
Abstract
Background:
Heavy menstrual bleeding (HMB) is the most common cause of iron deficiency anemia (IDA) in women. A novel, modified-release oral formulation of tranexamic acid (TA) designed to reduce gastrointestinal side effects was approved recently for treatment of HMB. We assessed improvements in objective laboratory measures of IDA in women with self-reported HMB who received long-term TA therapy.
Methods:
Women enrolled in a long-term, open-label, multicenter study self-medicated with TA 3.9 g/day administered as 1.3 g orally up to three times daily for 5 days/menstrual cycle for 27 cycles. Oral iron therapy was required if serum hemoglobin (Hgb) levels decreased to <11 g/dL.
Results:
A total of 723 women (mean age 38.3 years) were included in the intent-to-treat (ITT) population. Significant increases in mean serum Hgb and ferritin were observed throughout the study (p<0.01). Among 191 patients with low Hgb (<12 g/dL) at baseline, mean serum Hgb increased by ≥0.71 g/dL after the third cycle and all subsequent assessments (p<0.001). After 3 and 27 cycles, 34.1% and 45.7%, respectively, of patients with low Hgb at baseline shifted to within normal range, respectively. Among 233 patients with low ferritin (<10 ng/mL) at baseline, mean serum ferritin increased by >5.38 ng/mL after cycles 15 and 27. After 6 and 27 cycles, 35.2% and 58% of patients, respectively, with low ferritin levels at baseline shifted to within normal range.
Conclusions:
Long-term self-medication with this novel TA formulation improved Hgb and ferritin levels in women with self-reported HMB.
Introduction
Heavy menstrual bleeding (HMB), often defined as regular, normal intervals of menstruation with >80 mL of blood loss per menstrual cycle, 1,2 is the most common cause of iron deficiency in the developed world. 3,4 Iron deficiency anemia (IDA) has been detected in >25% of women with gynecologic conditions associated with heavy uterine bleeding. 5 Anemia resulting from HMB and the associated fatigue may negatively affect a woman's health-related quality of life. Anemia interferes with daily activities, has a negative impact on economic productivity and social well-being, and is associated with increased hospitalization costs, the probability of emergency room admission, and the likelihood of blood transfusion. 4,5
In Europe and other regions of the world, conventional oral, immediate-release tranexamic acid (TA) has been used for decades as a nonsurgical, nonhormonal treatment option for HMB. 6 Although conventional TA formulations have been generally well tolerated, they are associated with gastrointestinal side effects. 6,7 In clinical trials, diarrhea, abdominal pain, nausea, vomiting, and dyspepsia have been reported in 12% (3 g/day for 4 days for two cycles) 8 to 30% (4 g/day for 4 days for three cycles) 9 of patients receiving conventional TA. An oral, modified-release formulation of TA (Lysteda®, Ferring Pharmaceuticals Inc., Parsippany, NJ) is designed to reduce gastrointestinal side effects by controlling the dissolution of TA into the stomach. 10 This novel TA formulation was approved recently by the U.S. Food and Drug Administration (FDA) for treatment of cyclic HMB in patients in the United States. 11
Actual blood loss and anemia in women with HMB often do not correlate with the women's perception of blood loss. Nonetheless, TA has been shown to significantly decrease actual blood loss and significantly improve self-perceived menstrual blood loss. 12 A 2-year, open-label, multicenter study has demonstrated the safety of long-term treatment with TA 3.9 g/day and the potential for improved tolerability with its modified-release formulation. 13 To assess the potential for long-term TA therapy to decrease the burden of HMB as it relates to anemia, we analyzed serum hemoglobin (Hgb) and serum ferritin concentrations in women who were enrolled in the long-term safety study.
