in-person diagnostic interview assessment to rule out alternative diagnoses, nor has the impact of other health conditions or help-seeking experiences been investigated. The current study aimed to determine the prevalence of generalized acquired HSDD in women aged ≥18 who attended primary care or obstetrics and gynecology clinics for nonurgent clinic visits in the United States.
Methods:
A total of 701 women were enrolled at 20 clinical sites across the United States between June 11, 2010, and October 15, 2010. Participants completed a two-part self-administered questionnaire, and a validated, structured, in-person diagnostic interview, conducted by a trained health professional was used for diagnosing HSDD according to DSM-IV-TR criteria.
Results:
Fifty-two women (7.4%) were assigned a diagnosis of generalized acquired HSDD. Prevalence was lower in minority and postmenopausal women. Level of education and other sociodemographic factors did not appear to differentiate between women with and without HSDD. A marked increase in HSDD prevalence was noted in the perimenopausal (i.e., 40–49 years) and immediate postmenopausal (i.e., 50–59) age groups. Of the women diagnosed with HSDD, 53% had sought care from a health professional for HSDD.
Conclusions:
In this sample of women recruited in the clinical care setting, we observed an overall prevalence rate of 7.4% of acquired, generalized HSDD, with markedly increased prevalence in midlife women.
Introduction
Hypoactive sexual desire disorder (HSDD) was first identified in the mid-1970s in defining contributions by Harold Lief, M.D., 1 and Helen Singer Kaplan, M.D., Ph.D. 2 Since that time, HSDD has received increasing attention as a relatively common and often distressing sexual disorder in women. 3 –6 Recent population level surveys of two of the primary symptoms of HSDD—decreased desire for sexual activity and sexually related distress—suggest that this combination of symptoms is present in up to 15% of U.S. women. 3,4,7 –9 Women with reduced sexual desire and sexually related distress have been shown to have increased rates of depression, reduced quality of life, and poorer sexual and relationship satisfaction. 8,10 –13 Despite these difficulties, <40% of women with symptoms of low desire and associated distress seek help for their problem, and there are no approved drug therapies for the disorder. 14
An important limitation in existing large prevalence studies is the lack of a rigorous, clinician-based diagnostic assessment of HSDD. In light of growing controversy concerning diagnostic criteria for sexual dysfunction in women 15,16 and the counter argument in favor of the Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV-TR) criteria, 17,18 the study design and method used for assessing HSDD diagnosis must be carefully implemented in a fashion faithful to the HSDD construct. Whereas previous community-based or epidemiologic studies have been based on self-report questionnaire measures for assessing individual components of HSDD or sexually related distress, methods such as these may overestimate the prevalence of the disorder by failing to take into account whether or not it conforms to HSDD diagnostic criteria, as defined by DSM-IV-TR. 17 To more accurately assess the prevalence of clinically diagnosed HSDD, it is essential to control for potential effects of false positive diagnoses through systematic investigation and exclusion of alternative diagnostic contributors. To accomplish this important goal, we selected a validated HSDD diagnostic tool 19 that provides for a structured interview and clinician-based assessment of the presence or absence of HSDD and specific criteria for establishing the diagnosis in each case. Only women with generalized, acquired HSDD, not accounted for by another major medical or psychiatric condition, prescription or nonprescription drug, surgery or other nonsexually related cause, were counted as true positive HSDD cases for the present study. Women with situational low desire attributed to life cyle changes (e.g., pregnancy or childbirth), temporary stress or fatigue, or current dissatisfaction with the partner relationship were similarly excluded from the diagnosis if their loss of desire was deemed to be context or situation specific.
A validated diagnostic tool, the Decreased Sexual Desire Screener© (DSDS), has recently become available for diagnosing HSDD according to DSM-IV-TR criteria. 19 The diagnostic method requires a combination of self-report and interview assessment and has been used in a number of treatment studies to date. Availability of this validated method of diagnostic assessment provides an opportunity for in-person, interview-based assessment of HSDD in a nationally representative clinic sample of women. Accordingly, the DSDS interview method was used to assess the primary end point of our study, that is, prevalence of clinically diagnosed HSDD in a representative range of women of varying ages and sociodemographic backgrounds.
