
Abstract
Background:
S-equol, a metabolite of the soy isoflavone daidzein, has been proposed as having potential for relief of menopausal symptoms. This study compared the efficacy of the natural S-equol supplement, SE5-OH, with isoflavones for relieving hot flashes and other menopausal symptoms.
Methods:
An 8-week randomized, double-blind, active comparator trial with SE5-OH was conducted in postmenopausal women (aged 45–65 years), who experienced ≥5 hot flashes/day. Participants (n=102) were assigned to one of four treatment groups: 10 (n=24), 20 (n=27), or 40 (n=25) mg S-equol/day or soy isoflavones (n=26). Participants recorded their hot flash frequency and rated their menopause symptom severity.
Results:
Reductions in hot flash frequency at week 8 were similar for all treatment groups. However, based on analyses of the cumulative effect for the 8-week period, 40 mg/day S-equol had a greater reduction of hot flash frequency compared to isoflavones (p=0.021). A subgroup analysis further indicated that for subjects with >8 hot flashes/day at baseline, 20 and 40 mg/day S-equol were superior to isoflavones in reducing hot flash frequency (p=0.045 and p=0.001, respectively). In addition, 10 and 20 mg/day S-equol improved muscle and joint pain score compared with isoflavones (p=0.003 and p=0.005, respectively).
Conclusions:
S-equol, 10 mg/day, appears to be as effective as soy isoflavones at reducing hot flash frequency and more effective for relieving muscle and joint pain in postmenopausal women. S-equol, ≥20 mg/day, alleviates hot flashes to a greater extent than soy isoflavones in those women who experience >8 hot flashes/day.
Introduction
Hot flashes are the most common vasomotor symptom associated with estrogen deficiency and are experienced by approximately 75% of North American women. 1,2 It is well known that hormone therapy (HT)—estrogen with or without a progestogen—is the most effective treatment for menopause-related vasomotor symptoms. 3 However, findings from the Women's Health Initiative (WHI) Trial 4,5 identified side effects of HT; therefore, physicians now assess each woman on an individual basis to determine the risk/benefit ratio of estrogen therapies. 3 As a result of these findings, many women are seeking natural alternatives to HT.
Recently, one of the principal metabolites of the soy isoflavone daidzein, S-equol, has been proposed as an alternative to estrogen therapy for the relief of vasomotor symptoms and as the active ingredient that mediates the effect of soy on vasomotor symptoms. 6 S-equol, which is formed from daidzein by intestinal flora, 7 –9 binds with greater affinity than its parent isoflavone to estrogen beta receptors. 10,11 Not all individuals have the ability to produce S-equol (i.e., not all are S-equol producers). Evidence indicates that 20%–30% of the adult population of Western countries are able to produce S-equol after consuming soy foods or soy isoflavone supplements compared to 50% of adults living in Asian countries. 12 The differences in equol-producing ability are attributed to variations in gut microflora. 13 The higher percentage of equol producers among Asian women combined with their high soy (daidzein) intake 14 may explain their lower prevalence of hot flashes compared to Western women. 15 A preliminary epidemiologic study of Japanese perimenopausal and postmenopausal women showed that urinary S-equol levels were significantly lower in women with more severe menopausal symptoms. 16 Several human studies have examined the potential for S-equol to relieve symptoms associated with menopause. 17 –19 The data from these studies demonstrate that SE5-OH, a natural supplement of S-equol, alleviates menopausal symptoms in perimenopausal and postmenopausal women.
Phytoestrogens, such as soy isoflavones, have been investigated for their ability to relieve menopausal symptoms. It is generally thought that the results of studies using soy supplements have been conflicting, but, a systematic review showed that in most double-blind placebo-controlled studies, using extracted or concentrated soy isoflavones significantly reduced vasomotor symptoms. 20 Thus, to date, there is a scientific consensus for mild vasomotor symptom relief with certain levels of soy isoflavone intake. 21
Because most Western women cannot produce S-equol, 12 S-equol supplementation may alleviate menopausal symptoms when used in place of isoflavones. Until now, no study has compared the efficacy of S-equol to that of soy isoflavones in relieving menopausal symptoms in postmenopausal American women. The objective of this small pilot study was to determine if S-equol has a comparable or superior effect to a standardized soy isoflavone extract for relieving menopausal symptoms. We compared the efficacy of S-equol, at dosages of 10, 20, or 40 mg/day, provided in the form of SE5-OH-containing tablets, with that of a standardized soy isoflavone extract at alleviating menopausal symptoms in postmenopausal women 45–65 years of age.
Materials and Methods
This study was a randomized, double-blind, parallel-arm study that included a 4-week screening phase and an 8-week intervention period conducted in 12 centers: Las Vegas, NV, St. Louis, MO, Pinellas Park, FL, San Antonio, TX, Chicago, IL, Scottsdale, AZ, Tucson, AZ, Cincinnati, OH, Edina, MN, West Palm Beach, FL, Akron, OH, and Columbus, OH. The protocol and amendments were approved by an Institutional Review Board for each center, and the International Conference on Harmonisation guidelines pertaining to Good Clinical Practices were followed. All study requirements and procedures were explained to each subject, and each subject provided written informed consent.
