
Abstract
Objectives:
This study evaluated the healthcare resource use, work productivity loss, costs, and treatment patterns associated with newly diagnosed idiopathic heavy menstrual bleeding (HMB) using a large employer database.
Methods:
Medical and pharmacy claims (1998–2009) from 55 self-insured U.S. companies were analyzed. Women aged 18–52 years with ≥2 HMB claims (ICD-9 626.2, 627.0) and continuously enrolled for ≥6 months before the first claim were matched 1:1 with controls. Exclusion criteria were cancer, pregnancy, and infertility; HMB-related uterine conditions; endometrial ablation; hysterectomy; anticoagulant medications; and other known HMB causes. All-cause healthcare resource use and costs were compared between the HMB and control cohorts using statistical methods accounting for matched study design. Treatment patterns were examined for HMB subjects.
Results:
HMB and control cohorts (n=29,842 in both) were matched and balanced in baseline characteristics and costs. During follow-up, HMB subjects had significantly higher all-cause resource use than did control subjects: hospitalization incidence rate ratio (IRR)=2.70 (95% confidence interval [CI] 2.62-2.79); emergency room visits IRR=1.35 (95% CI 1.31-1.38); outpatient visits IRR=1.29 (95% CI 1.29-1.30). Average annualized all-cause costs were also higher for HMB subjects than controls (mean difference $2,607, p<0.001). Costs associated with HMB claims represented 50% ($1,313) of the all-cause cost difference. Of HMB subjects, 63.2% underwent surgical treatment as initial therapy.
Conclusions:
In this large matched-cohort study, an idiopathic diagnosis of HMB was associated with high rates of surgical intervention and increased healthcare resource use and costs.
Introduction
Heavy menstrual bleeding (HMB), also known as menorrhagia, 1,2 is a common health problem among women. Population-based studies worldwide have reported that approximately 10% of all women and 22% of women aged ≥35 years have HMB. 3 –6 The subjective indication of heavy periods correlates with increased menstrual blood loss for about 34% of women. 7
Management of HMB is multifaceted, and the choice of treatment depends on several factors, such as intensity of bleeding, pain, symptomatic anemia, desire for future fertility, health status, and concurrent medical conditions. 8 –10 Although many studies have published management algorithms for treating abnormal uterine bleeding (AUB), 11 –16 which includes HMB, less is known about real-world treatment patterns. Most recommendations call for initial medical management, typically with hormonal therapy in women of reproductive age, although evidence from randomized trials evaluating the effectiveness of most regimens is limited. 17 –19 Other medical treatments, such as nonsteroidal anti-inflammatory drugs (NSAIDs), antifibrinolytic agents (e.g., tranexamic acid), and cyclical progestins have also demonstrated limited effectiveness in reducing the blood loss in HMB. 20 –22 Unfortunately, side effects limit tolerance and acceptability of long-term oral drug treatment. Although failure of medical therapy is usually considered an indication for surgical interventions (e.g., hysterectomy, endometrial resection, or endometrial ablation), the preference for surgery treatment is not evidenced based. 23 The levonorgestrel-releasing intrauterine device (IUD) has also been shown to be an effective treatment comparable to endometrial ablation, 24 and randomized studies have shown lower costs when compared to hysterectomy for treatment of idiopathic HMB. 25
HMB adversely affects a woman's quality of life because of such symptoms as pain, fatigue, mood swings, and social embarrasment. 26 –28 Studies estimating resource use and costs associated with a strict definition of HMB without organic pathology have not been completed. However, past estimates suggest that HMB is associated with increased direct use of medical resources and that the treatment of HMB poses a sizable burden on the United States healthcare system. 29,30 Côté et al. 30 estimated the work loss costs in the United States in the late 1990s at $1,692 annually per woman. To update the cost estimates in the current healthcare system reflecting additional treatment options, we conducted a study that evaluated the treatment patterns, healthcare resource use, work productivity loss, and costs associated with newly diagnosed idiopathic HMB subjects from the perspective of an employer. According to the recent classification by Féderation Internationale de Gynecologie et d'Obstetrique (FIGO), the underlying patient population in the present study falls under AUB-N (not classified). 31 To reduce variability, this study focused only on idiopathic HMB, as the cost of treating HMB due to discrete causes (e.g., fibroid tumors or cancer) may depend on the cause itself and requires treatments different from those for idiopathic HMB.