Over and above lack of adequate diagnostic precision, we note that studies to date have not assessed HSDD and its clinical correlates in relevant healthcare settings. As the typical point of entry for women with HSDD into the healthcare system is via a primary care physician or women's health/gynecology provider, we sought to assess the clinical presentation of the disorder in these healthcare settings across geographic regions. Because these are the usual clinical settings for interactions to take place between women with HSDD and their healthcare providers, we aimed to optimize the generalizability of our findings by recruiting and interviewing women in the clinical settings of their typical healthcare visits. Previous studies have used a variation of this approach to investigate reproductive and contraceptive choices of women via in-depth interviews conducted in a clinic-based setting. 20,21 This is the first study to date to make use of this methodology in a large sample of women recruited for a multicenter, clinic-based study of HSDD.
Materials and Methods
A national, clinic-based study was designed to provide point prevalence estimates of generalized, acquired HSDD in women aged ≥18 based on clinician-based diagnostic interviews that conform to HSDD diagnostic criteria (DSM IV-TR). Women were recruited in primary care physician (PCP) and obstetrics and gynecology (OB-GYN) clinics across a wide variety of locations and practice settings. Sites were selected to provide a representative cross-section of practice settings and geographic regions. The study was terminated early because of funding cessation by the sponsor, Boehringer Ingelheim Pharmaceuticals, which occurred for reasons unrelated to the progress of the study or any aspect of study conduct. A total of 20 clinical sites (10 PCP and 10 OB-GYN) completed enrolment of 701 women between June 11, 2010, and October 15, 2010. Results from these initial interviews are presented here.
Sampling design
A stratified, cluster sampling design was used to obtain a sample representative of adult women who use the U.S. healthcare system. We used a geographic stratification design based on the U.S. Census distribution to identify representative sites in 49 counties. The 49 counties were randomly selected (proportional to the population of women ≥18) based on U.S. Census divisions (New England, Middle Atlantic, South Atlantic, East South Central, West South Central, East North Central, West North Central, Mountain, and Pacific) or regions (Northeast, Midwest, South, and West) and population density (urban, suburban, rural). One clinic (PCP or OB-GYN) was then randomly selected within each selected county to ensure broad geographic sampling. If completed, this study design would have permitted generalization of the results to the broader U.S. population of women using outpatient care at PCP and OB-GYN practices. Because the study was terminated prematurely, it was not possible to achieve representative sampling from all geographic regions as planned.
Site selection
In order to select one site per county within each county defined by the Census division and population density (urban, suburban, and rural), a list of PCP (internal medicine, family practice, or general practice) and OB-GYN providers was obtained from public-use sources. Once a clinical site was selected for a county, no other sites were contacted in that county. However, if a selected county had no eligible clinics or no clinic in that county agreed to participate, another county was selected using the same random sampling scheme.
Standardized diagnostic interview assessment of HSDD
A second key component of the study was the use of a standardized, validated interview assessment of HSDD status. 19 The DSDS was used for this purpose, and the interview was conducted by a trained and certified female, midlevel health professional interviewer. A rigorous diagnostic assessment was performed according to the instrument guidelines. The DSDS is a validated tool for use in the diagnosis of generalized, acquired HSDD in premenopausal and postmenopausal women. 19 It was developed to provide both expert and nonexpert clinicians with a brief, standardized diagnostic instrument for obtaining sensitive and reliable diagnosis of acquired HSDD in women. It consists of five questions, four of which assess symptoms of HSDD, including lack of desire and associated distress; the fifth is a multi-item question to aid the clinician in differential diagnosis. In a validation study of 263 women from 27 centers in North America, the DSDS (administered by a nonexpert clinician) was compared to a standard diagnostic interview (conducted by a clinician with expertise in sexual dysfunction); the sensitivity and specificity of the DSDS were 84% and 88%, respectively. The study sample in this validation study included women with HSDD, women with other types of female sexual dysfunction (FSD), and women with no FSD (and no HSDD). 19
Before the DSDS diagnostic interview, demographic data and health information were collected on a range of concomitant conditions and medical treatments. Participants completed the DSDS questions on paper, which were then verified by the interviewer. In order to be eligible for the diagnosis of HSDD, participants needed to answer Yes to the first four questions of the DSDS. For participants who responded Yes to the first four questions, the fifth multi-item question was used to aid the clinician in the differential diagnosis of HSDD. (Table 1).