Subjects
Healthy postmenopausal women residing in the United States, 45–65 years of age, were recruited via radio, television, newspaper, and internet advertisements. Participating women were self-described as white, black/African American, Asian, and others. The majority of the subjects were non-Hispanic/Latino white. Subjects met the inclusion criteria if they experienced no menstrual periods within the past 12 months; their follicle-stimulating hormone (FSH) levels were ≥40 mlU/mL; they had a documented normal screening mammogram within the preceding 9 months; they experienced at least a mean of 5 hot flashes/day during the study's 4-week screening period; they were in good general health as determined by medical history, physical examination, electrocardiogram (ECG), serum chemistry, complete blood count (CBC), and urinalysis; and they were able to comply with all study requirements, in the opinion of the principal investigator (PI) at each center. Subjects were excluded from the study if they had a history of breast, ovarian, or uterine cancer; had evidence of endometrial hyperplasia (a bilayer endometrial thickness >5 mm) as determined by transvaginal uterine ultrasound (TVU); had a recent history of idiopathic vaginal bleeding; had a body mass index (BMI) ≥33 kg/m2; used within 90 days before screening HT, selective estrogen receptor modulators (SERMs), selective serotonin reuptake inhibitors (SSRIs), neurontin, clonidine, veralipride, or systemic antibiotic therapy; used within 30 days before screening over-the-counter (OTC) herbs, alternative therapies or dietary supplements, including soy, phytoestrogens, or black cohosh; regularly consumed within 14 days before screening foods and drinks containing soy, flax, or lignans as a major ingredient; were vegetarians; had a known allergy to soy or soy-based products; had a history of substance or alcohol abuse; were active smokers; had a concurrent or history of gastrointestinal condition, such as inflammatory bowel syndrome (IBS) or celiac disease or history of gastric bypass surgery; or had a clinically significant abnormality. Medications, supplements, and diets that could interfere with measurement of the health outcomes were prohibited during the study.
Study design
Eligible subjects underwent a 28-day screening period that was divided into four separate phases, each lasting 1 week. During the entire screening period, day −28 to day −1, subjects recorded in a diary the daily frequency and severity of hot flashes. During day −21 to day −15, subjects consumed one placebo tablet in the morning and one in the evening to assess the magnitude of the placebo response. Subjects were informed that they would all receive a placebo at some point during the trial, but the placebo period was not specified. Subjects who experienced at least a 30% reduction in hot flash frequency at the end of the placebo run-in period compared to the start of the screening period were considered placebo responders and were excluded from the study. To determine if each subject was an S-equol producer or nonproducer, during day −14 to day −8, subjects underwent a 4-day soy challenge test previously described by Setchell and Cole 12 that required consumption of seven 240-mL doses of commercially available soymilk (Silk®, WhiteWave Foods Company, Broomfield, CO). A spot urine sample was taken to determine equol producer status. The 4-day soy challenge was followed by a 3-day washout period. Data during day −7 to day −1 were used to confirm that each subject met the inclusion criteria and to establish the subject's baseline hot flash frequency. Of 559 women recruited, 102 met the eligibility requirements and were assigned to the treatment groups (Fig. 1A).
