
Abstract
Objectives:
Inadequate screening adherence for breast, cervical, and colorectal cancer among Latinas places them at greater risk for poor survival rates, once diagnosed. The purpose of this study was to examine two delivery methods of lay health educators (promotoras de salud) to increase screening behavior and evaluate costs.
Methods:
This community-based group randomized trial assigned Latinas due for breast, cervical, or colorectal cancer screening (n=1006) to promotora-taught cancer screening/prevention classes delivered individually (IND) or in social support groups (SSG) over 8 weeks. Screening behaviors were assessed immediately after and 3 and 15 months after intervention. Intervention costs per study arm were compared.
Results:
Screening and maintenance behaviors were not significantly different between SSG and IND for any one type of cancer screening, but with a study entry requirement that participants were either never screened or due for screening, postintervention screening rates (that is, completing a screening that was due) were notable (39.4% and 45.5%, respectively). The cost of achieving any one screening was much higher for IND participants.
Conclusions:
SSG vs. IND delivery did not significantly affect cancer screening behaviors, but both interventions produced robust achievement of screenings for previously nonadherent participants. Group-based promotora-led interventions supporting social involvement are recommended as a more cost-effective approach to achieving cancer screening among Latina women.
Introduction
Regardless of the well-known benefits of early cancer detection, there is still a lag in the rates of screening among poor and underserved populations. 1 –4 A proliferation of policies and programs to support access, adherence, and coverage of costs has only served, for the most part, to sustain the gap in screening.
Latinos experience the greatest disparity in use of preventive services of any group, 5 with especially poor use of colorectal cancer screening (among other prevention strategies, such as tobacco cessation advice and influenza vaccine) among those of Mexican and Central/South American descent. 6 Screening rates at the recommended intervals for colorectal, cervical, and breast cancer for Latina women were estimated to be 31.2%, 74.6%, and 41.7%, respectively, for the period 2009–2011, compared to non-Hispanic whites at 48.3%, 81.4%, and 53%, respectively. 7 In a recent review of breast cancer screening for women in the United States, disparities were strongest (lowest screening prevalence) for women aged 50–59 years (53.9%), Latinas (49.8%, taking into account a 2-year window), those with lower income (47.6%), and those with less than a high school education (46.1%). 8 Despite generally lower incidence rates than among other populations, this inadequate screening adherence for breast, cervical, and colorectal cancer among Latinas places them at greater risk for later stage detection and poor survival rates, once diagnosed. 7,9
There are many documented reasons for these disparities among Latinas, including lack of healthcare access and cost of healthcare (with markedly lower rates of insurance), language barriers for those who speak primarily Spanish, cultural norms that do not necessarily support breast or colorectal cancer screening (but that do support cervical cancer screening, such as the every-6-months recommendation that is established in Mexico, the birthplace of a large proportion of Latina women in the region 10 ), and practical barriers related to time and transportation. 7,11 –13
One of the strategies that has been used successfully to reach Latinos to promote preventive care, especially among low-income Latina women, is education delivered to the community by lay health educators, or promotora/es de salud. 10,13,14 Promotora/es are seen as providing language-matched and culturally relevant health education, are networked in their communities such that interventions can be built as participatory research, and have a deep understanding of how one might overcome logistical and psychosocial barriers to health behavior change. 15 –18 Practices characteristic of promotora/es that have been suggested to explain why they may be successful include the social support provided and the ability to tap into social networks to diffuse information in a community. 19 –22 Social support in group settings has further been proposed to be effective in supporting health behavior change (including cancer screening in underserved populations) by providing information, feedback, practical support, emotional processing of new behaviors, and building on cultural norms. 20,21,23,24
Although the evidence is accumulating for the effectiveness of promotora-type interventions in improving breast and cervical cancer screening among Latina women, even randomized controlled trials (RCT) generally do not test what aspects of such programs might make them more or less effective, 10,25 nor is there a standard of evaluating costs relative to the outcomes achieved. 26 In working through neighborhoods and community sites, promotoras sometimes work directly with individuals one-on-one and other times deliver classes in groups, ostensibly fostering social support. The Community Guide Task Force findings evaluating published research on community-based programs targeting individuals for cancer screening have shown mixed evidence for whether one-on-one or group education provides an advantage. There is currently a stronger evidence base for effectiveness of one-on-one approaches in promoting cancer screenings in general, with the exception of positive findings for group-delivered education for breast cancer screening. Even so, there is not enough information to recommend one approach over another. Many of the studies do not use the unique talents and community base of promotera/es or take into account efforts to build social support in the group setting. 27
Our study was designed to examine effectiveness and costs related to a particular design factor, group, or individual delivery mode of a promotora-led intervention to promote breast, cervical, and colorectal cancer screening and prevention behaviors among low-income Latina women. We hypothesized that a group intervention that encouraged support among class participants would more effectively increase screening behavior than a one-on-one format and would be less expensive. The social support aspects of the group-based intervention were expected to (1) provide cultural modeling of the intended behavior and (2) provide practical support, such as information or transportation sharing. Further, we proposed that the efficacy of maintenance behaviors (repeat screening when applicable) would be greater in a group-delivered intervention by (3) enhancing the continued discussion and support for screening behaviors beyond the time of the intervention than in the individual setting where continued social support would be less available.