In women who answered Yes to the first four questions, it was then necessary to determine if the HSDD symptoms were better accounted for by a medical, substance-related, psychiatric, or other sexual condition. To evaluate this, a differential diagnosis was performed according to standardized training and instruction of all interviewers. A series of probe questions was developed for the fifth multi-item question (available on request from first author) to ensure standardized assessment of alternative diagnoses, such as depression or the effects of a prescription medication. Each item to which a participant responded affirmatively was discussed further using the probe questions provided. Interviewers were instructed to use relevant data from the interview responses and medical history to make the diagnostic determination of generalized, acquired HSDD.
Participant self-administered questionnaire
A brief two-part paper-and-pencil self-administered questionnaire (SAQ) was completed by all study participants. Part 1 was completed before the HSDD diagnostic interview, and Part 2 was completed immediately after the diagnostic interview. Validated scales were used for assessing key domains of sexual function (sexual desire, arousal, orgasm, pain, satisfaction) and other quality of life and mental health measures. The validated measures included the DSDS, 19 the Female Sexual Function Index© (FSFI), 22 the Patient Health Questionnaire© (PHQ-2), 23 the Female Sexual Distress Scale Revised© (FSDS-R), 24 and the Sexual Desire and Distress Questionnaire (SDDQ).
Additional items were developed specifically for the study or were taken from the HSDD Registry 25 or the PRESIDE study. 14 Most of these questions were subjected to additional qualitative analysis in the HSDD registry pilot phase. 25 These questionnaires assessed key domains of demographic characteristics, relationship status and satisfaction, subjective well-being and mental health, physical well-being, physical and sexual abuse, health status, reproductive history, sexual function, sexual distress, treatment seeking, and healthcare use.
Participants
A broad age range of women, including representation of both premenopausal and postmenopausal women, were selected for participation. All women ≥18 years who attended the selected clinics for nonurgent visits and were capable of responding to assessments in English were considered for participation. A nonurgent clinic visit was defined as any visit that did not require urgent medical intervention or extensive medical evaluation that would preclude participation.
A key factor in the sampling plan was attempted consecutive recruitment of all available patients not seeking emergency care. To reduce selection bias, the first available patient was invited to participate and was recruited if eligible and willing, contingent upon the interviewer's availability. Available subjects who met eligibility criteria were required to provide signed, informed consent statements before participation. Institutional Review Board approval was obtained before any study activities.
We selected a target sample size by age decade (18–29, 30–39, 40–49, 50–59, 60–69, 70–79, 80+) for PCP clinics and one for OB-GYN clinics based on the national civilian noninstitutionalized population estimates of 2008 from the National Health Interview Survey (NHIS) and the proportion of women seeking care at a PCP/OB-GYN office in the last year based on the 2008 NHIS. Once a clinic achieved its target sample size for a given decade, additional women within that age decade were not eligible for the study. If an age decade could not be filled, women were added in the other age groups at that site in order to reach the site target sample size.
Interviewers
All study interviewers received in-person training and certification before conducting field interviews. Eight midlevel female health professional interviewers (i.e., nurse practitioners) attended prestudy training on DSM-IV-TR criteria and in administration of the DSDS, according to guidelines described by Clayton et al. 19 Certification was based on the demonstrated ability of the interviewer to perform diagnostic assessments with >90% reliability.
Statistical analysis
As a result of early study termination, analysis of study data was restricted to basic descriptive statistics, including frequencies and cross-tabulations. Missing data were not imputed, and planned weighting schemes were not implemented. Data shown in the accompanying tables and figures are derived only from those respondents who completed all parts of the study (interview and two SAQs).
