
Abstract
Background:
The optimal treatment of heavy menstrual bleeding (HMB) remains a challenge for the physician. There is a need for further trials to compare the effectiveness and compliance between a levonorgestrel-releasing intrauterine system (LNG-IUS) and minimally invasive types of hysterectomy, for example, laparoscopic supracervical hysterectomy (LSH), in women with HMB. This article is the first to report a randomized trial aimed at comparing postoperative outcomes and effects on quality of life after LNG-IUS or LSH in women with HMB.
Methods:
The trial was performed at Tor Vergata University Hospital, Rome. Seventy-two women requiring treatment for HMB were randomly allocated into two treatment arms: LNG-IUS (n=36) or LSH (n=36). The primary outcome was the comparison of the effects on menstrual bleeding (pictorial blood loss assessment chart [PBAC]) at 12 months after the two procedures. The secondary outcome measures were the quality of life, improvement in bleeding patterns, intensity of postoperative pain, and early postoperative complications. A p<0.05 was considered statistically significant.
Results:
The PBAC score was significantly reduced in both treatment groups. The Medical Outcomes Survey Short Form 36 (SF-36) score improved in both groups. A more significant improvement in the parameters Role and Mental health was observed after LNG-IUS.
Conclusions:
LNG-IUS can be considered as first option for the treatment of HMB unresponsive to drug therapy, and it is particularly suitable for women who want to preserve an acceptable menstrual flow. LSH may be considered the best surgical option in women with HMB unresponsive to any medical treatment.
Introduction
Heavy menstrual bleeding (HMB) is a widespread gynecologic problem that considerably impairs the well-being of many women. It can be defined as a blood loss of ≥80 mL per menstrual cycle. 1 However, discernment of heavy bleeding is extremely subjective. A simple semiquantitative measure for objectively assessing menstrual bleeding is the pictorial blood loss assessment chart (PBAC). 2 Although it has been used in many recent trials, the PBAC score has not been shown to be reliable. Essentially, women are treated based on their history, without quantitative blood loss measurements. Usually, surgical treatment of HMB is used when medical therapy is unsuccessful or ineffective. Although hysterectomy is more effective than other treatments in reducing menstrual blood loss, there are potential physical and emotional repercussions as well as social and financial costs.
The levonorgestrel-releasing intrauterine system (LNG-IUS) has been proposed for treatment of HMB as an alternative approach to surgery and has shown effective reduction of menstrual blood loss. 3 A Cochrane Systematic Review compared the efficacy and compliance among different therapeutic approaches in patients with HMB, concluding that LNG-IUS may be considered a similarly efficacious alternative to hysterectomy or endometrial ablation. 4 This therapeutic modality is not always totally successful, however, and a subsequent surgical treatment often is required.
There is a need in the literature, for further trials to compare the effectiveness and compliance of LNG-IUS and minimally invasive types of hysterectomy, such as laparoscopic supracervical hysterectomy (LSH), in women with HMB. Our randomized trial aimed to compare postoperative outcomes and effects on quality of life in a series of patients treated using LNG-IUS or LSH.
Materials and Methods
Patients
The trial was performed in the Section of Gynaecology, Department of Surgery, Tor Vergata University Hospital, Rome. From April 2008 to September 2010, all women with HMB unresponsive to medical treatment were considered eligible for the study. Inclusion criteria were (1) the presence of HMB, (2) reproductive age (aged 35–50 years), (3) completed family, (4) failed on appropriate first-line oral medical therapy, (5) normal Pap smear, (5) no pelvic pathology at ultrasound, (6) normal endometrial biopsy, and (7) PBAC ≥100 (average of two consecutive cycles). Exclusion criteria were (1) previous endometrial resection/ablation, (2) previous insertion of LNG-IUS, (3) any uterine pathology on scan or hysteroscopy, (4) any pathology where hysterectomy was indicated, (5) not fully investigated abnormal uterine bleeding, and (6) postmenopausal bleeding. The study was approved by the local ethics committee.