Hypothesis One
Screening for breast, cervical, and colorectal cancer will be greater for those who receive a social support group (SSG) intervention than those who receive an individual (IND) intervention.
Hypothesis Two
Maintenance of screening for breast, cervical, colorectal cancer (i.e., repeat screening for procedures due each year) will be greater for those who receive an SSG intervention than those who receive an IND intervention.
Research Question One
Other than intervention conditions, what factors influence screening for breast, cervical, and colorectal cancer in a population of low-income Latina women?
Hypothesis Three
The cost per screening for breast, cervical, and colorectal cancer will be lower for those who receive an SSG intervention than those who receive an IND intervention.
Research Question Two
What is the cost of achieving cancer screening in this population?
Materials and Methods
Design
This study was a group-randomized community-based trial testing two methods of delivering a cancer screening and prevention curriculum taught by promotoras de salud. The primary outcome to be assessed was adherence to and subsequent maintenance of any one cancer screening modality for breast, cervical, or colorectal cancer for which a participant was due (that is, either having never been screened or past due for screening based on standard recommended periods per type of screening), with secondary analysis for cost.
Study population and site recruitment
The study was conducted in the Phoenix, Arizona, metropolitan area during 2004–2007 (with a prior year, 2003, devoted to curriculum development, establishing relationships with clinics for referral, and reviews of screening guidelines, cultural norms, and study design with a Hispanic Advisory Board [HAB]). Arizona's Latino population continues to grow, comprising approximately 24.2% statewide at the time of study initiation and rising to 31.8% at end of study. Sites identified as having a large proportion of low-income Latina women (targeting specific neighborhoods with resident families mostly below the poverty level) were approached for recruitment. Sites were identified through referrals from the HAB of lay and community-based leaders, friends, and networks of our promotora staff, fitting the community-based participatory research aspects of this study (described elsewhere 18 ).
Clusters of 4–10 sites, such as churches, schools, community centers, and apartment complexes, were recruited every few months, for a total of 144 sites over the time of the study. Site information was gathered, and then sites were block randomized (matched for similar characteristics, including type, size, ages of women attending, and language spoken) to either the IND or the SSG for each wave of intervention classes.
Study participant recruitment and consent
After an introductory presentation, women who were interested in joining the study were screened for eligibility. Women were eligible if they met the following inclusion criteria: self-identifying as Hispanic/Latina, aged≥18 (so as to include adult women or those potentially sexually active without asking a culturally uncomfortable question about sexual behaviors), and due for one or more of the breast, cervical, or colorectal cancer screenings for the appropriate age category, that is, out of compliance with the 2002 American Cancer Society (ACS) recommendations 28 for any one cancer screening, or not reporting being diagnosed with cancer other than nonmelanoma skin cancer. If interested and eligible, they were provided with informed consent and Health Insurance Portability and Privacy Act (HIPAA) information and invited to sign to indicate consent. Consented participants were interviewed for baseline data at this time, or scheduled at a later time before the beginning of the intervention.
Intervention
The intervention was delivered in six 80-minute sessions, with a 7th week scheduled for graduation for SSG or a visit for final questions with the promotora only for IND. Sessions for both the IND and SSG interventions were delivered primarily at the site where women were recruited, with occasional sessions being conducted in other sites, such as the participant's home, when makeup sessions or travel difficulties were encountered. Over the course of the study, a total of six promotoras taught across both arms of the study, randomly assigned to the groups/individuals to teach.