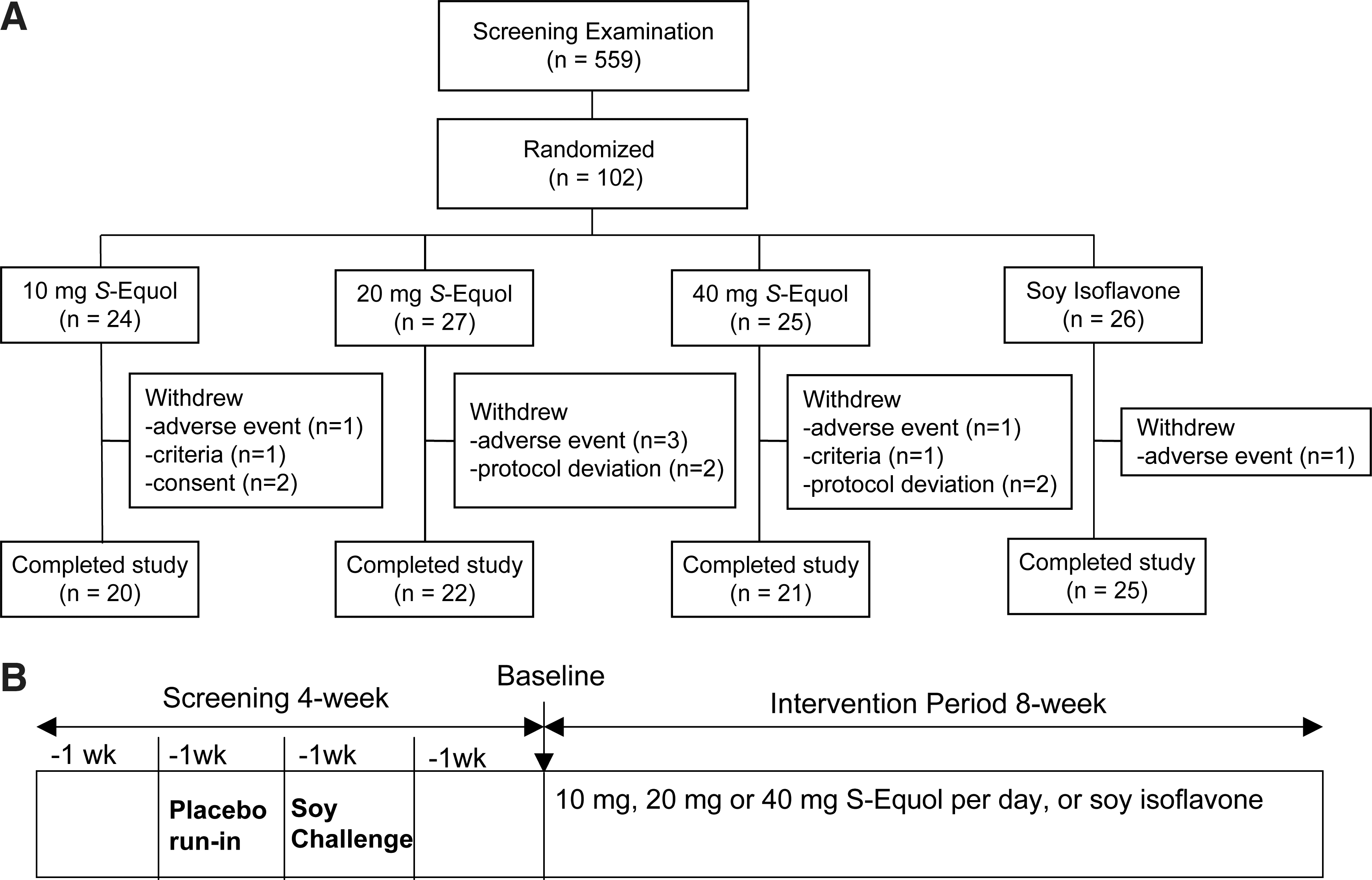
Because equol-producing status and BMI can affect outcome, the subjects were stratified based on equol producer status and BMI category (≤24, >24–<30, ≥30–<33). 16,22 Using a computer-generated randomization code, subjects were assigned to one of four intervention groups: 10 mg (n=24), 20 mg (n=27), or 40 mg (n=25) S-equol/day or standardized soy isoflavones (n=26). Both the subjects and the investigators were blinded to the group assignment (Fig. 1B). The lowest dose of S-equol used (10 mg) was based on preliminary studies investigating the relation between S-equol and menopausal symptoms, including hot flashes in Japanese women. 17,19 The higher doses were used to reflect the larger body mass in Western women and to establish a dose-response.
Supplements
The intervention products, SE5-OH containing S-equol and SoySelect® isoflavones, were supplied by Otsuka Pharmaceutical Co., Ltd. (Tokyo, Japan) and Indena S.p.A. (Milan, Italy), respectively. The tablets were manufactured by Pharmavite LLC (Northridge, CA). The SE5-OH tablets each contained 5.0 mg S-equol, 1.0 mg daidzein, 1.1 mg genistein, and 2.5 mg glycitein. SoySelect tablets contained 24 mg daidzein, 22 mg genistein, and 2.0 mg glycitein as aglycone equivalent. Placebo tablets contained lactose. SE5-OH and SoySelect tablets were all identical in appearance.
The intervention tablets were consumed twice per day for 8 weeks, four in the morning and four in the evening, for a total of eight tablets per day. The 10-mg, 20-mg, and 40-mg S-equol groups consumed two, four, or eight SE5-OH-containing tablets per day, respectively, divided over two doses and six, four, or no matching placebo tablets per day, respectively. The soy isoflavone active comparator was consumed as one morning oral dose of one SoySelect-containing tablet as recommended, plus three matching placebo tablets and one evening dose of four matching placebo tablets.
Subjects were provided a kit that included a 16-day (2-week plus 2-day) supply of tablets and returned to the study center biweekly to assess the number of unused tablets. Noncompliance for this study was defined as missing greater than five daily doses of the assigned intervention product during the treatment period.
Efficacy assessment
Throughout the 8-week intervention, subjects maintained a daily diary in which they recorded the frequency and severity of hot flashes and frequency of night sweats. At baseline, week 6 (data not shown), and week 8, subjects also completed the Greene Climacteric Scale (GCS). 23
The primary end point of interest was the mean change from baseline to week 8 in the daily frequency of hot flashes. Five secondary end points were stated to be of interest: hot flash severity, night sweat frequency, percentage of responders (defined as subjects with at least 50% reduction from baseline in hot flash frequency), total hot flash score (sum of each frequency×severity of hot flashes per day), and GCS subscale scores (Psychologic [Anxiety and Depression], Somatic, Vasomotor, and Sexuality).
