
Abstract
Background:
Our objective was to explore the potential benefits of molecular breast imaging (MBI) as a screening technique in women undergoing stress myocardial perfusion studies.
Methods:
MBI was offered to women receiving Tc-99m sestamibi injection for myocardial perfusion stress testing. During the required waiting period after stress isotope injection, MBI was performed using a dedicated breast imaging gamma camera system. MBI examinations were interpreted by breast radiologists, with review of a recent mammogram in cases with positive MBI.
Results:
Of 322 women enrolled, 313 completed MBI, comprising 5 with known breast cancer, 2 with known high-risk benign breast lesions, and 306 who were asymptomatic for breast disease with a recent negative mammogram. Analysis was limited to the 306 patients with no known breast disease. MBI was positive in 22 of 306, giving a recall rate of 7.2% (95% confidence interval [CI] 4.8-10.6]. MBI detected 4 new cancers, resulting in a supplemental diagnostic yield of 13.1/1000 women screened (95% CI 5.1-33.2). The number of cancers diagnosed per abnormal MBI examinations (PPV1) was 18% (4 of 22) (95% CI 7.3-38.5), and the number diagnosed per MBI-prompted biopsies (PPV3) was 44% (4 of 9) (95% CI 18.9-73.3).
Conclusions:
The addition of MBI to clinically indicated stress myocardial perfusion imaging studies in women results in a high diagnostic yield of newly detected breast cancers while generating a low rate of additional unnecessary workup.
Introduction
Mammography is the principal screening and diagnostic imaging modality for the detection of breast cancer. Estimates of the sensitivity of mammography in the general population vary from 71% to 96% 1 ; however this sensitivity is significantly reduced in certain subgroups of women, notably women under the age of 50 years, 2 women with dense breast parenchyma, 3 and women at increased risk for breast cancer. 4 Recognition of the limitations of mammography in these subgroups has fueled interest in alternative breast imaging modalities that offer potential improvements in sensitivity and specificity, particularly in the subgroups of women for whom the sensitivity of mammography is impaired. One of these potential screening techniques is molecular breast imaging (MBI). This technique uses two opposing semiconductor-based gamma cameras optimized for breast imaging (Fig. 1) in order to image the distribution of a tumor-seeking radiopharmaceutical, Tc-99m sestamibi, in the breast tissue. 5 Several studies have shown that this technique has a high sensitivity for detection of small breast lesions (<15 mm in size). 6 –8

Prototype dual-head molecular breast imaging (MBI) system comprising two cadmium zinc telluride detectors (GE Medical Systems, Haifa, Israel) mounted on a modified mammographic gantry.
We have previously evaluated MBI as a potential screening technique in women with mammographically dense breasts on past prior mammogram (considered either heterogeneously or extremely dense by Breast Imaging Reporting and Data System [BI-RADS] categories) 9 and additional risk factors for breast cancer. 10 In that work, the addition of MBI to routine screening mammography significantly increased sensitivity for breast cancer detection from 27% with mammography alone to 91% for the combination of mammography and MBI (p=0.016). The specificity of MBI alone was 93%, and the specificity of MBI combined with mammography was 85%. Of the eight supplemental cancers detected by MBI in that study, three were detected in women with only slightly elevated risk for breast cancer by Gail model (5-year risk between 1.7% and 2.5%), and one was detected in a woman with breasts not considered dense on her current study mammogram (BI-RADS category of scattered fibroglandular densities). These findings raised the question of whether or not this technology may also be a valuable adjunct imaging tool in women who do not have the highest categories of breast density or who do not have additional risk factors for breast cancer.
In large clinical trials evaluating new potential screening techniques, such as contrast-enhanced magnetic resonance imaging (MRI) or whole-breast ultrasound, patient selection is usually limited to subgroups of the eligible screening population where mammography is known to be of limited use, such as women at elevated risk for breast cancer. Breast density is itself an independent risk factor for developing breast cancer, 11 and there is often considerable overlap among groups of women with dense breasts and those with additional risk factors, such as elevated risk by risk-prediction models. Although the American Cancer Society (ACS) has recommended annual screening MRI for women in the highest risk categories, such as those with >20% lifetime risk or mutations in BRCA-1 or BRCA-2 genes, they concluded that not enough evidence exists to recommend MRI screening on the basis of breast density alone. 12 To date, there are few studies and little information on how alternative screening techniques perform in an average-risk screening population.