Proportions for categorical variables and means and standard deviations (SDs) for continuous variables were used to describe the analysis sample. Participation rates were examined both overall and by clinic type. Crude estimates of HSDD prevalence rates were calculated to address the main objective of this study, in addition to associated demographic and medical history characteristics of the sample. All analyses were performed using SAS 9.2 (SAS Institute Inc., Cary, NC).
Results
Participation and response rates
Figure 1 shows enrollment and retention rates according to the type of clinical setting (PCP vs. OB-GYN). As shown, initial acceptance rates were higher (59%) in the OB-GYN settings than in PCP (44%) clinics. After completion of the informed consent process, <1% of women discontinued their participation during interview or questionnaire phases. A missing data rate of <1% was observed.
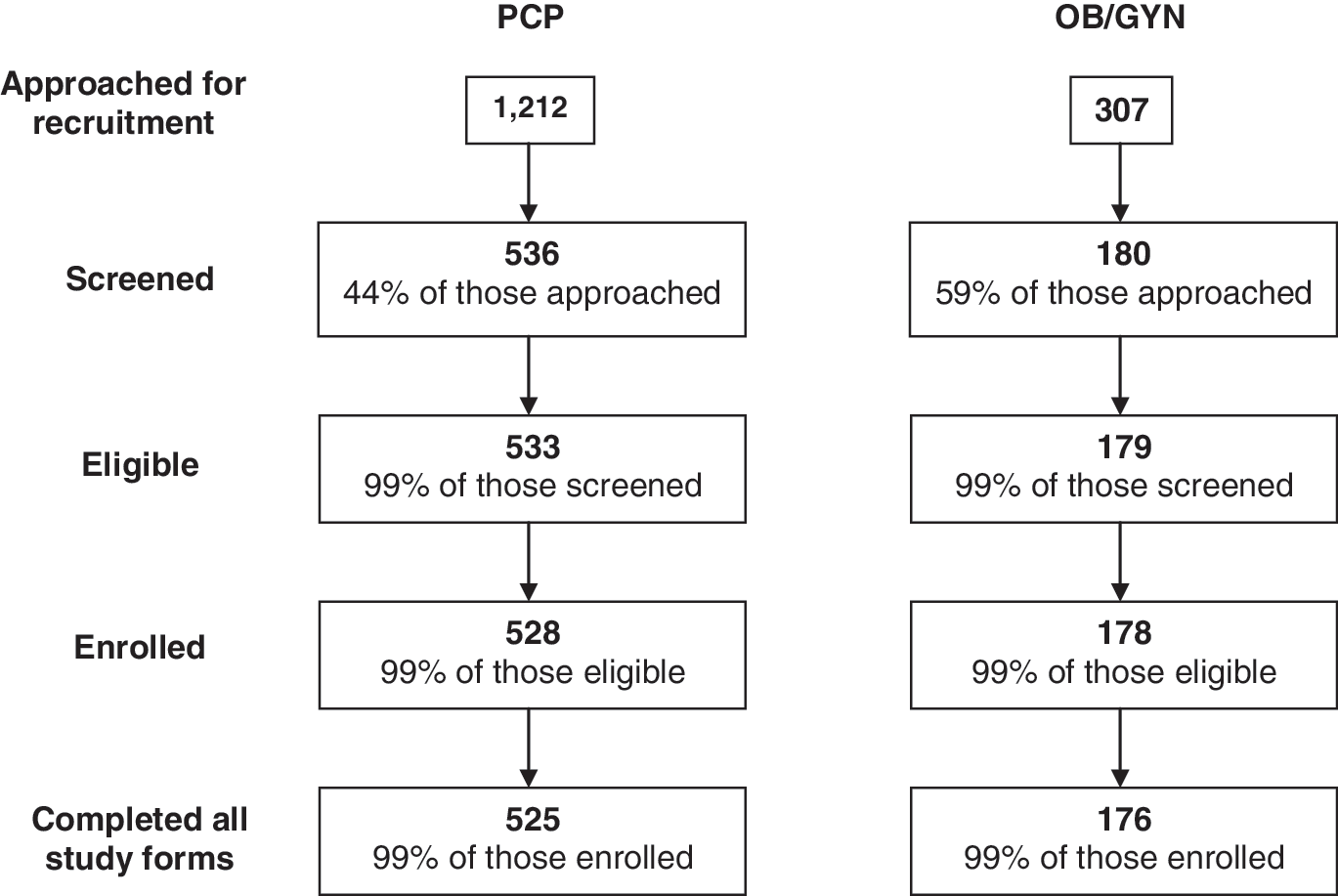
Subject recruitment, screening, and enrollment by clinic type. OB/GYN, obstetricians/gynecologists; PCP, primary care physicians.