Materials and Methods
Data source
The study sample was selected from a de-identified administrative private insurance database (Ingenix Employer Database) that included approximately 12 million beneficiaries (including employees, spouses, and dependents) from 55 large U.S.-based companies with claims for services provided in the years 1998–2009. The database includes information on demographics (e.g., age, gender), monthly health plan enrollment information, claims by types of services (e.g., hospitalization, emergency room [ER], outpatient), dates of services, diagnoses and procedure codes, and outpatient prescription drug claims. Diagnosis-specific claims were identified by International Classification of Diseases, 9th Revision (ICD-9) codes. Prescription drug claims were identified by National Drug Codes for oral medications and by the Healthcare Common Procedure Coding System (HCPCS) for nonoral medications. Short-term and long-term disability claims were available for employees of 27 companies, with dates of coverage and amounts paid to employees. Institutional review board approval was not required for this study.
Study design and study sample
A retrospective longitudinal matched-cohort design was employed (Fig. 1). The study sample consisted of female beneficiaries selected using the following inclusion criteria: (1) ≥2 claims with an HMB diagnosis (ICD-9 626.2—excessive or frequent menstruation; 627.0—premenopausal menorrhagia) within 6 months of each other, and (2) aged 18–52 years as of the date of first diagnosis of HMB (index date), and (3) ≥6 months of continuous insurance coverage before the index date. Exclusion criteria included (1) diagnosis of cancer except skin cancer, (2) pregnancy or infertility, (3) uterine condition (i.e., cervical dysplasia, complex or atypical endometrial hyperplasia, endometrial intraepithelial neoplasia) that may cause HMB anytime during the study period, and (4) procedure claim for endometrial ablation or hysterectomy before the index date. Women were also excluded if they had uterine fibroids, cervical or endometrial polyps, benign uterine neoplasm, simple endometrial hyperplasia, use of myomectomy or uterine arterial embolization, von Willebrand's disease or other bleeding disorders, or filled prescription(s) for anticoagulant medications up to 6 months before the index date. After these exclusions, we restricted the HMB cohort to subjects with idiopathic HMB diagnosis. Figure 2 presents the step-by-step disposition of the subjects during sample selection.

Study design. HMB, heavy menstrual bleeding.