Whereas breast cancer and cardiovascular ischemia have traditionally been diagnosed through very different imaging modalities, in nuclear medicine the radiopharmaceutical, Tc-99m sestamibi, has the unique distinction of being employed in both cardiac imaging and certain types of tumor imaging (mainly parathyroid adenomas and breast cancer). This radiopharmaceutical was originally developed in the mid-1980s for myocardial perfusion imaging, 13,14 but soon after its introduction, it was recognized that its uptake was not tissue specific but rather proportional to mitochondrial and plasma transmembrane electrical potentials, which are higher in tumors because of their increased metabolic requirements. 15 The affinity of this radiopharmaceutical for both nonischemic myocytes and malignant breast tumors provides a unique opportunity to evaluate the performance of MBI in a population of women undergoing myocardial perfusion imaging. This is a population that would be assumed to be at average risk of breast cancer, as there is no evidence to date of an association between breast cancer and heart disease. Hence, the performance of MBI in this subgroup may provide valuable information on how MBI would perform in a wider screening setting, in terms of its supplemental diagnostic yield, the false positive rate, and positive predictive value.
The primary aim of this study was to explore the potential benefits and drawbacks of MBI as a screening technique in a population of women who were undergoing stress myocardial perfusion studies, with the long-term aim of evaluating the potential use of MBI as a screening tool for breast cancer in an average-risk population.
Patients and Methods
Study population
All women undergoing a nuclear cardiology stress single photon emission computed tomography (SPECT) study at Mayo Clinic Rochester between January 2008 and June 2010 were offered participation in this IRB-approved, Health Insurance Portability and Accountability Act (HIPAA)-compliant protocol through the provision of study brochures in the waiting room of the nuclear cardiology clinical area. Patients who expressed an interest in participating were assessed for eligibility. Women were eligible if they (1) were scheduled to undergo a same-day stress myocardial perfusion imaging study with Tc-99m sestamibi injection and (2) had a mammogram performed within the preceding 12 months either at Mayo Clinic or elsewhere that was available for review in the event of a positive MBI study. Patients were ineligible if they were physically unable to sit upright and remain still for 20 minutes. Informed consent was obtained from all participants.
Imaging procedures
Patients underwent a clinically indicated low-dose rest/high-dose stress myocardial perfusion SPECT study. During the period of this study, worldwide shortages of Tc-99m caused variability in the amount of Tc-99m sestamibi routinely used for myocardial perfusion imaging in our laboratory. The majority of patients received 300–444 MBq (8–12 mCi) Tc-99m sestamibi as a resting dose and subsequently underwent cardiac rest imaging. After exercise or pharmacologic stress, patients typically received 1180–1628 MBq (32–44 mCi) Tc-99m sestamibi depending on the protocol used. In a subset of patient studies, the administered doses were reduced by a factor of 2. The total injected dose of Tc-99m sestamibi (low-dose rest+high-dose stress) ranged from 666 to 2035 MBq (18 to 55 mCi), with mean, median, and standard deviation (SD) of 1642 MBq (44 mCi), 1850 MBq (50 mCi), and 444 MBq (12 mCi), respectively.
Cardiac stress imaging commenced 30–45 minutes after completion of the exercise or pharmacologic stress procedure. Myocardial perfusion studies were performed using conventional dual-head, large field of view gamma cameras.
During the required waiting period between cardiac stress injection and stress imaging, MBI was performed. MBI imaging commenced approximately 5 minutes after completion of the exercise or pharmacologic stress procedure, which was approximately 75 minutes postrest injection and 15 minutes poststress injection. The MBI system comprised two opposing 20×20 cm CZT-based detectors (prototype Discovery NM 750b, GE Healthcare, Haifa, Israel), previously described, 5,8 that were mounted on a modified mammographic gantry. Two images were acquired of each breast in views analogous to those used for mammography, the craniocaudal (CC) and mediolateral oblique (MLO) projections. Patient positioning was performed by nuclear medicine technologists trained in mammographic positioning. For each view, gentle stabilization was applied by lightly compressing the breast between the two detector heads. Compressed thickness was recorded. Image acquisition was 3 minutes/image. Acquisition time was extended to 5 minutes/image in patients who received reduced doses of Tc-99m sestamibi as described above.
Image interpretation and workup
Interpretation of MBI images was performed by radiologists specializing in breast imaging with 1–3 years experience in the interpretation of MBI studies (D.A.C. and C.L.T.). MBI images were examined for the presence of abnormal tracer uptake and scored using an assessment of 1 to 5, which paralleled the BI-RADS assessment, 9 where 1=no abnormal uptake, 2=benign, normal physiologic uptake, 3=indeterminate uptake, 4=uptake suspicious for malignancy, and 5=uptake highly suggestive of malignancy. Assessments of ≥3 were considered test positive, and scores of 1 or 2 were considered test negative. Positive MBI findings were reviewed in conjunction with the most recent mammogram. At this review, previous mammograms, reports, and all ancillary patient information were accessed where available.