The study sample was broadly representative of major geographic regions in the United States, with the largest number of participants being recruited in the West region (280) and fewest in the Midwest (122). Overall, however, more PCP and OB-GYN clinics were recruited from in the Northeast (7 sites) than in other U.S. Census regions. The participating clinics are listed in Table 2. Additional clinics had been identified in the remaining counties and Census regions at the time of study termination.
Enrollment was not complete at the time of study termination.
OB-GYN, obstetricians-gynecologists; PCP, primary care physicians.
Sample characteristics
A total of 701 women were enrolled at 20 clinical sites (10 PCP and 10 OB-GYN sites) across the United States. The study sample had a mean age overall of 46.2 years; 53.9% of the study sample were premenopausal, and 41.7% were postmenopausal. Among 701 women who completed the interview and questionnaire assessment, 52 women (7.4%) were assigned a diagnosis of HSDD, according to the DSDS criteria applied in the current study. There were no remarkable variations in HSDD status according to level of education or body mass index (BMI).
Women with HSDD diagnosis were also somewhat more likely to be married and white compared to women without HSDD (75.0% vs. 46.8% married, 96.2% vs. 81.6% white, respectively). Women with HSDD were more likely to be from the Northeast (38.5%) and to report being a current or past smoker (28.8%) compared to women without HSDD (18.8%). The most frequent comorbidities for women with or without HSDD included heart or cardiovascular disease, joint problems, and emotional distress. Consistent with the common comorbidities reported, the most frequent prescription medications used were cardiovascular, pain, and anxiety medications (Table 3).
Menopausal status was not able to be determined because of missing data.
BMI, body mass index; IUD, intrauterine device; SD, standard deviation.
Overall, the prevalence of HSDD in our sample was 7.4%, with a trend toward a higher prevalence in premenopausal compared to postmenopausal women (6.9% vs. 7.9%) and a slightly higher prevalence rate for women seen in an OB-GYN clinic (15 in 176, 8.5%) setting compared to a PCP setting (37 in 525, 7.0%).
HSDD diagnostic assessment
Of 701 women, 208 (29.7%) responded affirmatively to the four initial DSDS questions indicating presence of decreased or low desire with accompanying distress. However, only 52 (25%) of these women were classified by DSDS diagnostic interview criteria as fulfilling criteria for generalized, acquired HSDD. 19 Over half of the women (52.2%) reporting low desire with associated distress failed to qualify for the diagnosis because their lack of desire or distress was better accounted for by another medical or psychiatric condition (e.g., depression), side effects of a prescription or nonprescription drug, or secondary to the effects of stress or a relationship conflict. Of this group, 40.2% failed to receive a diagnosis of HSDD because of the presence of depression or another mental health problem. There were 16 women (19.5%) who reported multiple determining factors. Of these, 11 women reported the presence of depression among multiple factors, 8 women reported urologic/reproductive operations (i.e., hysterectomy), 8 women reported other medical conditions, and 5 women reported injuries or other surgeries as one of the factors contributing to their low desire (Table 4).
Multiple factors can include a combination of surgeries, depression, injuries, and others.
Figure 2 shows the prevalence by age decade of diagnosed HSDD, according to DSM-IV criteria, and the prevalence of low desire with distress as defined by a Yes response to the first four questions of the DSDS, without qualifying information concerning alternative causal factors. An increase in prevalence is observed in the 40–50-year-old and 50–60-year-old age groups, associated with the perimenopause and early postmenopausal phase for most women. The increased prevalence of HSDD during this period coincides with the increased number of women with symptoms of both decreased desire and distress in these age groups. The increases in both prevalence rates during this period are noteworthy.