Of 100 women with HMB unresponsive to medical treatment, 82 fulfilled the inclusion criteria and were recruited for the trial; 10 refused to participate. A written informed consent was obtained from each patient before randomization. Enrollment was closed when 72 patients were included, and 36 patients were allocated to each group. The patients were randomized the day before the procedure (Fig. 1) based on a computer-generated list using serially numbered, opaque, sealed envelopes. Each patient was blindly allocated by a physician to LNG-IUS (n=36) or LSH (n=36). The sequence was concealed until interventions were assigned. Those who performed the procedures did not know which women undergoing the procedure had been included in the study. Those assessing the outcomes were blinded to the group assignments. All procedures were performed by the same surgeons using the same technique. Standard preoperative assessment was performed together with an abdominal and transvaginal ultrasound examination, a Pap smear, and an endometrial biopsy to exclude any pathology. Intraoperative prophylactic antibiotic therapy by cefazolin was administered to the LSH group. The patients were discharged from the hospital when they were tolerant of a normal diet, able to dress themselves, fully mobile, apyrexial, and not requiring analgesics.
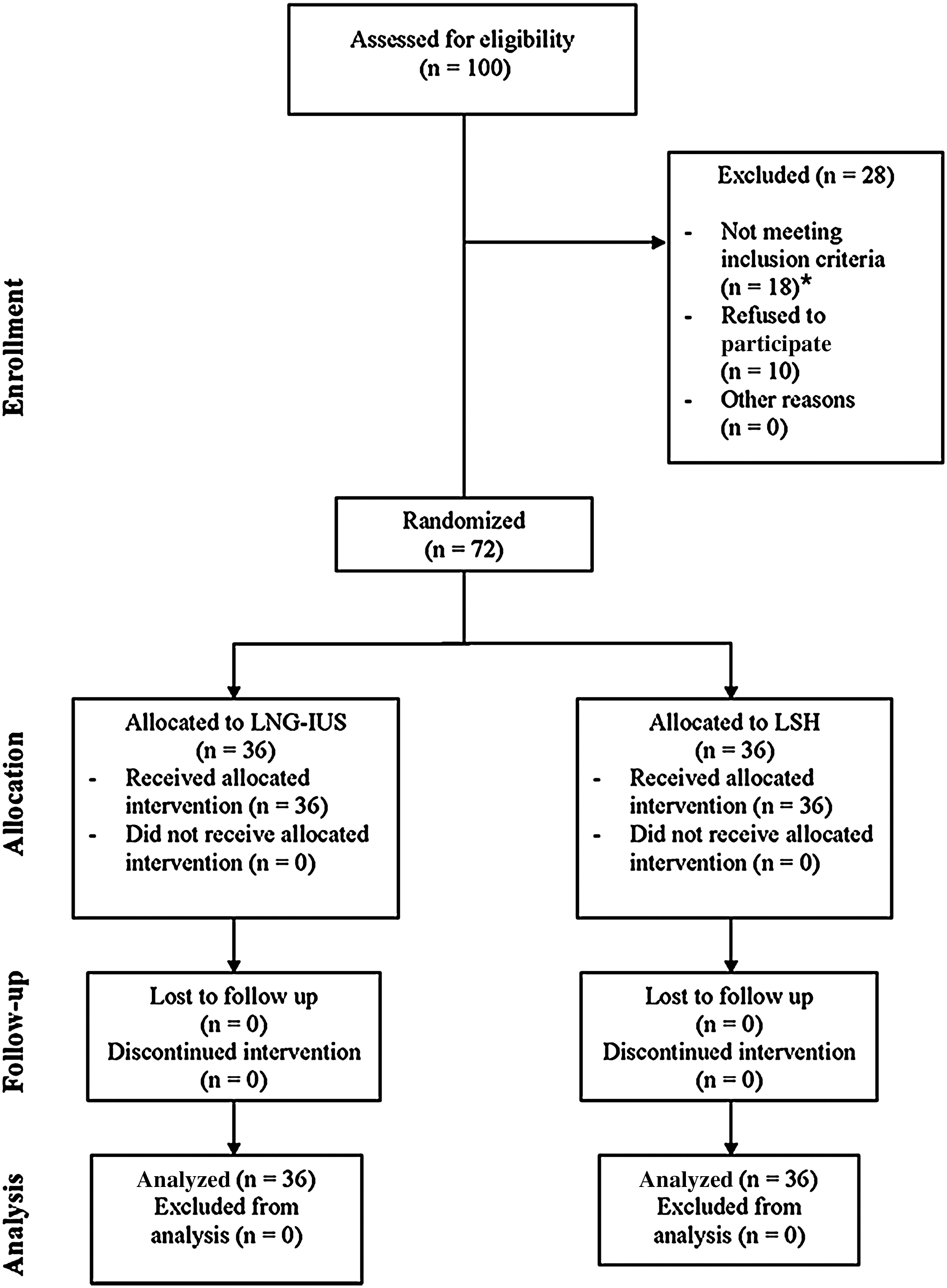
Participant flow through the study. LNG-IUS, levonorgestrel-releasing intrauterine system; LSH, laparoscopic supracervical hysterectomy. *Not eligible because of submucosal fibroids (n=8), endometrial polyps (n=4), previous treatment with LNG-IUS (n=4), or previous treatment with endometrial resection/ablation (n=2).