Materials and Methods
Study design and treatment
This was a long-term, open-label, multicenter study designed to assess the safety of a modified-release nonhormonal, oral formulation of TA in women with HMB. For inclusion in the study, patients were required to have a normal pelvic examination, cervical cytology (Papanicolaou test), or transvaginal ultrasonagraphy (TVU). If the pelvic examination was abnormal, a TVU was performed. If the TVU was abnormal, an endometrial biopsy was performed, and a normal endometrial biopsy was required for inclusion in the study. After a screening phase of one menstrual period, patients self-administered TA 3.9 g/day (1.3 g orally three times daily for up to 5 days) at the onset of HMB for a total of 27 menstrual cycles. Patients using medications to relieve HMB before screening were allowed to enter the study after a washout period of up to 8 weeks. Use of the following herbal remedies within 4 weeks before screening or during the study was not allowed: Capsella bursa pastoris (i.e., sheperd's purse), Agnus castus, Estroven PMS (i.e., chasteberry, Vitex, Cimicifuga racemosa), Symphytum officionale (i.e., Comfrey), and Angelica sinensis (i.e., Dong quai) Concomitant administration of pain medications (acetaminophen, aspirin, and nonsteroidal anti-inflammatory drugs) and vitamins were allowed to reflect the real-world setting in this long-term follow-up study. Initiation of oral iron therapy was permitted if Hgb levels were ≤12 g/dL at study enrollment, and therapy was required if levels decreased to <11 g/dL during the study. The study received Institutional Review Board approval annually at each site and was conducted in accordance with the Declaration of Helsinki, Good Clinical Practice, and applicable regulatory requirements. All study participants provided written informed consent.
Patients
A detailed description of patient inclusion criteria has been reported. 13 Briefly, women 18–49 years of age with a history of cyclic HMB were enrolled. Diagnosis of cyclic HMB was based on review of the patient's medical history, patients' self-reports of the impact menstrual bleeding had on their normal activities, findings on screening physical and gynecologic examinations, and results from laboratory testing. To be eligible, women had to have had at least 6 months of regularly occurring menstrual cycles (21–35 days apart), with menstrual periods lasting no more than 10 days. Women with clinically significant health abnormalities, including thromboembolic disease or coagulopathy, uncontrolled hypothyroidism (thyroid-stimulating hormone [TSH] ≥10 mU/L), severe anemia (Hgb <8 g/dL), thrombophilia, thalassemia, sickle cell disease, or any known bleeding disorder, were excluded from the study. Women of childbearing potential were required to use an acceptable method of birth control other than hormonal contraception.
Assessments
Blood samples for measurement of Hgb and ferritin were collected during selected study visits, which occurred 1–7 days after the last day of the menstrual period. Serum Hgb concentrations were measured at baseline and after treatment cycles 1, 3, 6, 15, and 27 (or at study termination). Serum ferritin concentrations were measured at baseline and after treatment cycles 6, 15, and 27 (or at study termination). Laboratory tests were performed by a central laboratory. 13
Statistics
Analyses were conducted on the intent-to-treat (ITT) population, which was defined as all study participants who received at least one dose of study drug. Descriptive statistics were used for quantitative laboratory test data. A subpopulation of patients with low baseline serum Hgb levels was defined as patients with baseline Hgb levels <12 g/dL. A subpopulation of patients with low baseline ferritin levels was defined as patients with baseline ferritin levels <10 ng/mL. The low baseline Hgb and ferritin subpopulations were further stratified based on whether patients received iron therapy. Frequency counts were compiled for classification of qualitative (categorical) variables and were used for prospective shift analyses to describe out-of-normal-range shifts of laboratory tests. A post hoc, exploratory analysis of normal-range shifts was performed on Hgb and ferritin level results using McNemar's test. All hypothesis testing was 2-sided with an α=0.05 level of significance. Statistical analyses were conducted using SAS Software, version 9.1.3 (SAS Institute, Cary, N C).
Results
Of the 784 women enrolled in the study, 723 were included in the ITT population (Table 1). The mean age was 38.3 years, and the mean duration of HMB was 9.8 years. At baseline, approximately one quarter of the patients had low (<12 g/dL) Hgb levels, and approximately 30% of the patients had low (<10 ng/mL) ferritin levels. Patients were exposed to TA during 10,213 menstrual cycles and were self-medicated with TA for a mean of 2.9 days/cycle at a mean dose of 3.8 g/day. A total of 239 patients remained in the study throughout all 27 on-treatment menstrual cycles. Failure to return was the predominant reason for withdrawal (156 women, 28.6%). Of the 545 patients who withdrew during this long-term study, 17.8% did so because of an adverse event. 13 However, the majority of these adverse events were considered definitely not, probably not, or possibly related to TA.
Percentage based on n=716 because of missing baseline values.
Percentage based on n=717 because of missing baseline values.
ITT, intent to treat; SD, standard deviation.
There was a trend toward a mean increase in Hgb and ferritin levels from baseline to study termination (Table 2). Significant increases in mean Hgb during TA treatment were observed after menstrual cycles 3, 6, and 15 compared with baseline. Significant increases in mean ferritin during TA treatment were also observed after menstrual cycles 15 and 27. The proportion of patients with normal/high Hgb or ferritin levels at baseline who reported low Hgb or ferritin concentrations at subsequent cycles remained at <10% throughout the study (data not shown).