Each subject was provided with a vasomotor symptom diary card on which they recorded daily the frequency of night sweats experienced the previous night and each hot flash they experienced that day. Hot flashes were rated as mild (sensation of heat without sweating), moderate (sensation of heat with sweating, able to continue activity), or severe (sensation of heat with sweating, causing cessation of activity), which corresponded to a score of 1, 2, or 3, respectively. The scores were tabulated weekly, and each subjects' average daily hot flash frequency and severity score was determined.
The GCS comprises 21 menopausal symptoms. Subjects were asked to rate the extent to which they were bothered by each of the 21 symptoms on a scale of 0–3, where 0 was not at all, 1 was a little, 2 was quite a bit, and 3 was extremely. Symptom ratings were then clustered into six subscales: Psychologic, Somatic, Vasomotor, Anxiety, Depression, and Sexuality. 23
Safety assessment
A complete medical history for each subject was taken at the initial screening visit and updated at the baseline visit. Throughout the study, subjects were clinically assessed by the PI at each center, all of whom were medical doctors trained in gynecologic medicine. Specifically, subjects were monitored for changes in various blood measures related to hematology, clinical chemistry, serum hormone levels (FSH, estradiol, thyroid-stimulating hormone [TSH], sex hormone-binding globulin [SHBG]), changes in urinalysis, vital signs, ECGs, screening mammograms, TVUs, and adverse events (AEs). The blood measurements, mammograms, and TVUs were conducted at baseline and at the end of the trial.
An AE was defined as any new medical problem or exacerbation of an existing problem experienced by a subject while enrolled in the study, whether or not it was considered treatment related by the investigator. A treatment emergent adverse event (TEAE) was defined as an AE that started after the start of supplementation; however, only those TEAEs for which a reasonable cause between treatment and the AE was related or possibly related were considered to be potentially supplement related. All TEAEs were coded by system organ class and the preferred term cited in The Medical Dictionary for Regulatory Activities. 24
Assessment of S-equol producer status
Spot urine samples were frozen at −80°C until analyzed by the Research Triangle Institute (Research Triangle Park, NC) using a validated proprietary method 25 for determination of total urinary daidzein and equol concentrations. In brief, aliquots (300 μL) of human urine calibration standards, quality control samples, and authentic samples were mixed with enzyme solution containing 1000 U/mL β-glucuronidase and 100 U/mL sulfatase in 1 M ammonium acetate pH 5.0 buffer. Samples were added to the internal standard, 4-hydroxybenzophenone. Quantitative analysis was performed using high performance liquid chromatography-tandem mass spectrometry detection (LC/MS/MS), with multiple reaction monitoring. Women whose urinary S-equol levels exceeded 50 ng/mL (0.21 nmol/mL) after the soy challenge were designated as equol producers in the study.
Statistical analysis
Demographic characteristics, including age, race, ethnicity, weight, height, BMI, and S-equol producer status were summarized using descriptive statistics (total number, mean, median, standard deviation [SD], maximum, minimum, and percentage as applicable).
Efficacy outcomes were analyzed using the observed case (OC) and last observation carried forward (LOCF) datasets, which were both derived from the intent-to-treat (ITT) model. The OC dataset consisted of actual recorded observations. In the LOCF dataset, missing data were imputed by carrying forward the subject's preceding nonmissing value except that a baseline value was not carried forward. The ITT dataset comprised data from all randomized subjects who had a baseline and at least one postbaseline assessed value, that is, the LOCF dataset. For the primary analysis, an analysis of covariance (ANCOVA) model for the change from baseline was applied to the LOCF dataset of the diary and GCS data, with treatment and S-equol producer status as main effects and baseline values as covariates. Differences between 20 mg and 40 mg S-equol doses vs. soy isoflavone were declared significant if both the overall F-test of the treatment effect of the ANCOVA and the t test of a contrast between S-equol doses and soy isoflavone were significant at the 0.05 level. With a statistical significance level of 0.05 set for both the F-test and the t test, the type I error in this procedure was also ≤0.05. A comparison of the primary efficacy variable between 10 mg S-equol and soy isoflavone was conducted by using a t test in a contrast statement of ANCOVA at the 0.05 level if both the 20 mg and 40 mg S-equol doses showed statistically significant differences compared to the soy isoflavone.
A post-hoc mixed model repeated measures (MMRM) analysis was used as an additional efficacy (sensitivity) test for daily hot flash frequency using the OC dataset. The dependent variable was the change from baseline in the mean daily hot flash frequency. The main independent variables were treatment, equol status, and baseline hot flashes. All outcomes were normally distributed.