Surgical technique
LNG-IUS (Mirena®, Leiras Oy, Turku, Finland), which releases 20 μg levonorgestrel over 24 hours, was inserted into the uterine cavity within 7 days of onset of menstruation under paracervical uterine block with 10 mL of ropivacaine (Naropin®, Astrazeneca Spa, Basiglio, Italy). Mirena was loaded into the insertion tube, and after the operator secured the threads, set the flange, and released the arms, the device was advanced up to the uterine fundus and was released, withdrawing the inserter.
Women undergoing LSH were placed in the modified dorsal lithotomy position with Allen stirrups. An uterine manipulator was used, and the bladder was drained continuously. Laparoscopy was performed with a 10-mm principal trocar, introduced through the umbilicus, and two ancillary 5-mm trocars. The uterus was separated from its attachments and blood supply down to the cardinal ligaments using a LigaSure V Sealer/Divider (Valleylab, Boulder, CO). The uterine body and fundus were separated from the cervix at the level of the internal os with a monopolar spatula electrosurgical device. An electric disposable morcellator (X-Tract Tissue Morcellator; Gynecare, Ethicon, Somerville, NJ) was used for specimen removal.
An intent-to-treat analysis of all outcomes on the basis of the original randomization was carried out. The primary outcome of the trial was comparison of the effects on menstrual bleeding (PBAC score) at 12 months after the two procedures. Standardized sanitary products were issued for use during completion of PBAC questionnaires in order to compare the PBAC score between the two groups of women. The score intervals 0, 0–50, 50–100, and >100 were considered, respectively, as amenorrhea, spotting, normal, and heavy blood loss. Bleeding patterns were analyzed considering changes in hemoglobin levels, presence of anemia (defined as hemoglobin <12 g/dL), and bleeding frequency and length. The secondary outcome measures were quality of life, intensity of postoperative pain, and early postoperative complications (any unfavorable episode occurring within 30 days after surgery requiring readmission, blood transfusion, or repeat surgery). Quality of life was assessed using the Medical Outcomes Survey Short Form 36 (SF-36). Postoperative pain was assessed during the first 24 hours using a visual analog scale (VAS) that consisted of a nongraduated 10-cm line ranging from 0 (no pain) to 100 (pain as bad as it could be). Women were subdivided in five categories: absence of pain (VAS=0), mild pain (VAS=1–25), moderate pain (VAS=26–50), severe pain (VAS=51–75), and very severe pain (VAS=76–100).
Statistical analysis
A power calculation verified that >30 patients in each group would be necessary to detect a difference of >50 points in PBAC score, with an alpha error level of 5% and a beta error of 80%. For comparison between the two treatment modalities, the Student's t test was used for normally distributed continuous variables, and the chi-square or Fisher's exact test was used for those variables not following normal distribution. The two treatment groups were compared using a one-way analysis of variance (ANOVA), followed by Tukey's HSD for post hoc comparison of the mean values. A p value<0.05 was considered statistically significant. All analyses were performed using the statistical software SPSS version 15.0 for Windows (SPSS Inc., Chicago, IL).