The training content and materials for the intervention had been developed in Spanish 18 and were reviewed by all investigators to update and check for accuracy. Topics included a definition and description of cancer; detailed information on dietary, tobacco, and physical activity recommendations for reducing risk for cancer; and screening for breast, cervical, and colorectal cancer, including screening procedures. A resource booklet (English and Spanish) that listed dozens of clinics or centers within several systems of care where one could obtain each type of screening according to type of healthcare coverage (or none) was presented and discussed to help guide each participant to the closest and least expensive options for screening. The National Cancer Institute's (NCI) Cancer Information Service toll-free number was included.
The content of this curriculum was then reviewed by the HAB for cultural, education-level, and community relatedness, and modifications were made based on this input. Once the content was finalized, enhancements were added to the curriculum manual to specifically promote group interaction, involvement, and interdependency for the SSG arm of the study, including how to organize a group and develop a sense of identity and commitment to the group (i.e., naming the group, encouraging women to meet each other's needs, and setting group goals). This interactive version of the curriculum included the same content as the IND but added such processes as group teaching exercises, discussion, and creative handouts that required interaction of participants. The final curriculum manuals (one with didactic teaching content for IND and one with the same content but enhanced with interactive processes for SSG) were written in Spanish and then translated to English.
Study measures and translation
Measures included demographics, cancer screening history, and a number of sociocultural variables (Table 1) collected in face-to-face interviews (time 1[T1], time 2[T2]) and via phone calls (T3, T4) with a bilingual (Spanish and English-speaking) staff member reading the questions and recording the answers. Each type of screening was assessed by providing the name of the test and a description in lay language and asking if and when was the last time (i.e., date) one obtained this type of test. Other measures are listed in Table 1. Traditionalism/modernism, rural vs. urban lifestyle preference, and acculturation scales (all factors shown to be related to a number of health behaviors in this population) had been developed and previously validated in Spanish. Perceptions of social support were examined using four dimensions suggested by House and Kahn 29 (instrumental, informational, appraisal, and emotional support) and one additional construct created for purposes of this study to directly query health-related aspects of support.
T1, baseline; T2, immediate postintervention; T3, 3 months postintervention; T4, 15 months postintervention to track screening maintenance.
FOBT, fecal occult blood test; R/U, rural vs. urban; SS, social support; T/M, traditionalism/modernism.
The social support scales and the remaining portions of the questionnaire were translated into Spanish and backtranslated to English. The full questionnaire in English and in Spanish was reviewed by the HAB, and minor adjustments were made to assure a comparable tool across both languages. Participants were asked to list closest friends/relatives, and lists were compared to assure that cross-contamination across sites was not likely to occur. Cost-related data were drawn from study implementation tracking records, budget reports, and personnel records.
Data analysis
Adherence to screening behavior was assessed through participant-reported dates of the screening test immediately (T2) and 3 months postintervention (T3) for the cancer screening for which a participant was due at T1. The sample used to define maintenance of cancer screening consisted of women who were adherent to cancer screening guidelines (by T3) and had a completed survey 15 months postintervention. If a woman obtained any one repeated cancer screening by T4 (15 months postintervention), she was considered to have maintained adherence. Comparison of baseline characteristics between the SSG and IND interventions was performed using chi-square tests and two sample independent t tests. For both the primary and secondary analysis, a test of proportions using the logistic function and taking into account the possible effect of clustering (due to randomization of sites) was used to determine if there is a difference in cancer screening behaviors between the SSG and IND interventions. Secondary analysis was conducted for the individual screening procedures (cervical, breast, and colorectal) and for age groups ≥18 and <40 years, ≥40 and <50 years, and ≥50 years for both the primary and secondary hypotheses.
Analysis relative to screening outcomes was carried out using statistical software Stata 10.0 (Stata Corp., College Station, TX). Scales for acculturation, traditionalism, rural preferences, reciprocal support, and the five social support subscales were assessed for internal consistency using Cronbach's alpha, suggesting adequate reliability: acculturation (0.73), traditionalism (0.57), rural preferences (0.67), informational support (0.86), instrumental support (0.77), appraisal support (0.81), emotional support (0.85), health-related support (0.83), and two reciprocal support factors, active support (0.89) and caring support (0.67). Additional analyses assessed the relationships among screening for any one cancer and demographic, health service access, and psychosocial factors using logistic regression analysis. A model including all potential predictors was first estimated. Then, backwards elimination was used to remove factors that were not statistically related to screening behavior.