Positive MBI studies prompted diagnostic evaluation as follows. If the abnormality on MBI corresponded with stable or benign findings on a recent mammogram, no further workup was performed. If the MBI abnormality was not explained by benign findings on mammography, further diagnostic workup, which may have included diagnostic mammogram, directed ultrasound, MRI, 6-month follow-up MBI, or biopsy, was performed as necessary and according to the established standard of care at Mayo for patients with positive MBI findings. 10
In patients with positive findings on MBI, a radiologist specializing in both nuclear medicine and breast imaging (D.A.C.) reviewed the raw data and reconstructed transaxial images from the myocardial perfusion studies to assess whether the MBI abnormality could retrospectively be detected on the myocardial perfusion examination.
Analysis
The final histopathology of lesions was determined from the most severe of results obtained from core needle biopsy or surgical excision. All malignancies and high-risk lesions were excised. Lesions that were detected by MBI but not biopsied because of negative or benign findings on subsequent diagnostic workup were classified as false positive if findings remained negative or benign at >1 year of follow-up.
Patients with known breast cancer or known high-risk breast lesions at the time of study entry were excluded from the analysis. In patients considered asymptomatic for breast disease with negative recent mammogram before enrollment, the diagnostic yield, recall rate, and positive predictive value of MBI were calculated. Diagnostic yield was defined as the proportion of women with positive MBI and histopathologically confirmed cancer diagnosis and expressed as per 1000 women screened with MBI. Recall rate was defined as the percentage of patients with abnormal findings on MBI that prompted comparison with prior mammogram or further diagnostic imaging or both. Positive predictive values (PPVs) were calculated as the ratios of number of patients with breast cancer per number of abnormal MBI examinations (PPV1) and the number of breast cancers diagnosed per number of biopsies performed (PPV3). Exact 95% confidence intervals (CIs) were calculated using the Wilson method without continuity correction. 16
Results
A total of 322 women were enrolled and consented to the study, of whom 313 completed MBI imaging. Seven patients were excluded from the analysis because they had known breast disease detected by prior screening mammogram, leaving 306 patients in the analysis set with no known breast disease or symptoms and negative screening mammogram performed within the previous 12 months. Participant characteristics of the analysis set are listed in Table 1. The mean compressed breast thickness for all MBI views acquired was 7.7 cm, with a median of 7.8 cm, SD of 1.3 cm, and range of 3.8–12 cm.
Analysis set includes participants who were considered asymptomatic for breast disease, had a negative mammogram within<12 months before study entry, and completed molecular breast imaging (MBI).
Participants may have had more than one additional risk factor but were assigned to only one risk factor category. Risk factors are listed in order of most risk.
Figure 2 provides a flowchart of findings and diagnostic workup performed in participants. MBI was interpreted as negative or benign (assessment 1 or 2) in 284 of 306 (93%) participants and positive (assessment ≥3) in 22 of 306 (7%) participants. In the 22 positive MBI studies, 4 were resolved as benign findings through combined review of MBI with recent mammogram, and 18 prompted further diagnostic workup as follows. Diagnostic mammogram and directed ultrasound were performed in all 18, resulting in benign findings and no further workup in 2, performance of 6-month follow-up MBI in 6, performance of ultrasound-guided biopsy in 5, and further evaluation by contrast-enhanced breast MRI in 5. Of the 5 patients who had MRI performed to evaluate an MBI abnormality, 1 had benign findings and no further workup was performed, and 4 prompted MRI-guided biopsy. In all 6 cases where 6-month follow-up MBI was performed, the lesions were either less intense or no longer apparent at 6 months and, therefore, resolved as benign.

Flowchart of workup performed to evaluate positive MBI findings and the resulting diagnoses. ADH, atypical ductal hyperplasia; DXMG, diagnostic mammogram; MRI, magnetic resonance imaging; SXMG, screening mammogram.
Overall, there were 13 patients with positive MBI findings in whom further workup did not warrant biopsy; in 11 of these patients, a negative mammogram performed at least 1 year later confirmed negative cancer status, and in the remaining 2, a telephone interview at least 2 years later confirmed no signs or symptoms of breast cancer.