716 used because of missing baseline values.
717 used because of missing baseline values.
Subpopulation
Because iron therapy was recommended for patients who experienced Hgb levels <12 g/dL and was mandatory for patients who experienced Hgb levels <11 g/dL, a more appropriate assessment of anemia measures in patients treated with TA is to evaluate the change from baseline of these measures among those patients with low Hgb or low ferritin levels at baseline. A total of 191 patients had baseline Hgb levels <12 g/dL and 233 patients had baseline ferritin levels <10 ng/mL (Table 3).
Hemoglobin levels
In contrast to the ITT population as a whole, a greater increase in mean Hgb levels was observed in patients with low Hgb levels at baseline. Mean serum Hgb in patients with low Hgb levels at baseline increased by ≥0.71 g/dL after cycle 3 and all subsequent postmenstrual cycle assessments compared with baseline (Table 3) (p<0.001 vs. baseline for each cycle). The proportion of patients with below-normal levels of Hgb at baseline who achieved normal Hgb levels increased with TA therapy throughout the study from 19.9% after 1 cycle to 45.7% after 27 cycles (Fig. 1A).
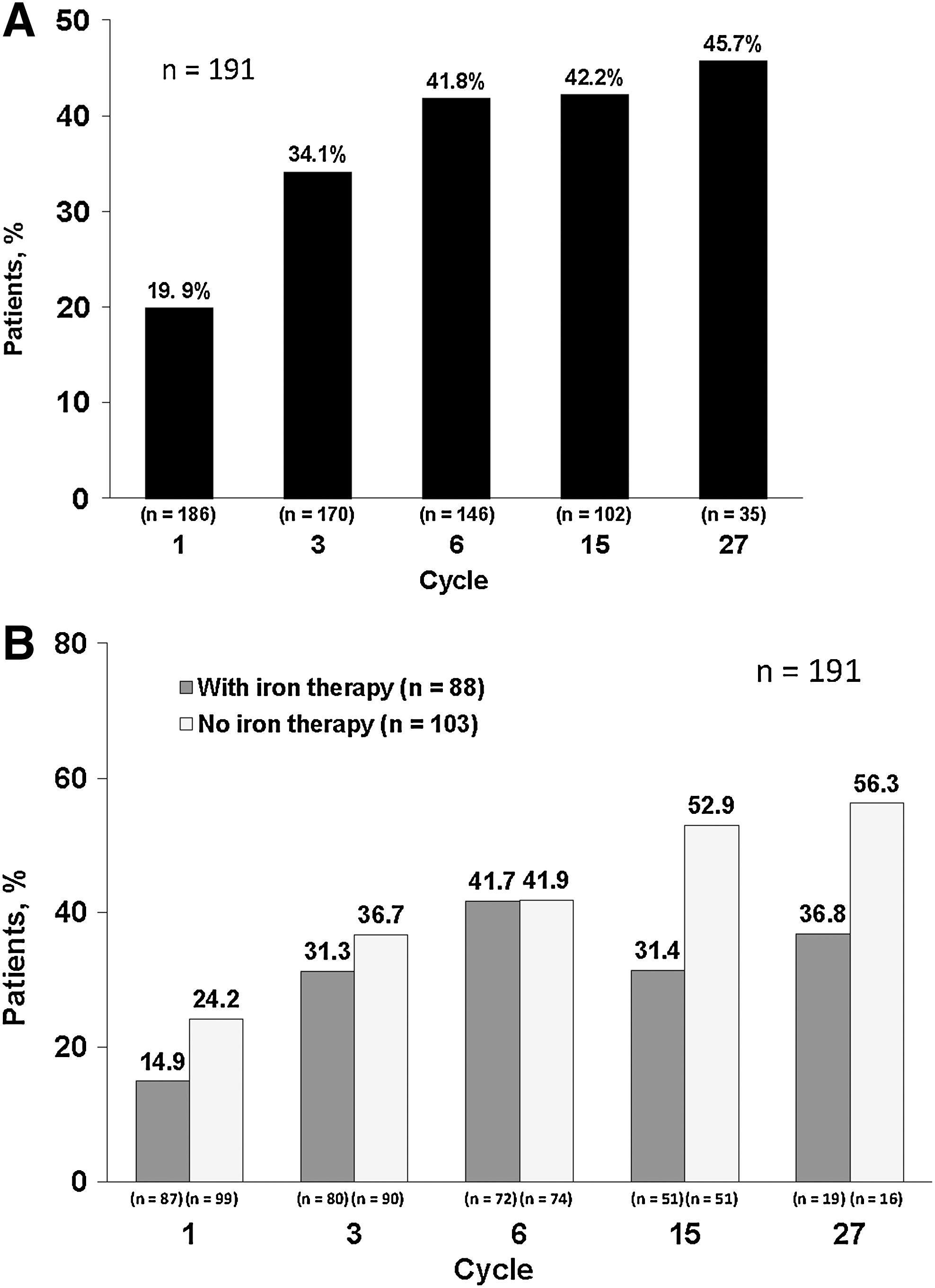
Percentage of patients shifting from below-normal serum concentrations of hemoglobin to within the normal range while being treated with a novel, modified-release oral formulation of tranexamic acid (TA) (Lysteda®, Ferring Pharmaceuticals Inc., Parsippany, NJ) 3.9 g/day, by cycle.