The cost analysis was performed from the perspective of a future organization offering this type of intervention and provides the level of cost detail needed for such an organization's budgeting. Costs in each cost category were noted separately and reported on a cost per participant and cost per participant screened basis in year 2006 dollars. Costs incurred in other years were adjusted to 2006 costs using the consumer price index. 36 Promotora time was separately allocated to recruitment and the time incurred for each class session. Transportation costs for the promotoras were calculated based on the round trip distance between the main program office and the class site, using the 2006 standard mileage rate of $0.445 per mile. 37 Materials costs were split between durable goods (items that could be used for a number of classes) and consumable goods (items that were given to participants at each class) and represent the actual costs incurred. The cost estimates for durable goods assumed that each item had a useful life of 100 class sessions (a conservative estimate based on electronics obsolescence and model durability) before it had to be replaced, and these costs were allocated to each group based on the percent of useful life used.
Results
Study sample
The eligibility survey and baseline survey was administered to 2038 and 1036 participants, respectively (Fig. 1); 1006 participants were determined to be eligible for the study, including meeting the requirement of being due for any one type of cancer screening. Of these, 604 participants were from sites randomized to SSG, and 402 participants were from sites randomized to IND. Estimates of group size before site matching for randomization were similar across both arms of the study, but sites randomized to IND produced fewer volunteers for eligibility screening than for those in SSG. Of the 1006 eligible participants, 509 participants were reached for data collection postintervention (T2) or by the 3 months postintervention time point (T3)(49.4% attrition rate). Age, acculturation, having a regular primary care provider, and level of education were assessed for equivalence between the 509 remaining participants and those who dropped out or were lost before T2 evaluation. No significant differences were found on these characteristics between the evaluable participants and those not continuing after baseline data were collected (data not shown); only the 509 evaluable participants were included in further analyses. Of these 509 remaining, 475 participants had been due for cervical cancer screening (all were aged ≥18), 148 were due for breast cancer screening (all aged ≥40), and 75 were due for colorectal cancer screening (all aged ≥50).
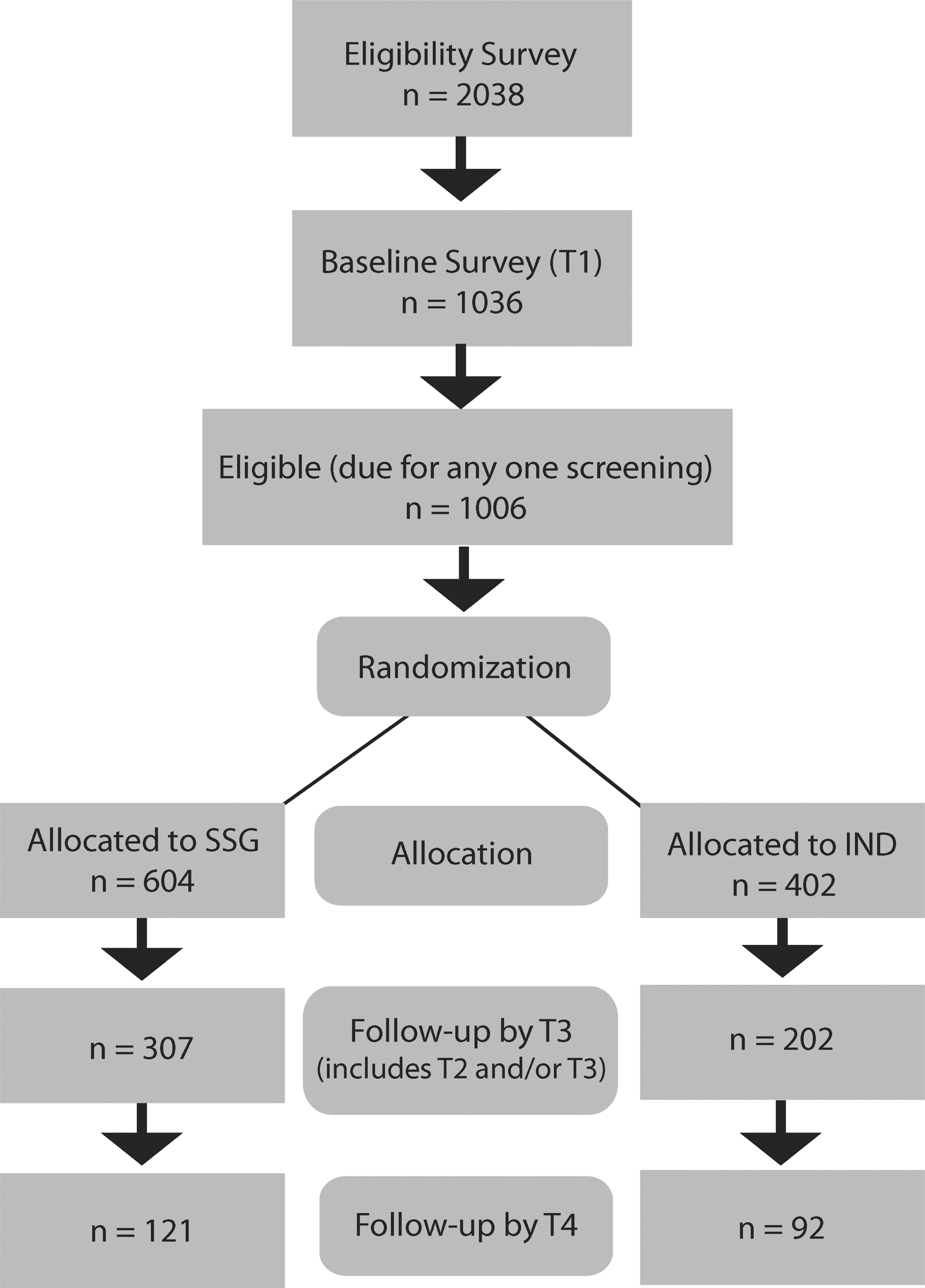
Recruitment and attrition flowchart. T1, baseline; T2, immediate postintervention; T3, 3 months postintervention; T4, 15 months postintervention to track screening maintenance; IND, individual; SSG, social support group.