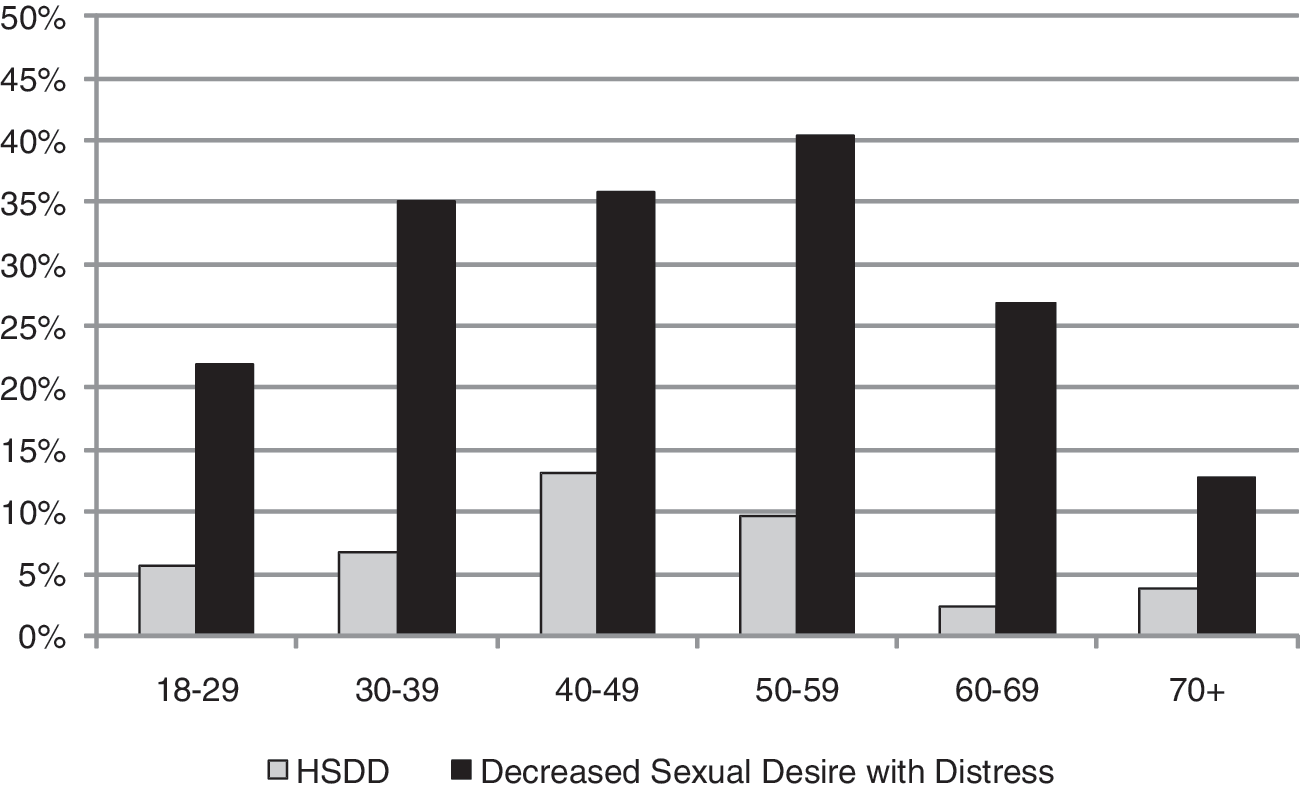
Prevalence of hypoactive sexual desire disorder (HSDD) and decreased sexual desire with distress by age decade. HSDD is defined as receiving a diagnosis of generalized, acquired HSDD by the diagnostic interview. Decreased Sexual Desire with Distress is defined as responding Yes to the first four questions of the Decreased Sexual Desire Screener© (DSDS).
Sexual function in women with HSDD
Overall FSFI scores were calculated for the 577 respondents who provided complete answers for all 19 questions of the FSFI questionnaire, 22 and FSFI domain and total scores were calculated separately using questionnaires with no missing data only. One of the questions in the satisfaction domain addresses satisfaction with sexual relationship. Women not in a partner relationship often skipped this question; therefore, the satisfaction domain had complete data for only 83.3% (584 of 701) of the participants.