Among patients who did not receive concomitant iron therapy, the proportion of patients who shifted from below-normal levels at baseline to normal Hgb levels increased throughout the study from 24.2% after 1 cycle to 56.3% after 27 cycles (Fig. 1B). After cycles 15 and 27, the proportion of patients who had low Hgb levels at baseline and who achieved normal Hgb levels without iron therapy was markedly greater than the proportion of patients who received concomitant iron therapy.
Ferritin levels
Mean ferritin concentrations in patients with low ferritin levels at baseline increased from baseline after cycles 6, 15, and 27 (Table 3) (p≤0.001). The proportion of patients with below-normal levels of ferritin at baseline who achieved normal ferritin concentrations increased with TA therapy throughout the study from 35.2% after 6 cycles to 58% after 27 cycles (Fig. 2A). Among patients who did not receive concomitant iron therapy, the proportion of patients who shifted from below-normal levels at baseline to normal ferritin concentrations increased throughout the study from 33.6% after 6 cycles to 62.9% after 27 cycles (Fig. 2B). After cycle 27, the proportion of patients who had low ferritin levels at baseline who achieved normal ferritin levels without iron therapy was greater than the proportion of patients who received concomitant iron therapy.

Percentage of patients shifting from below-normal serum concentrations of ferritin to within the normal range while being treated with a novel, modified-release oral formulation of TA (Lysteda®) 3.9 g/day by cycle.
Discussion
Although often defined in clinical trials as menorrhagia >80 mL/cycle, HMB is difficult to objectively define in the clinical setting. Many women complaining of HMB have a much lower level of blood loss per cycle, 14 and women typically seek treatment for HMB based on a reduction or negative impact on daily activities rather than the actual volume of blood loss. 4,14 –16 Nonetheless, few studies have investigated treatment options for HMB in a patient population selected on the impact of menstrual bleeding on a woman's ability to engage in normal activities rather than an objective blood loss volume. In a long-term study, the safety and effect of TA on health-related quality of life were investigated in women with cyclic HMB. 13 Results from that report demonstrate that TA is well tolerated and is associated with noticeable and sustained improvements in health-related quality of life as assessed using the Ruta Menorrhagia Questionnaire, the Short Form 36 Health Survey Version 2.0, and the Menorrhagia Impact Questionnaire. 13 Herein, we reported on the effect of TA on measures of anemia in this patient population, which is more representative of the real-world clinical setting compared with other clinical trials using blood loss as an inclusion criterion. Our findings suggest that based on objective laboratory measurements of Hgb and ferritin concentrations, patients treated with TA will have less anemia, with improved oxygen-carrying capacity and iron storage.