Baseline characteristics were assessed for equivalence between SSG and IND groups; there were no significant differences between the two groups on the age distribution of the study participants, the type of cancer screening due at study entry, ever having a particular type of cancer screening at study entry, or any of the other demographic, acculturation, and social support factors shown in Table 2. Of the 509 participants available for evaluation, 213 (41.8%) were adherent to at least one cancer screening procedure for which they were due. Some were adherent to more than one test; 198 participants were adherent to a cervical cancer screening, 40 were adherent to a breast cancer screening, and 7 were adherent to colorectal cancer screening.
PCP, primary care physician.
Hypothesis One
The results of the primary hypothesis regarding intervention effects on any one screening (that is, counting any one screening obtained for individuals who are due for that screening type) and secondary analyses according to screening protocol and age categories are presented in Table 3. There was not a significant difference in screening behaviors among women in the SSG and IND intervention groups for any one type of cancer screening (primary hypothesis), although there was a fairly consistent trend toward higher rates of screening among those in the IND group. This was true even by cancer screening procedure and by the three different age categories.
Small sample sizes.
IND, individual; SSG, social support group.
Hypothesis Two
This hypothesis suggested that the SSG intervention would help support women past the time of the intervention to continue screening (i.e., screening behavior maintenance). This was tracked over the following year after the intervention and included only 213 participants who had been screened within the T2/T3 period so that follow-up on annual rescreening for that particular type of screening could be evaluated (i.e., all but endoscopy). The results for screening maintenance for each screening type and the different age categories are presented in Table 3. Once again, there does not appear to be a significant difference in maintaining adherence to cancer screening behaviors among women in IND and SSG intervention groups for any one type of cancer screening. This was true even by cancer screening procedure and by age categories, except among ≥50 year old women.
Exploratory analysis of group-level interaction
Given the lack of differences in rates of screening between the two interventions, an ad hoc analysis was conducted to examine participants' perceptions of social support and reciprocal support by the end of the classes to see if the manipulation of group-level social interaction and processes produced higher levels of social support in the groups than in the individual-level intervention. Means for these factors were quite high and similar across both groups (ranging from 4.32 to 4.61 on Likert-type response scales, where 5=strongly agree), although slightly higher scores for emotional, instrumental, and reciprocal support among the SSG participants (p=0.042, 0.034, and 0.009, respectively) indicate that there was a significant difference in perception of these social processes between groups.