The ANCOVA outcome analyzes the change in number or score of menopausal symptoms from baseline to week 8 and includes only women with week 8 data. The MMRM analysis includes all the repeated measurements, weekly average of the change from baseline, and eight repeated measures. The result of the MMRM analysis is an overall 8 weeks treatment effect. Regarding daily hot flash frequency, a subgroup analysis was conducted using baseline hot flash frequency, ≤8 or >8. The median frequency of hot flashes in this study was 8/day. Thus, a flash frequency of 8/day was chosen as the cutoff value between less severe and more severe number of hot flashes in this subgroup analysis.
Results
At baseline, there were no statistically significant differences among the four treatment groups in age, weight, height, BMI, race, ethnicity, and S-equol producer status (Table 1). Forty of the 102 women had detectable estradiol levels at baseline; the average was 22.6 pg/mL, and the range was 10–96 pg/mL. Eighty-eight of 102 (86%) women who began the study completed the study through to week 8. Data from these subjects formed the OC dataset. Because results of the efficacy analysis did not vary between the LOCF and OC datasets, only the OC dataset results are reported below. Fourteen of 102 subjects (14%) discontinued the study, 8 because of AEs, 4 for protocol violations, and 2 withdrew consent. After exclusion of subjects who dropped out by AEs, compliance was 94%. No subjects used antibiotics during the study.
There were no significant differences among or between groups by analysis of variance, (ANOVA).
BMI, body mass index; SD, standard deviation.
Menopausal symptoms
The average number of daily hot flashes in the entire study population was 10.0±4.03 (range 5–20 hot flashes/day). As indicated in Table 2, there were comparable reductions in each of the treatment groups in daily hot flash frequency, ranging from 3.09 to 3.66 hot flashes/day in the S-equol groups and 2.92 hot flashes/day in the isoflavone group.
Derived from analysis of covariance (ANCOVA) model, with terms of treatment, S-equol producer status, and baseline value as covariates. Corresponds to a comparison between S-equol (10, 20, or 40 mg) and soy isoflavone.
CFB, change from baseline; LS mean, least square mean (adjusted for effect of covariates); N/A, not applicable.
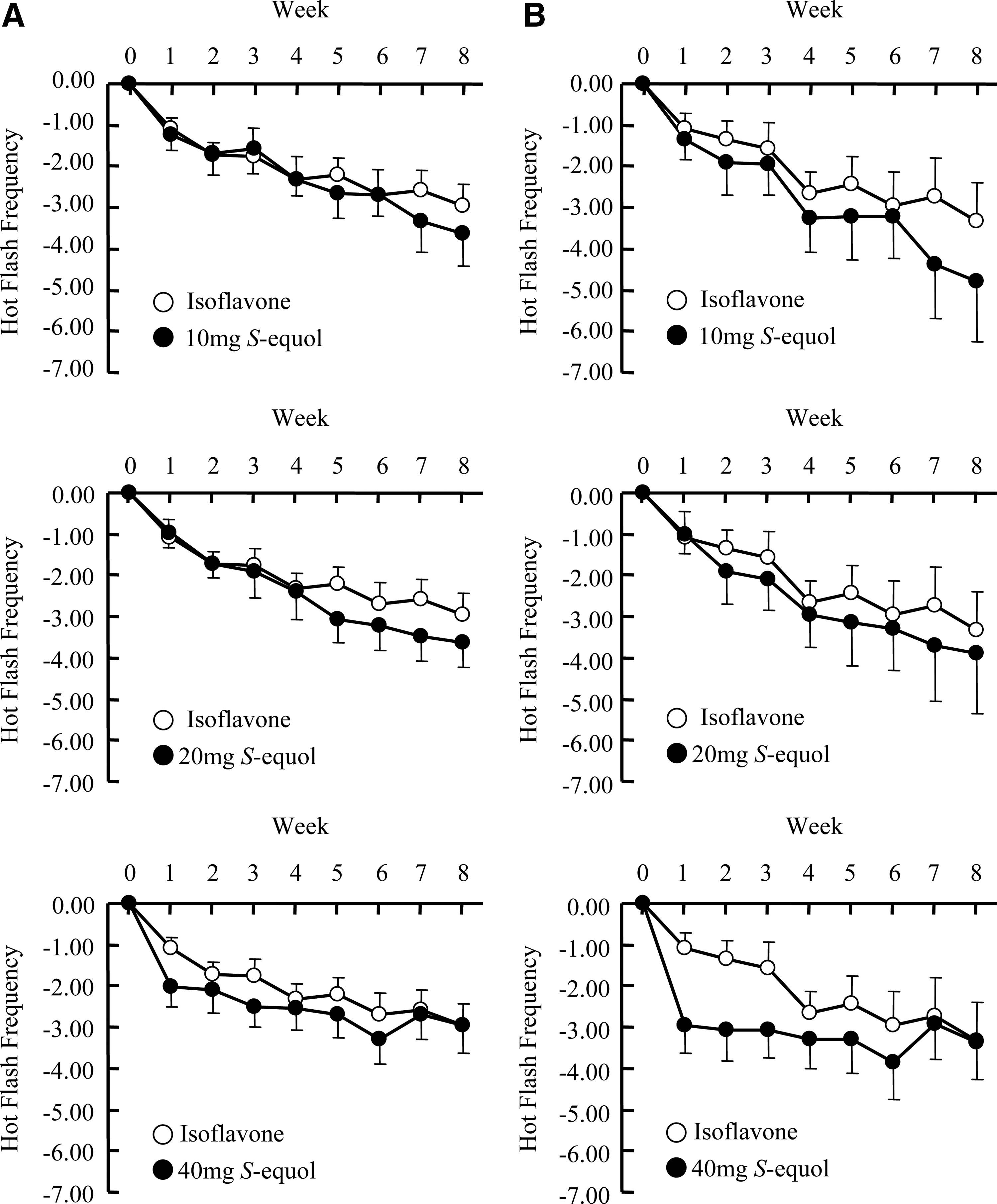
Figure 2A shows the change from baseline in mean daily hot flash frequency for each week over the treatment period for all subjects. For the 10-mg/day and 20-mg/day S-equol groups, the trend to superiority over the isoflavone group emerges after 4 weeks of treatment, whereas the apparent superiority of the 40-mg/day S-equol group emerges after 1 week but is no longer apparent by week 7. None of these differences were significant in the ANCOVA analysis. MMRM analysis also showed a comparable reduction in daily hot flashes with S-equol (2.30–2.71 hot flashes/day) to that observed with isoflavones (2.14 hot flashes/day). Further, the MMRM analysis demonstrated superiority for the 40-mg S-equol group (p=0.021), and the effect of the 20-mg S-equol group approached superiority (p=0.076).
Mean change from baseline in daily hot flash frequency, by week, for all subjects