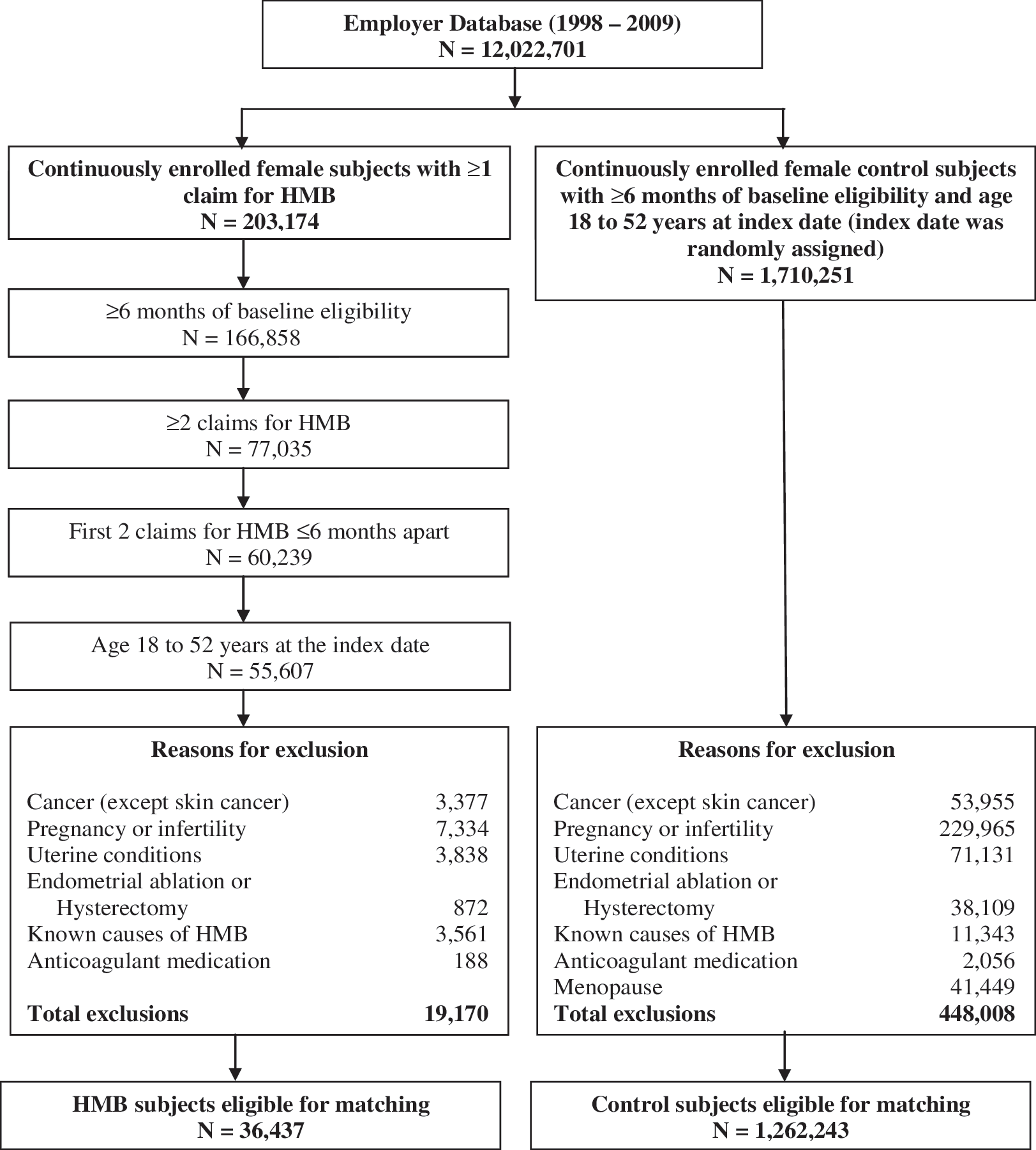
Subject disposition.
Controls were selected from continuously enrolled women without a diagnosis of HMB. Index date was randomly imputed for each control subject to ensure that the distribution of year of index date across cohorts was similar. With the exception of the HMB criteria, inclusion and exclusion criteria for controls were the same as for the HMB subjects. Additionally, control subjects were excluded if they had a diagnosis of menopause before the index date. The 6 months prior to the index date were used to assess baseline covariates for matching. Eligible HMB subjects were matched 1:1 with control subjects based on percentiles of propensity scores 32 and exact matching on the following factors: age groups, year of index date, region, disability coverage, Charlson Comorbidity Index (CCI), 33 dysmenorrhea, endometriosis, and medical and pharmacy cost categories. Each subject's observation period extended from the index date until the earliest date between health plan disenrollment, claim for menopause, or end of data availability (December 31, 2009).