Research Question One
Other than intervention conditions, what factors influence screening for breast, cervical, and colorectal cancer in a population of low-income Latina women?
Demographic and health services access factors potentially related to adherence were examined, including age, education, income, having a regular provider, and type of insurance (private, public, or none). Having a regular provider vs. not having a regular provider and decreasing age were associated with increased screening for any one cancer site (p=0.045 and 0.001, respectively). The additional psychosocial factors were examined in a full model of effects, including acculturation, traditionalism, rural values, social support factors, and reciprocal support. None of these factors showed statistically significant effects on screening behavior.
Hypothesis Three
The cost per screening for breast, cervical, and colorectal cancer will be lower for those who receive an SSG intervention than for those who receive an IND intervention.
Research Question Two
What is the cost of achieving cancer screening in this population?
Table 4 presents the cost analysis performed for each intervention. As can be seen, the cost to achieve one cancer screening in this population ranged from $263 to $517 in the SSG group and from $862 to $1716 in the IND group. Study records revealed that, on average, the promotoras spent about 2.5 hours on recruitment for each class series taught, including a meeting and presentation at each site and class participant registration. In addition, they spent a total of 3.5 hours for each class session taught (including preparation, reminder calls, travel, and class time). Average salary plus 20% benefits for the promotora staff was $15.49 per hour. Average number of participants per class (class size for SSG, number who received individual sessions for IND) was 6.7, and the average number of class sessions attended for the IND group was 5.0, with an average distance of 26.7 miles traveled. Total costs per participant were divided by the proportion of participants in each group screened (Table 3) to give costs per screening for each group. The SSG group used an average of 1.0% of the assumed 100-class session useful life per participant for durable goods, whereas the IND group used 5.0%. As can be seen in Table 4, the cost per participant and the cost per participant screened are more than three times higher in the IND group than in the SSG group.
Using the screening rates shown in Table 3 and assuming that all participants who started the program had the same rate of screening adherence as those who completed the program (and whose data are available at study end).
Using the screening rates shown in Table 3 for those who completed the program (n=307 in SSG and n=202 in IND) and assuming a zero screening rate for the other participants who started in each group.
Discussion
This community-based group RCT reached a large number of women from low-income neighborhoods with initial low rates of screening for breast and colorectal cancer but a stronger history of cervical cancer screening. In this study, we did not detect statistically significant differences in achievement of screening behavior between the interventions, one using a group setting to foster social support, the other delivered individually. With high attrition rates, it is possible that the results of “no significant difference between intervention groups” is more about selective retention (i.e., engaged individuals are more likely to stay in the study and get screened than those who have less interest, regardless of intervention strategy).
Both interventions were implemented by promotoras de salud, or women who were bilingual and bicultural and from the communities recruited. It is notable that staff members who were working as promotoras had anticipated from the beginning of the study that their individual-level intervention would work as well, if not better, than the group intervention. They had previous experience teaching in both conditions and suggested that the bond created between the teacher and participant was strong, particularly when one could build a personal relationship while promoting healthy behaviors. One of the important rules of the protocol was that once the intervention ended, the promotoras were expected to communicate that they would not continue to stay in touch and that the participant would meet with the interviewers to complete their time in the study. With that procedure, it was expected that IND participants would not have continued contact but that SSG participants might stay in touch with each other and continue to support healthy behavior, improving maintenance over time. Although the perceptions of some of the social support factors and reciprocal support were slightly (significantly) higher in the SSG intervention compared to IND, ratings were similar and generally high across both groups. In the end, these factors did not make a significant difference across the groups in screening behavior. Thus, the similarity of results may be due to similar effects for each intervention type or may be related to the lack of power because of high rates of attrition.