After stratifying by baseline frequency of hot flashes (≤8 or >8/day), a comparison of treatment effects on mean daily hot flash frequency as determined over the entire 8-week treatment period by MMRM analyses showed superiority in subjects with >8 hot flashes at baseline. For this subgroup, the difference in reduction of daily hot flash frequency compared to isoflavone treatment of the 20-mg and 40-mg S-equol dosages was demonstrated (p=0.045 and p=0.001, respectively). The effect of 10 mg S-equol approached superiority at p=0.063 (Fig. 2B).
The percent of responders at week 8 (i.e., ≥50% reduction in hot flash frequency) is shown in Table 3. The percentage of responders in the 40-mg S-equol group was more than twice that in the isoflavone group (42.9% vs. 16.0%, p=0.056). The baseline severity of hot flashes was 2.22±0.5 in the 10-mg S-equol group, 2.16±0.3 in the 20-mg S-equol group, 2.22±0.4 in the 40-mg S-equol group, and 2.28±0.3 in the soy isoflavone group. There was no significant difference between any S-equol group and the isoflavone group. The baseline daily hot flash frequency was similar for all groups (Table 2), which may account for the lack of significant difference in the total hot flash severity (hot flash frequency per day×daily severity) between any S-equol group and the isoflavone group. There were no significant differences between any S-equol group and the isoflavone group in the change from baseline to week 8 in any of the GCS subscale scores, Psychological (Anxiety and Depression), Somatic, Vasomotor, or Sexuality.
Responders were defined as those who experienced ≥50% reduction in hot flash frequency from baseline.
Corresponds to a comparison between S-equol (10, 20, or 40 mg) and soy isoflavone using Fisher's exact test.
Other variables measured and analyzed in this study were the effects of treatment on each of the 21 menopausal symptoms measured by the GCS. Women who received 10 mg or 20 mg S-equol had a statistically significant improvement in symptom scores of muscle and joint pain (p=0.003 and p=0.005, respectively) vs. those receiving isoflavones (Table 4). For all other GCS symptoms, there were no statistically significant differences between any of the S-equol groups and the isoflavone group.
Derived from ANCOVA model, with terms of treatment, S-equol producer status, and baseline value as covariates. Corresponds to a comparison between S-equol (10, 20, or 40 mg) and soy isoflavone.
Adverse events
Overall, 48 of 102 subjects (47%) reported at least one TEAE. Nineteen subjects experienced at least one TEAE that was considered to be potentially supplement related: 8 (33%) with 10 mg S-equol, 5 (19%) with 20 mg S-equol, 4 (16%) with 40 mg S-equol, and 2 (8%) with isoflavone. TEAEs that occurred in >10% of subjects in any S-equol dose group were abdominal distention, 5 (15%) in the 20-mg S-equol group and 3 (13%) in the 10-mg S-equol group, and endometrial hypertrophy, 3 (13%) in the 10-mg S-equol group]. In the 40-mg S-equol and isoflavone groups, the same TEAE did not occur in more than 1 subject. TEAEs that related to the reproductive system or breast tissue, as detected by TVU or mammography, occurred in a total of 4 subjects. In addition to the 3 subjects described, a fourth subject in the 20-mg S-equol group developed breast cancer, which was considered by the PI to be unrelated to treatment.