Outcomes measures
Treatment patterns
For the HMB cohort, rates of treatment use and sequences of treatments were reported for the following medications: (1) combined hormonal contraceptives, including oral agents, vaginal ring, and contraceptive patch, (2) progestin-only oral agents, including contraceptive (e.g., norethindrone 0.35 mg) and noncontraceptive (e.g., medroxyprogesterone acetate) agents, (3) levonorgestrel-releasing intrauterine system (LNG-IUS), medroxyprogesterone acetate injection, and etonogestrel implant system, (4) uterine-preserving surgical procedures, including endometrial ablation and dilatation and curettage (D&C), and (5) hysterectomy.
Healthcare resource use
The frequency or rates of all-cause and HMB-related healthcare services were calculated as the number of services/events (i.e., unique visit days) divided by subject-years of observation. The following medical services were examined: hospitalizations, ER visits, and outpatient visits. HMB-related services were claims associated with a primary or secondary diagnosis of 626.2 or 627.0.
Direct medical and indirect work loss costs
The following annual costs were calculated: all-cause direct healthcare costs (hospitalizations, outpatient visits, ER visits, pharmacy prescriptions, and other services). Other services included claims for which the place of service was not listed as hospitalization, outpatient, ER, or pharmacy (e.g., nursing home). Costs for medical services associated with a primary or secondary diagnosis of 626.2 or 627.0 were considered as HMB-related costs, which were a subset of all-cause direct costs for the HMB cohort.
Indirect work productivity loss costs during the follow-up period included actual employer payments for disability days plus estimated costs for sick leave. It was assumed that each hospitalization accounted for a full day of work loss (8 hours), whereas an outpatient or ER visit accounted for a half-day of work loss (4 hours). The national median hourly wage from the Bureau of Labor Statistics was applied to calculate sick leave costs (total work loss hours*median hourly wage). Five-sevenths of the total sick leave hours were used in the calculation to account for weekend visits, which do not result in work loss costs. Disability claims contained a primary diagnosis code, disability start date, and disability end date. Wage data from individual companies were used to calculate disability costs. HMB-related disability costs were associated with a primary diagnosis of 626.0 or 627.0.
Costs were estimated based on the reimbursements from insurer/managed care plan to providers (employers' perspective). Subject copay or deductibles were not included in direct costs. Costs were inflation-adjusted to 2010 U.S. dollars based on the medical care component of the Consumer Price Index.
Statistical analysis
Descriptive statistics, including frequency counts and percentages, were used to summarize the categorical variables, and means and standard deviations (SD) were used for continuous variables. Statistical comparisons between the matched cohorts were conducted using McNemar's test or chi-square test for categorical variables with 2 and >2 categories, respectively, and paired t tests for continuous variables.
Incidence rate ratios (IRR), the ratios of the incidence rates for the HMB cohort divided by the incidence rates for the control cohort, were used to compare all-cause resource use. An IRR >1 corresponded to increased resource use for the HMB cohort; IRR <1 corresponded to decreased use. The IRRs were modeled using conditional Poisson regression models accounting for matched pairs. To assess statistical significance relative to the null value of 1 in IRR, 95% confidence intervals (CIs) were calculated based on the Poisson probability distribution to account for the person-time design.
Costs were compared through incremental costs. Incremental costs were calculated as the difference between the average annualized costs in the follow-up period of the HMB and control cohorts. Weighted average annualized costs were calculated to adjust for the various lengths of eligibility using the follow-up period of each patient as weight; therefore, the annualized per patient costs represent the mathematical equivalent of a standard per-patient-per-year value (i.e., aggregated costs divided by aggregated years, with both values summed across all patients). This approach produced a value for each patient, allowing for statistical testing. Because costs are often nonnormally distributed, we used nonparametric methods to assess statistical significance: a permutation test with 1,000 replications was used to test the statistical significance of incremental costs relative to the null value of 0.
All statistical analyses were performed using SAS release 9.2 (SAS Institute, Inc., Cary, NC).