Regardless of this result, there is a notable finding across both groups for achievement of cancer screenings among participants who had previously been nonadherent to screening guidelines (i.e., not including colorectal cancer screening, participants achieved approximately 40% and 50% for screening adherence and maintenance, respectively). In populations where screening behavior is depressed (in particular, among those for whom obtaining screening in the past or keeping participants adherent to repeat screening has failed), production of any level of screening within a short period of time is an achievement. The screenings reported in our study show the number and percent of women who obtained screening only if unscreened (due) at the time of study entry (or, if screened, due again 12 months later for the annual screening modalities). When we examine those who were being assessed for screening (only those who were due at the time of enrollment), rates of screening in the range obtained are remarkable when considering that those followed for a type of screening had either never been screened or were nonadherent. For example, for mammography, only 18% of women aged >40 were up to date, and of those who were eligible to be evaluated for achieving mammography screening, 31.5% had never obtained one and 50.6% were due (late for screening). For cervical cancer screening, only 7.7% had never been screened and 13.5% were due. For both of these screenings, more than half of those eligible to enter the study had never been screened. These profiles of study entrants suggest that they may be more difficult than those typically adherent to move toward new or renewed screening behavior.
Research designed to reach people in community settings with cancer screening messages generally documents improvements in knowledge and intention, 38 but actual rates of screening are either not documented, based on self-report, or generally low (10%–20%), 39 –42 (with some exceptions for programs that use intensive combined interventions working within clinics for follow-up). 38 Our data are also based on self-report and far exceed what most of these community-only programs achieve. More importantly, the findings regarding cost suggest that community programs targeting groups may be not only as effective as one-on-one, time-consuming interventions but also cost substantially less to implement per person reached and per screening obtained.
Limitations
According to the original research proposal, the study was powered to detect an 8% difference in the main outcome with a total of 1600 participants with 800 participants in each study arm. There was substantial attrition in the study, with a final sample size of 509 for the primary hypothesis. This resulted in a sizable decrease in power and, thus, makes it more difficult to detect a difference between the interventions, if indeed there is one. There was a further decline in sample size for the secondary hypothesis, with a final sample of 213 participants adhering to cancer screening guidelines by 3 months postintervention, with 121 in the SSG arm and 92 in the IND arm. The reasons for attrition are largely unknown, with large numbers of women lost to follow-up without explanation (e.g., no-shows, calls not returned). The pattern of loss was characterized by no contact. We were unable to ascertain in most cases whether a woman was passively withdrawing or had moved away. The large attrition rates also compromise generalizability of the results, without knowing if there was a systematic pattern to the type of women who were lost that was not noted in the factors measured. Thus, even though comparisons of the percentages of screening obtained within each arm of the study suggest that the individually delivered intervention produces levels of screening adherence similar to the social support group intervention, the reduced power due to attrition leaves the question still open about which method may be more effective. Nevertheless, the more obvious conclusion may still hold, that bringing participants into a group session results in a substantially lower cost per screening than individual intervention formats.
A further limitation was that screening behavior assessment was based on self-report. These self-reported data were collected by phone, rather than face-to-face, at the third and fourth data collection points postintervention, possibly limiting the clarity of communication or the reliability of the answers. Our efforts to fully describe, remind, and prompt memory of screening, if obtained, and encourage participants to report actual behavior hopefully attenuated reporting based on lack of memory or social desirability effects. Nevertheless, the self-reported data pose a limitation to interpretation of study results.
Conclusions
Our study addresses the potential for a promotora-led educational intervention in community settings to achieve screening adherence for breast, cervical, and colorectal cancer, comparing two delivery modalities. The SSG intervention included the same essential curriculum elements as the IND intervention, with the addition of group processes designed to foster social support. Rates of screening adherence were not significantly different for the SSG and IND arms of the study; both arms of the study achieved a meaningful degree of screening adherence for participants who were either never screened or past due for screening. Although the rates of screening were consistently higher following the IND intervention than the SSG intervention, this difference did not reach statistical significance. This result may be due to the low power because of attrition, leaving the question about which type of intervention might be more effective for achieving screenings unanswered. What is most remarkable is the enormous difference in the costs between the two intervention modalities. When cost is the primary consideration, considering the much higher costs associated with the individual arm of the study, a group-delivered method of promoting cancer prevention in promotora-led community interventions is recommended.
Footnotes
Acknowledgments
We thank the promotoras de salud (Berta Carbajal, Lily Amaya Mar, Marlene Nunez, Norma Gonzalez, Telesfora Gonzalez) and interviewers for their contributions to all aspects of this project. The study was funded by the American Cancer Society, Juntos en la Salud: Cancer Prevention and Screening for Latinas TURSG-03-080-01-PBP.
Disclosure Statement
The authors have no conflicts of interest to report.