Results
The two groups of patients did not differ in terms of age, body mass index (BMI), and parity (Table 1). All patients were Caucasian. There were no significant differences in pretreatment bleeding patterns and pretreatment hemoglobin levels (Table 2). Mean operating time was 11.82±1.71 minutes in the LNG-IUS arm and 147.7±11.8 min in the LSH arm (p=0.000). After double checking that the baseline PBAC scores of the two arms were correct, we compared the PBAC scores. The PBAC score was significantly reduced in both treatment groups compared with pretreatment scores. However, at 3 months, there were significant differences in PBAC scores between the two groups (p=0.004), a score respectively corresponding to normal bleeding in the LSH group and spotting in the LNG-IUS group. In contrast, at 6 and 24 months, PBAC scores were significantly lower in women undergoing LSH (normal bleeding) than in those treated with LNG-IUS (spotting) (p=0.000, and p=0.000) (Fig. 2).
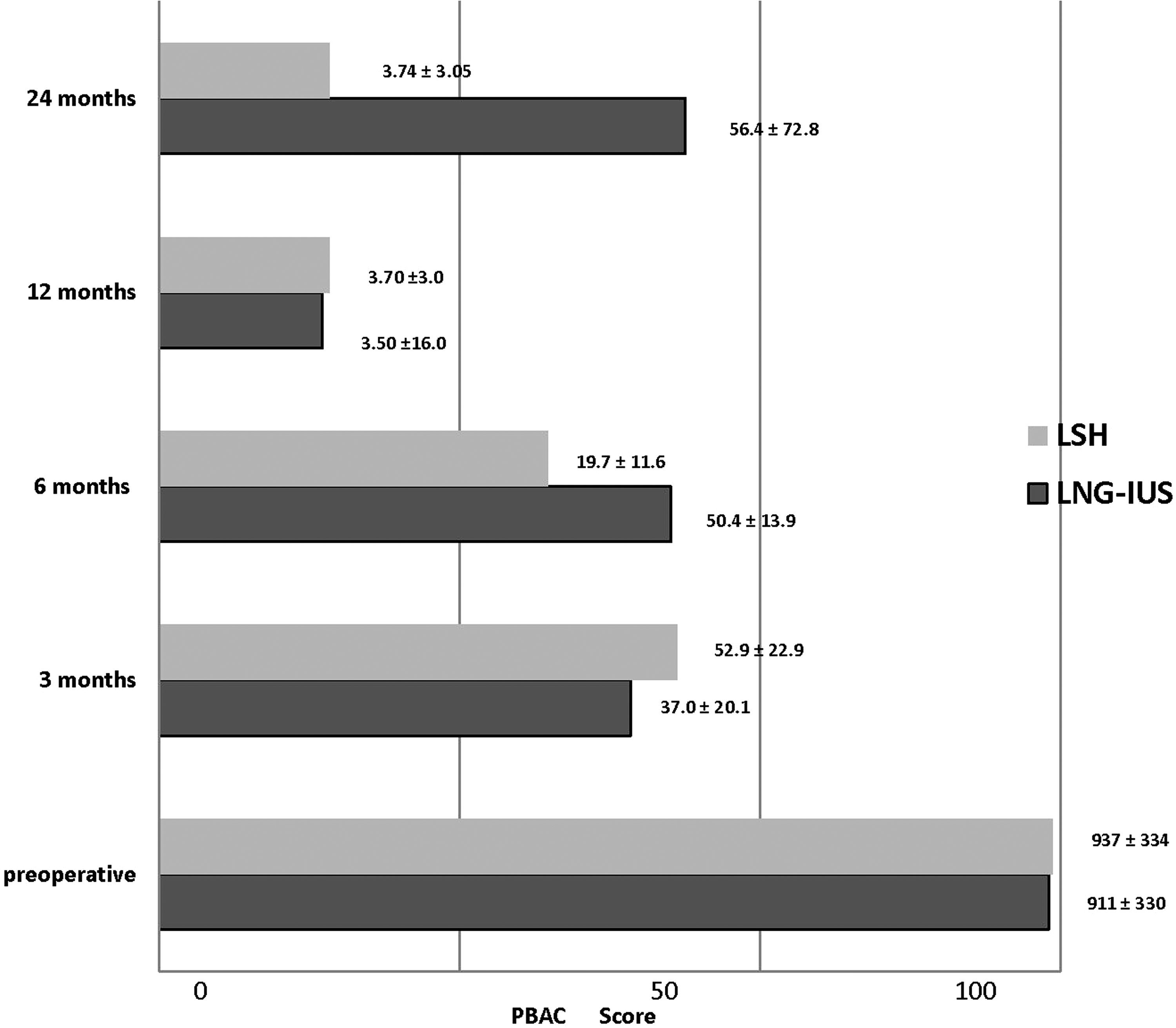
Comparison of pictorial blood loss assessment chart (PBAC) scores between LNG-IUS and LSH at follow-up. Data are presented as mean±standard deviation. (SD). The score intervals 0, 0–50, 50–100, >100 were considered, respectively, as amenorrhea, spotting, normal, and heavy blood loss.