Results
Baseline characteristics
Between 1998 and 2009, 29,842 women with HMB satisfied the selection criteria for this study and were matched with 29,842 women without a diagnosis HMB. The distribution of age groups, year of index date, region, insurance, disability coverage (24.2% of women in both cohorts), and medical history (dysmenorrhea and endometriosis) was equal across the cohorts (all p=1.000). Total baseline costs, based on 6 months before the index date, were also balanced between the HMB cohort ($1,489±3,549) and the control cohort ($1,502±3,816) (p=0.595) (Table 1).
Based on the 6 months before the index date.
Includes costs for prescription drugs, hospitalizations, outpatient services, ER services, and other services.
ER, emergency room; HMB, heavy menstrual bleeding; HMO, health maintenance organization; POS, point of service; PPO, preferred provider organization; SD, standard deviation.
Treatment patterns
Table 2 summarizes the treatment patterns in the HMB cohort (n=29,842). A little less than one third of the subjects (27.0%) received none of the treatments investigated in this study. Among those who received at least one treatment in the follow-up period (n=21,791), 53.8% (11,733 of 21,791) of subjects underwent uterine-preserving surgical procedures (including endometrial ablation and D&C), and 31.3% (6,831 of 21,791) of subjects underwent hysterectomy. About 13.6% of subjects received noncontraceptive progestin-only oral therapy anytime during the follow-up period. Uterine-preserving surgical procedures (44.6%) and combined hormonal contraceptives (19.2%) were the most common first treatments received after the HMB diagnosis. Among subjects who received at least two treatments (n=5,924), the top two treatment sequences were uterine-preserving surgical procedures followed by hysterectomy (18.5%) and progestin-only oral medications followed by uterine-preserving surgical procedures (16.0%).
Includes all treatments (medications or procedures) the patients received during the follow-up period. Percentages may not add up to 100.
Includes combined oral contraceptive, contraceptive vaginal ring, and contraceptive patch.
Includes levonorgestrel-releasing intrauterine system (IUS), medroxyprogesterone acetate injection, and etonogestrel implant system.
Calculated among the 5,924 patients who received at least two of the treatments listed.
Healthcare resource use
Table 3 presents the comparison of resource use in the follow-up period. HMB subjects had significantly higher annual all-cause resource use compared to controls: hospitalizations (IRR 2.70, 95% CI 2.62-2.79), ER visits (IRR 1.35, 95% CI 1.31-1.38), and outpatient visits (IRR 1.29, 95% CI 1.29-1.30). Approximately 12% of all-cause outpatient visits were HMB related (1.25 of 10.7).
Incidence rate has been calculated using the following patient-years of observation: 68,608 for the HMB cohort and 55,358 for the no-HMB cohort.
The top primary diagnoses for hospitalization in both cohorts were: HMB subjects (626.2—excessive or frequent menstruation, 14.6%, and 218.9—leiomyoma of the uterus, 11.0%); control subjects (786.50—chest pain, 1.2%, and 789.00—abdominal pain, unspecified site, 0.6%) (Table 4).
Costs
The average annual costs were significantly higher for the HMB subjects than for the control subjects ($6,439±8,682 vs. $3,832±8,308; difference=$2,607, p<0.001) (Table 5). Nearly 80% of women with HMB had higher average annual costs compared to their respective control women. Costs associated with HMB claims represented about 50% ($1,313) of the all-cause cost difference between the two cohorts. Outpatient costs accounted for the majority of the annual total costs in both cohorts: $3,249 (50.4%) for the HMB cohort and $1,725 (45.0%) for the control cohort. All-cause total work loss costs, including sick leave and disability costs, were also significantly higher for the HMB compared to the control subjects ($623±1,593 vs. $549±2,480; difference=$74, p<0.001).