Eight subjects withdrew from the study because of TEAEs: 2 were in the 10-mg S-equol group: endometrial hypertrophy (n=1); (7 mm in thickness with no other abnormal endometrial findings), abdominal pain (n=1); 4 in the 20-mg S-equol group: breast cancer (n=1), constipation (n=1), urinary tract infection (n=1), autonomic nervous system imbalance (n=1); 1 in the 40-mg S-equol group (depression); and 1 in the isoflavone group (positional vertigo). No notable or consistent changes in hematology, serum chemistry, urinalysis, hormone levels (FSH, TSH, SHBG), physical examinations, vital signs, or ECGs were observed for any of the treatment groups.
Discussion
The present study examined whether supplementation with S-equol has a comparable or more profound benefit than a standardized soy isoflavone preparation for relieving menopausal symptoms in postmenopausal American women. Effects of treatment on daily hot flash frequency for both the protocol-specified ANCOVA analysis and the post-hoc MMRM analysis showed that 10 mg/day S-equol achieved comparable reductions in daily hot flash frequency to the positive control soy isoflavone. The ANCOVA analysis demonstrated that all treatments achieved equivalent reductions in daily hot flash frequency at week 8. A post-hoc MMRM analysis demonstrated superiority of the 40-mg S-equol dose (p=0.021), and the 20-mg S-equol dose approached superiority (p=0.076). Because the ANCOVA analysis evaluates the change from baseline to week 8 and, by definition, includes only data for women with week 8 data, and the MMRM evaluates the overall 8-week treatment effect, it is not surprising that there is a difference in p values between the analyses. The trend toward superior effects of 40 mg S-equol compared to isoflavones in reducing hot flashes became apparent as early as week 1 and was sustained over several weeks (Fig. 2). Although it is not clear why the 40-mg S-equol group had different hot flash reduction dynamics, it might be clinically meaningful to administer 40 mg S-equol in the first few weeks and then decrease the dose to 20 mg or 10 mg S-equol after week 4.
A subgroup analysis indicated that for subjects with >8 hot flashes at baseline, S-equol approached or achieved superiority to isoflavones in reducing daily hot flash frequency, based on a post-hoc MMRM analysis (p=0.063, p=0.045, and p=0.001, for the 10, 20, and 40 mg/day groups, respectively). This was true even in the face of fewer subjects in the subgroup analysis. These data suggest that S-equol supplement might be useful for women who have a higher frequency of hot flashes.
Despite that all subjects had at least 12 months of amenorrhea and baseline FSH >40 mlU/mL, there was some variance in plasma estradiol levels. Several studies reported that estradiol levels did not differ between symptomatic and asymptomatic women, suggesting that consistent low estradiol levels are not an etiologic factor for induction of hot flashes. 26,27 We unexpectedly included a subject who had a high estradiol level, 96 pg/mL. However, baseline daily hot flash frequency and its deviation were similar across the groups (Table 2). Thus, although a high estradiol level might affect the results, it had little apparent effect in the groups studied.
No statistically significant differences among groups were observed for hot flash severity or any of the six subscales of the GCS questionnaire (Psychological, Somatic, Vasomotor, Anxiety, Depression, or Sexuality). However, post-hoc analyses of changes in each of the 21 GCS symptoms showed a statistically significant improvement at week 8 for muscle and joint pain in subjects receiving 10 mg (p=0.003) or 20 mg (p=0.005) S-equol compared to those taking isoflavones. No previous study has examined the effects of either isoflavones or S-equol on muscle and joint pain. Recent studies conducted with Japanese postmenopausal women showed that neck or shoulder muscle stiffness score improved in the 10-mg S-equol group compared with placebo. 17,18 Muscle stiffness and muscle pain can result from impaired local blood flow; thus, the ability of S-equol to induce endothelial nitric oxide synthase via the mitogen-activated protein kinase (MAP kinase) system exists as a possible mechanism by which S-equol reduces muscle and joint pain in this study. 28,29 Although isoflavones are also thought to affect vascular blood flow, 30 our results suggest S-equol's effects may be stronger than the effects of isoflavones.