As shown in Table 5, the FSFI total scores for women with HSDD who responded to all questionnaire items (83.3%) was 15.4±7.9 (mean±SD), compared to women with low sexual desire and distress, whose total FSFI score was 18.8±8.0. In contrast, women without low desire or sexually related distress had a mean FSFI score of 24.0±10.2, which is similar to the normal range cutoff point of 26.65. Higher scores on the FSFI equate to better sexual function. Women diagnosed with HSDD scored markedly lower on the total score (15.4±7.9) and had lower scores on specific domains or subscales of the FSFI, except for sexual pain.
Overall and domain-specific FSFI scores were calculated only if all components of the index or domain were answered, respectively.
Over half (55.8%) of the women diagnosed with HSDD reported feeling frequently or always bothered by low sexual desire on the FSDS-R (Question 13). 24 Conversely, <20% of women not diagnosed with HSDD reported feeling bothered by lack of desire for sex.
Treatment seeking in women with HSDD
Figure 3 presents our study findings for care seeking among women with diagnosed HSDD. Informal help-seeking activities were evaluated and included researching the topic (e.g., Internet browsing), reading articles in newspapers and magazines, talking with partners and friends, and similar activities. Among women diagnosed with HSDD, about one half (28 of 52) had sought formal treatment, typically from OB-GYN physicians, whereas about 40% (11 of 28) sought professional help specifically for their problem. Notably, however, only 28.6% (8 of 28) of women who sought formal treatment actually received treatment from their healthcare provider. The treatments received included prescription hormone injections, patches and creams (n=5), sildenafil (n=2), antidepressant medications (n=1), and herbal supplements (n=1). A small number (2 of 28) had received counseling or therapy for their HSDD problem.

Help seeking among women diagnosed with HSDD. Help-seeking groups (formal and informal) are neither mutually exclusive nor identical in composition. Women could contribute to more than one group, response option, or treatment type.
Discussion
This study was designed to extend our knowledge of the prevalence of HSDD by performing in-person diagnostic assessments by trained and certified interviewers using a validated method for determining HSDD status. 19 Moreover, we designed the study to assess the prevalence of HSDD and associated clinical characteristics of women in PCP and OB-GYN clinics in representative geographic locations. Although we were not able to complete recruitment for the study because of premature discontinuation by the sponsor, results obtained provided new data on the feasibility of clinic-based prevalence studies and resulting estimates of HSDD. Previous studies have shown that women can be successfully recruited in clinical settings for studies of reproductive and contraceptive needs, 20 and this method may be especially useful for assessing the prevalence of sexual function concerns in women who are attending care and potentially able to access formal professional assistance. This is the first study of this type to apply clinic-based recruitment and a structured, diagnostic interview method in a large, multicenter, study of generalized, acquired HSDD in women.
Given the busy office setting in which the study took place; in addition to the sensitive subject matter of the interview, we achieved an excellent response rate, particularly in the OB-GYN setting (response rate 59%). Although our rate of participation was <50% in the PCP practice setting, our completion rate in both settings once consent had been given was >99%. Similarly, clinical sites found study procedures to be acceptable, and none of the sites opted to discontinue participating once the interviews had begun. Many women commented on the interesting nature of the questions and interview format and high face validity and acceptability of the study to them. Additionally, the use of highly trained female interviewers may have increased participants' comfort level, and gift cards were provided to reimburse patients for travel and time of participation.
Based on the consistency of these observations across sites, it is unlikely that completion of the study would have affected our feasibility findings or response rates across the two types of clinic settings (PCP vs. OB-GYN). Based on our use of an in-person diagnostic evaluation by a highly trained research interviewer and rigorous exclusions of context-specific or DSM-IV differential diagnoses, we found an overall prevalence of generalized, acquired HSDD of 7.4%. This prevalence increased to approximately 12% of women in the midlife decade (40–49 years old) group who qualified for the diagnosis. A similar increase in this age group was observed by Shifren et al. 4 and Leiblum et al. 4,8 The finding in our study that most women who qualified for the diagnosis of HSDD were in a long-term partner relationship is consistent with similar findings in other population-based studies, 4,8 in addition to our recent HSDD Registry for Women. 14 A likely explanation for this finding is that women in long-term relationships are more likely to be distressed or bothered by their lack of desire, as well as concerned about the potential long-term impact of the problem on their partner relationship.