There were 7,839 HMB women who had at least one claim with a diagnosis of anemia (ICD-9: 280.xx to 285.xx) any time during baseline or the follow-up period. The cost increase associated with HMB was slightly more pronounced for HMB women with anemia; the average annual all-cause costs for HMB subjects with anemia was $7,624±10,411, compared to $4,266±9,356 for controls (difference=$3,358, p<0.001). Similar findings were observed for HMB subjects without anemia (n=22,003) relative to controls (average annual all-cause costs: $5,918±7,745 vs. $3,660±7,848; difference=$2,258, p<0.001), highlighting the cost burden of HMB in women with or without anemia (data not shown, available upon request to the authors).
Discussion
HMB is a common condition among women of reproductive age, with a high prevalence rate of approximately 30%. 7 Despite its being a globally recognized problem, there is a dearth of information on the impact of HMB on the healthcare system. A handful of studies have reported healthcare costs, work loss costs, and resource use associated with AUB, which includes HMB. 5,29,30 To our knowledge, however, this is the first real-world study to evaluate the long-term burden of HMB on resource use, direct medical costs, and indirect work productivity loss costs relative to control subjects without a diagnosis of HMB using a national claims database of large employers. This article is also among the first to report treatment patterns observed in women with HMB receiving care in a large insurance claims database reflecting general clinical practice in the United States.
HMB is an expensive condition from an employer's perspective, given the high prevalence of the condition. In this large matched-cohort study with over 29,000 subjects in both case and control groups, we found that average annual all-cause resource use was significantly higher in subjects diagnosed with idiopathic HMB compared to subjects without a diagnosis of HMB. This increased use of healthcare services consisted of a comprehensive increase in the use of hospitalization, outpatient, and ER services. We also found that subjects diagnosed with HMB had significantly higher annual direct medical costs and indirect work loss costs compared to subjects who were not diagnosed with HMB. About 80% of women with HMB had higher average annual costs than control women without a diagnosis of HMB, underscoring that HMB is indeed an expensive condition from a payer's perspective. The overall cost difference was largely driven by HMB-related costs.
Uterine-preserving surgical procedures, including endometrial ablation, were the most common first-line treatment for subjects with HMB. This datum is in conflict with practice guidelines that recommend medical therapy as the first-line treatment. 17 –19 Although hormonal therapies were used by >30%, a sizable proportion of subjects with HMB did not receive either hormonal or surgical treatment. Our results may overestimate the proportion of subjects without treatment because we did not investigate the use of nonhormonal medications, such as NSAIDs or antifibrinolytic agents; however, tranexamic acid was not approved to treat HMB in the United States during the study period. These other treatments have demonstrated limited effectiveness and safety in clinical trials. 20 –22 Also, as 40% of our sample in both cohorts was from the Southern United States, the treatment proportions may reflect regional influences. Only a small proportion of subjects (<3%) received treatment with a LNG-IUS. This treatment is effective in reducing the blood flow in HMB and is associated with an improved quality of life. 34,35 It should be noted that LNG-IUS was not approved for treatment of HMB in the United States during the study period. 36
Our findings on resource use are generally in line with the few existing estimates. Studies have found that women who reported heavier menstrual blood loss were significantly more likely to visit a physician, receive ER care, and undergo a surgical procedure. 3,37 Côté et al. 5 estimated that women who have a heavier flow are at least 1.45 times as likely to use healthcare as are women who have a lighter or normal flow. Doherty et al. 38 reported that 63% of patients with menorrhagia were admitted to hospital at some stage for investigation and management of their symptoms. This study also found that subjects with HMB had a significantly higher annual rate of hospitalization compared to subjects without a diagnosis of HMB.
The current study showed that idiopathic HMB diagnosis was associated with increased direct and indirect costs. Half of the cost difference between the HMB and control cohorts was driven by HMB-related services. We found that 27.6% of all-cause annual hospitalization costs were related to HMB claims. Similar to our findings, Goodman 28 reported that 25% of all gynecologic surgeries involve a diagnosis of AUB and that 15% of all office visits are AUB related. Another study reported that >20% of all visits to obstetricians and gynecologists are because of AUB-related symptoms. 37 We also demonstrated that nearly 25% of all-cause annual outpatient costs were incurred in HMB-related visits.