Hgb is the most widely used measure to screen for anemia. Although some short-term studies have not shown improvements in Hgb levels with conventional TA after 4 to 5 cycles, 17,18 one uncontrolled usage study reported an increase in Hgb levels in women with HMB after receiving conventional TA for 3 cycles (from 11.54 g/dL to 12.60 g/dL). 19 In this long-term study, treatment with TA 3.9 g/day resulted in significant improvement in Hgb levels as early as cycle 3 (p<0.009). Compared with patients with normal Hgb levels at baseline, a greater increase in mean Hgb levels occurred among patients with low Hgb levels at baseline (mean increases >0.70 g/dL at cycle 3 through the remainder of the study). This finding was not unexpected because as prospectively specified, patients with baseline Hgb levels <12 g/dL could receive oral iron therapy. In addition, with time the patients with the lowest Hgb levels are expected to experience improved Hgb levels even in the absence of therapy. Nonetheless, patients with low Hgb levels at baseline shifted from low Hgb levels to the normal Hgb range; the proportion of these patients who shifted from low to normal Hgb levels increased with longer duration of TA therapy (Fig. 1B). The proportion of patients with low Hgb levels at baseline who achieved normal Hgb levels without concomitant oral iron therapy was markedly greater than that of patients who received iron therapy. This is likely because those patients who did not receive iron therapy had higher Hgb levels at baseline and, thus, required less improvement to reach the normal range. The proportion of patients with normal/high Hgb levels at baseline who maintained normal/high Hgb levels remained consistent throughout the study (i.e., patients with normal baseline Hgb levels generally did not worsen).
Although not specific, serum ferritin is the most sensitive laboratory test for detecting IDA. 20 Normal serum ferritin levels vary from laboratory to laboratory; however, 12–150 ng/mL is generally considered the normal range for women. 21 In this study, treatment with TA caused significant improvement in serum ferritin levels after cycle 15 and cycle 27 (p≤0.005). TA therapy significantly improved serum ferritin levels in patients with low ferritin levels at baseline after cycle 6 and through the remainder of the study, with a near doubling of serum ferritin levels after cycles 15 and 27 (mean increases >5 ng/mL, p<0.001). As shown with the Hgb measurements, patients with low ferritin concentrations at baseline who did not receive iron therapy shifted from low to normal ferritin levels at increasing proportions with longer duration of the study (Fig. 2B).
Conventional TA formulations have been associated with therapy-limiting gastrointestinal side effects. 6 –8,22 In this long-term safety study, TA was generally well tolerated, with just 1% of patients reporting a gastrointestinal side effect probably or definitely related to the modified-release TA formulation. 13
This long-term study is the first to report an improvement in Hgb and ferritin levels on treatment with a TA formulation in women without genetic bleeding disorders but who are suffering from HMB. As with many long-term studies, there was a discernible study withdrawal rate after 15 cycles. Nonetheless, during the study, the patients, with a mean duration of HMB of 9.8 years, self-medicated an average of 3 days per cycle (up to 5 days was allowed) and still experienced improvements in Hgb and ferritin levels. The long history of HMB in these women had a negative effect on their quality of life, which was shown to be improved with TA. 13 Although this study does not directly measure a correlation between quality of life and Hgb or ferritin levels, a recent study demonstrated a correlation between on-treatment Hgb concentrations with quality of life in women with HMB. 23
Conclusions
Treatment with TA improved Hgb and ferritin levels in women with HMB. During the study, a substantial proportion of women with below-normal levels of serum Hgb or ferritin at baseline experienced shifts to within normal ranges, regardless of their use of iron therapy. In addition, mean Hgb and ferritin concentrations significantly increased from baseline in the whole patient population and among patients with low Hgb or ferritin levels at baseline. TA was well tolerated during this long-term study. 13
Footnotes
Acknowledgments
We thank Ferring Pharmaceuticals Inc., for financial support for data analysis and manuscript development. We also thank Lamara D. Shrode, Ph.D., ISMPP Certified Medical Publication Professional™, of The JB Ashtin Group, Inc., who, on behalf of Ferring, developed the first draft of the manuscript based on an author-approved outline and assisted in implementing author revisions.
Disclosure Statement
K. M. has received research funding from Amgen, BioSante Pharmaceuticals, Wyeth, Xanodyne Pharmaceuticals, and Ferring Pharmaceuticals. R. G. M. has no disclosures to report. A. W. has received research funding from Pfizer, Graceway, Boehringer Ingelheim, BioSante Pharmaceuticals, Third Wave, Wyeth, GSK, Astellas, Depomed, Repros, Quatrx, Xanodyne Pharmaceuticals, and Ferring Pharmaceuticals. J. K. G. has received research funding from Pfizer, Organon, Ortho-McNeil, Wyeth, Galen Holdings, Warner Chilcott, Lilly, Sepracor, TAP, Barrier Therapeutics, Xanodyne Pharmaceuticals, Roche, BioSante Pharmaceuticals, Duramed, Berlex, Johnson & Johnson, Amgen, Perrigo Pharmaceuticals, Boehringer Ingelheim, Bayer, Teva, Schering-Plough, and Ferring Pharmaceuticals. T. L. A. is a full-time employee of Ferring Pharmaceuticals.