The overall prevalence rate of HSDD observed in our study (7.4%) is similar to the rate reported in the PRESIDE study (6.3%), after accounting for potential effects of depression or antidepressant drugs on self-reported loss of desire. Moreover, the age trend is nearly identical across the two studies. On the other hand, the 29.7% of women in our sample who reported symptoms of low desire and associated distress is higher than rates reported in PRESIDE and other community-based studies. 7,8,10,12 These differences in symptom reporting rates may be due to differences in the study populations (i.e., clinic-based vs. population-based samples) or increased sensitivity of the DSDS screening questions (Questions 1 through 4) to complaints of low desire and associated distress. On the other hand, the systematic exclusion of alternative diagnoses by in-person interviewing and use of rigorous differential diagnosis criteria based on DSM-IV in the current study resulted in comparable prevalence rates to those observed in PRESIDE, after accounting for effects of depression or antidepressant drugs. Depression, other medical and psychiatric conditions, side effects of a medication, stress, and relationship conflict may be primary causes of distressing low sexual desire, which should be carefully considered before a DSM-IV diagnosis is applied in either research or clinical care settings. Appropriate and effective therapeutic interventions require an accurate diagnosis, which may necessitate an evaluation by a skilled interviewer. Our results are descriptive and preliminary, given the early termination of the study as described.
Not surprisingly, our results confirm findings from previous studies showing large differences for sexual function scores of women with or without HSDD. The mean total FSFI score for HSDD cases (15.4±7.9) was approximately 11 points lower than the validated FSFI clinical cutoff of 26.5 for sexual dysfunction in a mixed group of women with HSDD and other sexual problems. 26 Furthermore, the mean FSFI score for HSDD participants overall is lower than norms observed in the original validation sample, which included women with Female Sexual Arousal Disorder (reported total FSFI score 19.2±6.6), 22 as well as a study of women with HSDD (reported total FSFI score 19.7±4.3). Sexual arousal scores were also markedly lower in women with HSDD, consistent with previous findings of the coexistence of arousal difficulties in women with HSDD. 7,10 Accordingly, proposals have been made by several authors to combine desire and arousal disorders in future diagnostic revisions. 15,16 Finally, the desire score for HSDD cases in the present study (3.0±1.3) was well below the recently established FSFI sexual desire clinical cutoff point of 5.0. 27
Conclusions
The DSDS administered in conjunction with a clinic-based, in-person history and diagnostic interview provides an accurate and replicable method for diagnosing HSDD. Despite premature discontinuation of the study by the sponsor, results obtained provided new data on the feasibility of clinic-based prevalence studies and resulting estimates of HSDD.
Footnotes
Acknowledgments
We gratefully acknowledge the contributions of Heather Cochran, M.A.T., Jennifer Yee, Blandyna Williams, and Max Krauthamer from New England Research Institutes, Inc., and Saeeduddin Ahmed, M.D., Michael Sand, Ph.D., M.P.H., and Robert Pyke, M.D., Ph.D., from Boehringer Ingelheim Pharmaceuticals, Inc. Funding for the study was provided by Boehringer Ingelheim Pharmaceuticals, Inc.
Disclosure Statement
R.C.R. is a consultant to Boehringer Ingelheim Pharmaceuticals, Inc., Palatin Technologies, and Johnson and Johnson. M.K.C., G.M., C.L., and L.R.G. have no conflicts of interest to declare. W.A.F. has served as a consultant and advisory board member for Boehringer Ingelheim Pharmaceuticals, Inc., Bayer, and Merck. J.L.S. is a consultant for New England Research Institutes, Inc., and has research support from Boehringer Ingelheim Pharmaceuticals, Inc. M.J.S. is an employee of Boehringer Ingelheim Pharmaceuticals, Inc.