The aforementioned published results cannot be directly compared to the findings from our study. First, the present study assessed the resource use and cost burden of HMB, whereas the cited studies evaluated the resource use and cost burden of AUB, which includes HMB. Second, whereas the cited studies reported the likelihood of increase in medical services associated with AUB, we quantified the annual impact of HMB on resource use. Also, the control groups selected in those studies may not be similar to the control group selected in this study. Nonetheless, our results are in the anticipated direction.
Prior estimates of work productivity loss costs in HMB are scant. Côté et al. 30 reported that work loss from increased blood flow is estimated to be $1,692 annually per woman. Our study estimated that women with HMB incur an average of $628 in total indirect costs over a 1-year period. These costs included sick leave costs and short-term and long-term disability costs. We most likely have underestimated the indirect costs because we had disability information from only half of the employers in the database. Moreover, as disability information was available only for employees, we were unable to capture the disability claims for spouses (of male employees) who had taken disability leave because of HMB. Nevertheless, this study is the first to show that HMB has significant economic implications for women in the workplace.
HMB is a known cause of iron deficiency anemia, 39 a condition that has been reported to be often untreated or inadequately treated in HMB patients. 40 We evaluated the costs among HMB subjects with anemia and without anemia. This study confirms that the presence of anemia along with HMB puts a significant financial burden on women. Further research is warranted to evaluate the costs of specific HMB subgroups that could help focus clinical attention.
There are some limitations to our study. As a result of the lack of clinical information in claims data, HMB and comorbidities were identified based solely on ICD-9 codes. Findings based on claims databases presume accurate assignment of billing diagnoses rather than confirmed diagnoses from direct examination of subject records. We relied on older definitions of HMB because of the lack of a formal HMB-specific ICD-9 code. The new FIGO classification was not available when the analysis for this study was conducted. 31 Subjects with a diagnosis of nonidiopathic (known) causes that accounted for HMB in the baseline period, such as fibroids, polyps, and coagulopathies, were excluded. 41,42 However, it is possible that subjects had a diagnosis of nonidiopathic causes of HMB (e.g., uterine fibroids) in the follow-up period. Also, because several common conditions (e.g., cervical dysplasia) that are infrequent causes of HMB were exclusions, some women with idiopathic HMB may have been excluded from the analysis. We did not examine the treatment patterns stratified by age, although we recognize that the initial treatment for HMB and the treatment path might be correlated with age at HMB diagnosis. Although the age was restricted at 18–52 years at index date in both cohorts, we did not control for the subjects' need for contraception, which may have accounted for some of the cost difference. The costs reported from the employers' perspective in this study may differ from those of other private or public insurers. Lastly, generalizability of results may be limited by sample selected for this study and insured subjects. Additional observational and clinical studies should be conducted to evaluate the real-world treatment patterns stratified by age groups accounting for the severity of HMB.
In summary, this large matched-cohort study conducted from an employer's perspective demonstrated that a diagnosis of idiopathic HMB is associated with significant resource use, direct medical, and indirect work loss cost burden.
Footnotes
Acknowledgments
Results from this study were presented as a poster at the 19th Annual Women's Health Congress, April 1–3, 2011, Washington, DC.
Disclosure Statement
This research was supported by Bayer HealthCare Pharmaceuticals, Wayne, New Jersey. J.T.J. has received payments for consulting and giving talks for Bayer, a company that may have a commercial interest in the results of this research and technology. This potential conflict of interest has been reviewed and managed by Oregon Health and Science University. The funding from Bayer was not contingent upon study results. Bayer participated in the study design, results interpretation, and manuscript review, as reflected in the authorship by Bayer employees, A.L. and J.P. P.L., F.L., S.P.S., and M.S.D. are employees of Analysis Group, Inc., which has received research funds from Bayer.