Data are presented as mean±standard deviation (SD).
BMI, body mass index; LNG-IUS, levonorgestrel-releasing intrauterine system; LSH, laparoscopic supracervical hysterectomy.
Data are presented as mean±SD.
PBAC, pictorial blood loss assessment chart.
Subjectively measured bleeding patterns included bleeding frequency and length. After LSH, 8 women (22.2%) had spotting every month at 3 and 6 months' follow-up. At 12 and 24 months' follow-up, all women undergoing LSH had amenorrhea. At 3 and 6 months after LNG-IUS, there was a significant improvement in bleeding frequency and length in comparison to preoperative bleeding patterns (p=0.000) (Fig. 3). At 12 months, no women reported amenorrhea, and 10 (27.8%) reported reduced bleeding frequency and length than at 3 and 6 months' follow-up. However, at 24 months' follow-up after LNG-IUS, patients reported increased bleeding frequency and length than at 3 months' follow-up (p=0.000) (Fig. 3). Only 1 woman (2.8%) reported menorrhagia, with a PBAC score of 97, and 5 women (13.9 %) reported intermenstrual spotting.
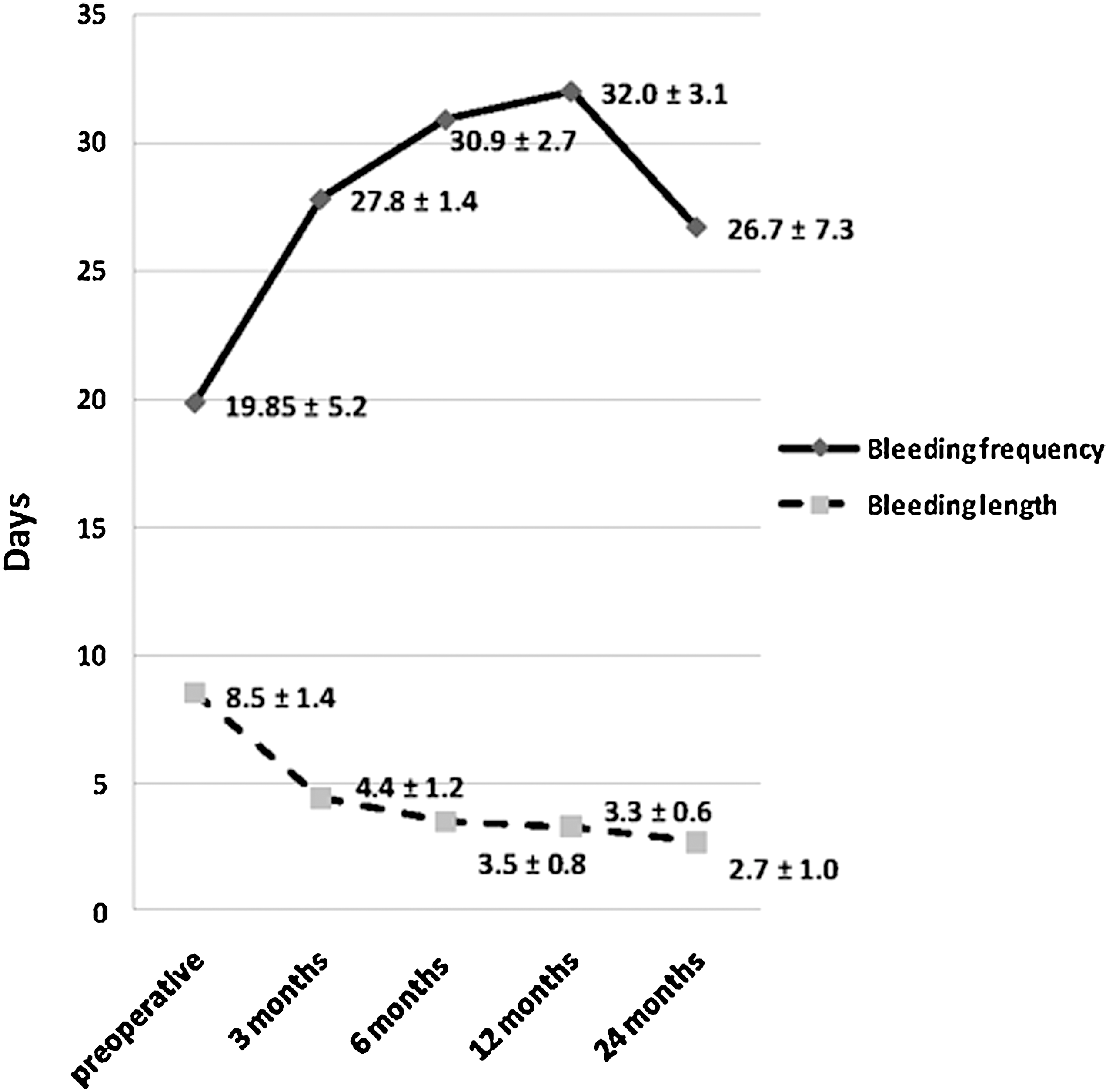
Bleeding frequency and length at follow-up after (LNG-IUS). Data are presented as mean±SD.