SE5-OH is a fermented soy germ ingredient that contains in addition to S-equol, small amounts of daidzein, genistein, and glycitein. Data from animal studies 31 indicate that the primary active ingredient in SE5-OH for reduction of vasomotor symptoms is S-equol. Using ovariectomized rats, Yoneda et al. 31 compared the effects of SE5-OH (containing S-equol) with purified S-equol on hot flashes using tail skin temperature (TST) measures, a marker of hot flashes in rodents. They reported SE5-OH and purified S-equol similarly lowered TST compared to control. In animals receiving SE5-OH, TST was reduced by 68.9% (day 21) and 86.2% (day 28) (p=0.014 and p=0.020, respectively), and in animals receiving purified S-equol, TST was reduced by 60.1% (day 21) and 89.1% (day 28) (p=0.038 and p=0.016, respectively). The remarkably similar reductions in TST in animals treated with SE5-OH or purified S-equol strongly suggest that S-equol is the primary active ingredient of SE5-OH. Corroborating human evidence (a cross-sectional study) that supports the role of S-equol in alleviating menopausal symptoms was discussed earlier. 16 It is acknowledged that S-equol has estrogenic effects similar to those of isoflavones, which could explain the mechanism underlying their hot flash. 32 Furthermore, both present and previous 16 studies suggest that S-equol may more effectively manage menopausal symptoms than isoflavones. A recent publication by the North American Menopause Society addresses the possible superiority of S-equol over regular soy supplements. 21
Previous studies did not demonstrate a beneficial effect on vasomotor symptoms after intervention by soy 20 or a daidzein-rich supplement. 33 However, these studies did not determine if subjects were equol producers, which might account for the discrepancy between the previous and the present study. In the present study, approximately 30% of women were equol producers, which falls within the historical range of Western populations. 12 Understanding that S-equol can be a potent mediator of vasomotor response and that only a minority of Western women are equol producers, it would seem prudent for future studies on menopause-related outcomes to evaluate and stratify treatment groups on the basis of equol-producing status.
Standardized isoflavone extracts, but not soy foods or soy protein supplements, are widely considered to have some level of efficacy for alleviating vasomotor symptoms. 20 The decision to use an active comparator (SoySelect) in this study was based on findings published by Upmalis et al., 34 who conducted a large-scale 12-week intervention study on 177 postmenopausal women to investigate whether SoySelect, a standardized isoflavone extract, effectively alleviates hot flash frequency and severity. Because the study demonstrated statistically significant favorable effects of SoySelect compared to an inert placebo on reduction of hot flash frequency, it was of interest to assess the efficacy of SE5-OH compared to SoySelect.
Study limitations include the absence of an inert placebo arm and the small sample size. Strengths of the study are exclusion of placebo responders, stratification on the basis of identified S-equol producer status, the high rate of compliance, and use of free-living subjects. Because of its preliminary nature, the study length was designed to be 8 weeks to sufficiently detect a response. It is acknowledged that clinicians desire a length of ≥12 weeks to demonstrate the treatment's efficacy on vasomotor symptoms. As this study was designed to be an active comparator pilot study with a relatively small sample size, the statistical power was not strong enough to adjust for multiple comparisons or to demonstrate statistical significance of trends apparent in the intermediate time points. These results must be considered as preliminary and will require confirmation in a larger trial. Nevertheless, preliminary evidence on S-equol's effects in a North American population was derived that warrants future research in a larger-scale and longer study.
In a meta-analysis of 174 randomized controlled trials, Tempfer et al. 35 reported that phytoestrogen supplements have a safe side effect profile, with moderately elevated rates of gastrointestinal side effects. The overall incidence of side effects in 9,629 participants was 2,019 of 5,502 (36.7%) vs. 1,824 of 4,806 (38%) in the phytoestrogen and control groups, respectively. Specifically, the rates of hormone-related side effects, such as endometrial hyperplasia, endometrial cancer, and breast cancer, were not significantly different between groups. In this study, all TEAEs except one were mild to moderate in both the S-equol groups and the isoflavone group. In this small-scale, 8-week-long pilot study, 3 subjects in the 10 mg S-equol group developed endometrial hypertrophy, as did 1 subject and no subjects in the 20-mg and 40-mg S-equol groups, respectively. These data suggest that S-equol does not affect endometrial hypertrophy. The number of subjects who experienced gastrointestinal disorders was 7 in both the 10-mg and 20-mg S-equol groups, and 1 in the 40-mg S-equol groups and 2 in the isoflavone group. The naturally occurring dietary fiber in S-equol and lactose in the placebo tablets may have contributed to the gastrointestinal disorders.
Conclusions
To our knowledge, this is the first study demonstrating that supplementation with 10 mg/day of natural S-equol contained in SE5-OH in American postmenopausal women has comparable effects to soy isoflavones on reduction of hot flash frequency. This dose of S-equol appears to be more effective than soy isoflavones for relieving muscle and joint pain. Furthermore, ≥20 mg/day S-equol may be superior than soy isoflavones for alleviating hot flashes in women with >8 hot flashes/day. Findings from this study warrant further investigation in a larger placebo-controlled, statistically powered study.
Footnotes
Acknowledgments
We gratefully acknowledge Dr. Wulf Utian for providing useful advice, Drs. Ed Shneyvas (Pharmavite LLC) and Teresa Henry (Pharmavite) for their technical support, and Dr. Dusan Kostic (Otsuka Pharmaceutical Development & Commercialization [OPDC]), Dr. Sonia Shenoy (Pharmavite), Ms. Krista Martinko (OPDC), and Mr. Jerry Brisson (OPDC) for their guidance and input in the study. We also acknowledge Otsuka Pharmaceutical Co., Ltd., Japan for providing the SE5-OH and financial support.
Disclosure Statement
No competing financial interests exist.