Hemoglobin levels were significantly improved in both treatment groups compared with pretreatment levels. However, at 3, 6, 12, and 24 months, women undergoing LSH showed a more significant improvement in hemoglobin levels than did those treated with LNG-IUS (Fig. 4). Postoperative pain intensity at 24 hours was significantly higher in the LSH group in comparison to the LNG-IUS group (p<0.05). After LSH, 32 women (89%) reported moderate pain (VAS=26–50), and 4 (11%) reported mild pain (VAS=1–25). After LNG-IUS, 18 women (50%) reported mild pain (VAS=1–25), and the remaining 18 reported no pain (VAS=0).
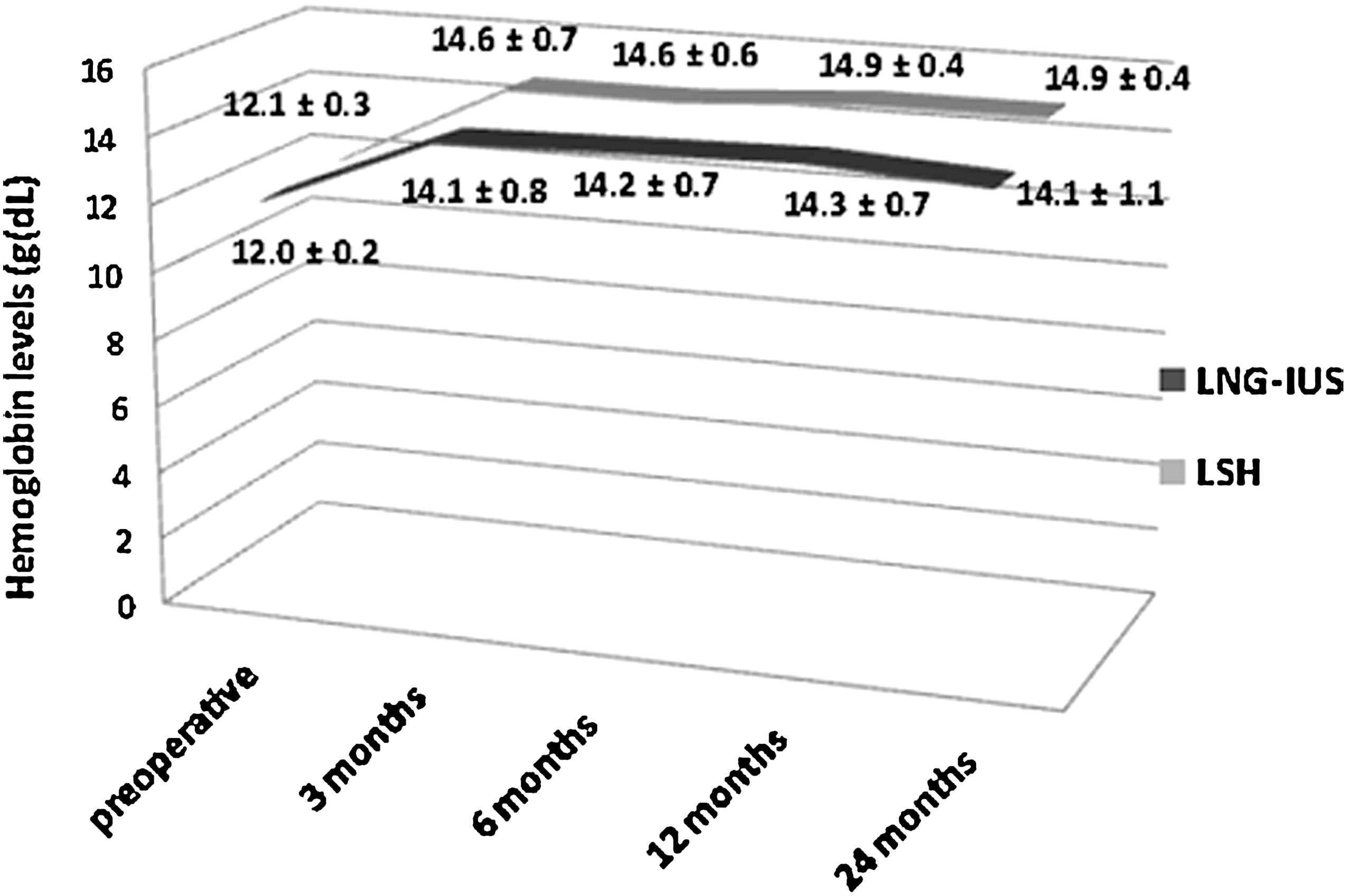
Comparison of hemoglobin levels between LNG-IUS and LSH at follow-up. Data are presented as mean±SD.
In regard to quality of life, the SF-36 scores improved in both groups (Table 3). At 3 and 6 months' follow-up, an improvement in all parameters was observed, but a more significant improvement was seen in the parameters of Vitality, Role (emotional), Role (physical), and Mental health after LNG-IUS (p<0.05) than after LSH. At 12 months' follow-up, the parameters of Role (emotional), Role (physical), Social function, Mental health, and Vitality showed higher scores in women treated with LNG-IUS than in those undergoing LSH (p<0.05). Only the parameters of General health, Physical function, and Pain did not show a statistically significant difference between the two groups at 12 months (p>0.05). At 24 months' follow-up, the parameters of Role (emotional), and Mental health showed higher scores in women treated with LNG-IUS (p<0.05). The parameter of Pain showed a higher score in the LSH group (p<0.05). No early postoperative complications requiring readmission, blood transfusion, or repeat surgery were observed in either group.
Data are presented as mean±SD.
Discussion
HMB is a widespread gynecologic problem that frequently requires medical care. A variety of medical therapies have been proposed as first-line treatment. Antifibrinolytic agents, prostaglandin synthetase inhibitors, and oral contraceptives have shown to be effective in the treatment of HMB. 4 –6 Comparative trials on oral medications vs. surgery indicate that surgery is more effective in most women to reduce menstrual bleeding and improve quality of life. 4 Various studies have shown that LNG-IUS is able to reduce HMB. 7 –9 Moreover, when LNG-IUS was compared to conservative surgery (endometrial ablation), the former was demonstrated to be more efficacious than the latter in reducing uterine bleeding length at 6 and 12 months after surgery. 9 –11 Although hysterectomy clearly represents the most effective treatment modality guaranteeing 100% cessation of menstrual bleeding, its significant physical and emotional repercussions and high social and economic costs cannot be ignored. Therefore, the optimal treatment of HMB remains a challenge for the physician.
There are no randomized trials reported in the literature comparing LNG-IUS with LSH in terms of postoperative outcomes and effects on quality of life. Three randomized trials compared LNG-IUS with abdominal or vaginal hysterectomy, concluding that LNG-IUS can be an alternative to hysterectomy in the treatment of menorrhagia. 3,8,12 No trials, however, compared LNG-IUS with more recent types of minimally invasive hysterectomy, such as LSH. LSH is less invasive and less traumatic than the abdominal approach. 13
To our knowledge, the present article is the first report of a randomized trial aimed at comparing postoperative outcomes and effects on quality of life after LNG-IUS or LSH in a series of women with HMB. To eliminate eventual bias in our study, we adopted strict criteria for the selection of women to be included in the study. Therefore, we excluded women (n=12) with any suspect/concomitant pathology responsible for HMB. We also excluded women who had previously undergone endometrial resection/ablation or were treated with LNG-IUD (n=6). Considering the importance of the surgeon's skill, particularly in laparoscopic surgery, all procedures were performed by the same surgeons using an identical technique.
A PBAC score <100 has been found to be correlated with a measured blood loss <80 mL. 2,14 In our study, although PBAC scores were significantly lower in women undergoing LSH than in those treated with LNG-IUS at 6, 12, and 24 months' follow-up, at 3 months, a higher score was observed in the LSH group. This likely can be explained by the fact that after LSH, 8 women (22.2%) had spotting every month up to 6 months' follow-up. However, the mean PBAC scores after treatment were <100 in both groups; therefore, both arms of treatment were shown to be effective in reducing PBAC scores. In the literature, numerous authors reported analogous PBAC scores after LNG-IUS. 4 Hemoglobin levels were significantly improved in both treatment groups compared with pretreatment levels. However, at 3, 6, 12, and 24 months, women undergoing LSH showed a more significant increase in hemoglobin levels than did women treated with LNG-IUS. The difference in rates of amenorrhea after the two treatments can easily explain the more significant improvement in PBAC scores and hemoglobin levels after LSH.
In regard to the subjectively measured bleeding patterns after LNG-IUS, at 3 and 6 months' follow-up, there was significant improvement in bleeding frequency and length in comparison to preoperative bleeding patterns. At 12 months, no woman reported amenorrhea, and 27.8% reported reduced bleeding frequency and length than at 3 and 6 months' follow-up. However, at 24 months' follow-up, patients reported increased bleeding frequency and length over that at 3 months' follow-up. We are not able to explain this finding; perhaps the local progestin effect of LNG-IUS decreases over time. A longer follow-up period could help elucidate the significance of such a result.
The SF-36 scores reflecting quality of life improved in both groups, although at 24 months' follow-up, only the parameters of Role (emotional), and Mental health showed higher scores in women treated with LNG-IUS. These data do not confirm the results found in the literature. 8 We are not able to explain this finding. Perhaps, the fact that the compliance of our patients treated with LNG-IUS was optimal, in that all women kept LNG-IUS in situ for 2 years, played a role. Alternatively, ethnical, social, psychologic, or other factors may have contributed. In contrast, the parameter of Pain showed a higher score in the LSH group (p<0.05), in accordance with a recent review by Middleton et al. 9 The parameter of General health showed similar scores in both groups, in disagreement with the literature, where this parameter showed a more significant improvement after hysterectomy than after LNG-IUS. 3 This divergence probably can be explained by the fact that we compared a specific type of minimally invasive hysterectomy, that is, LSH, with LNG-IUS, whereas Hurskainen et al. 3 considered other types of hysterectomy. At 3 and 6 months' follow-up, improvement of all parameters was observed, but a more significant improvement in the parameters of Vitality, Role (emotional), Role (physical), and Mental health was found after LNG-IUS than after LSH. At 12 months' follow-up, the parameters of Role (emotional), Role (physical), Social function, Mental health, and Vitality improved in the LNG-IUS arm in comparison to the LSH arm, showing statistically significant differences.
In conclusion, our trial demonstrates that LNG-IUS is an effective treatment modality for HMB, and it is associated with a significant improvement in all parameters related to the quality of life. Thus, it can be considered as first-line treatment for HMB unresponsive to drug therapy, and it is particularly suitable for women who want to preserve an acceptable menstrual flow instead of amenorrhea. LSH may be considered the best surgical option in women with HMB unresponsive to any medical treatment because it showed a definitive improvement in symptoms together with a satisfactory life quality profile. Further controlled prospective studies are required, however, to confirm our results about the effectiveness and compliance of different therapeutic approaches in women with HMB.
Footnotes
Disclosure Statement
The authors state that no competing financial interests exist.