A total of 9 biopsies (5 by ultrasound and 4 by MRI in 9 patients) were prompted by abnormal MBI findings, resulting in a diagnosis of cancer in 4 patients and benign findings in 5 patients. The 4 cancers detected by MBI in asymptomatic patients included a 1.2-cm mixed invasive ductal carcinoma (IDC)/invasive lobular carcinoma (ILC), a 0.9-cm IDC, a 0.2-cm IDC with 0.6-cm ductal carcinoma in situ (DCIS), and a 0.3-cm DCIS (Table 2). Figures 3 and 4 show examples of patients with breast cancer detected by the addition of MBI at the time of the myocardial perfusion study. The 5 benign biopsy findings comprised a fibroadenoma, an intramammary lymph node, sclerosing adenosis; benign breast parenchyma with focal stromal fibrosis and dilated ducts, and atypical ductal hyperplasia (ADH) (no cancer found at excision). The patient with false positive MBI and benign findings of fibroadenoma is shown in Figure 5.

Breast images from patient 3, with a 0.9-cm invasive ductal carcinoma (IDC). (
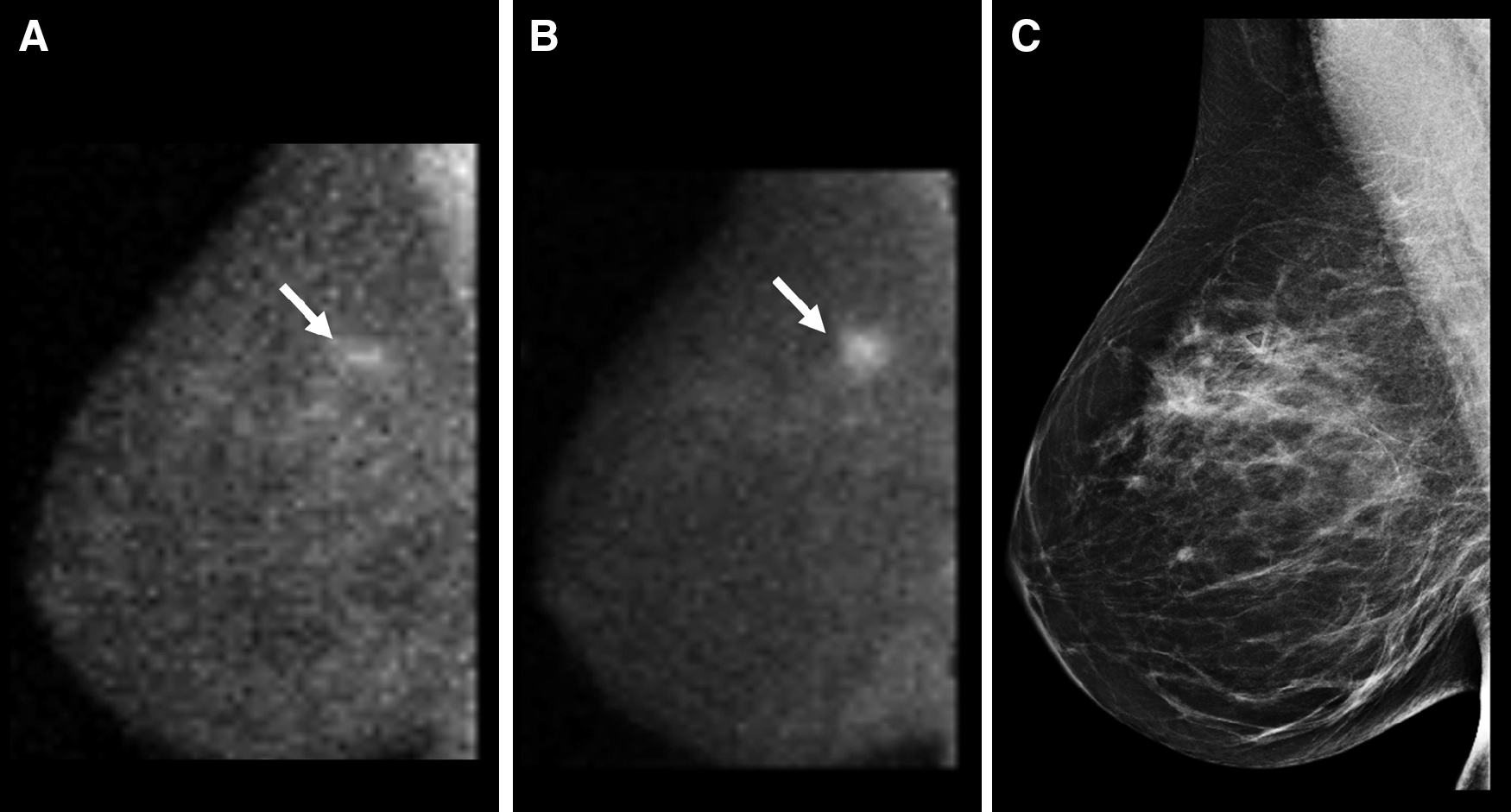
Breast images from patient 4. (
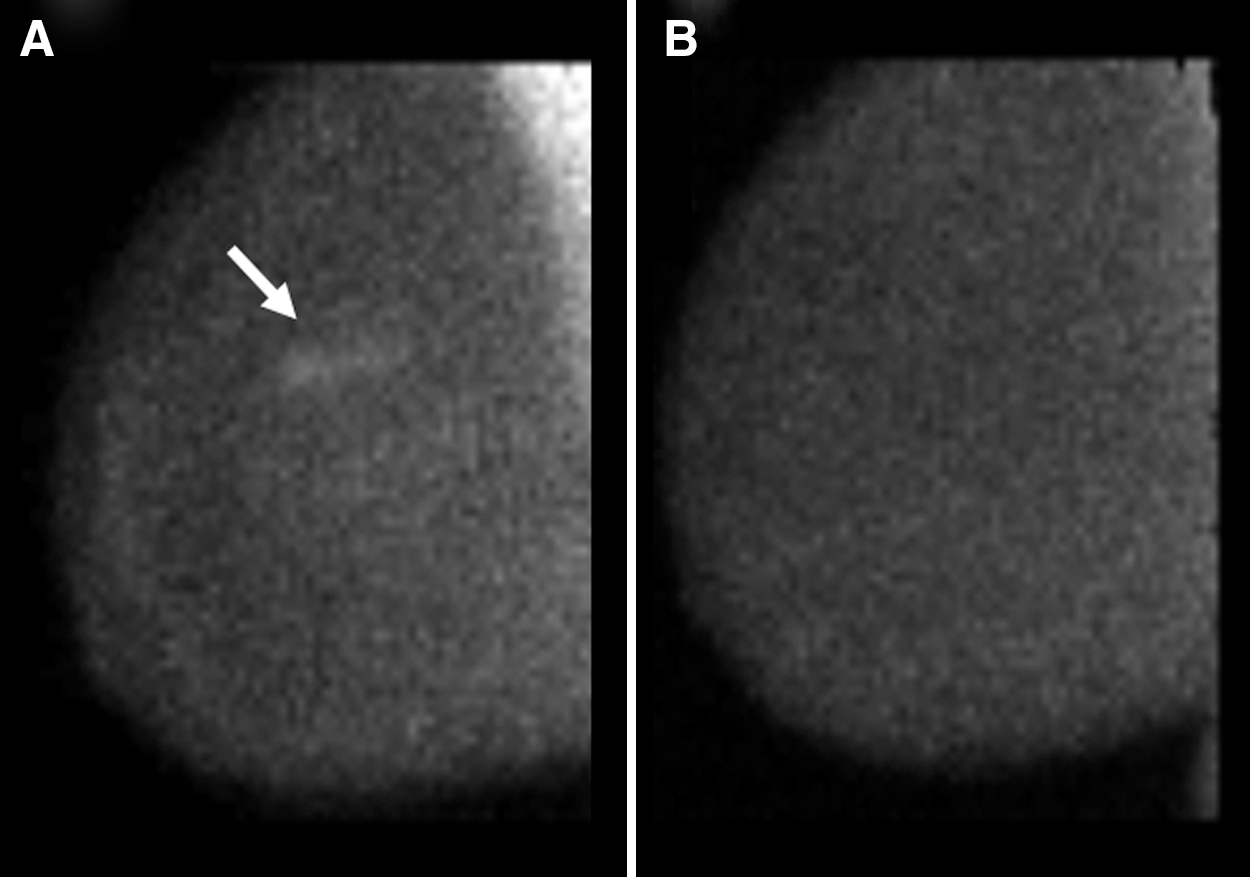
Breast images from a patient with false positive findings on MBI. (
Each participant was assigned a single risk factor category in order of priority as listed in Table 1.
MBI assessment of≥3 was considered positive.
DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; TNM, tumor, node, metastasis.
The diagnosis of breast cancer in 4 of 306 patients with addition of MBI to myocardial perfusion imaging resulted in a supplemental diagnostic yield of 13.1/1000 women screened (95% CI 5.1-33.2). The recall rate for MBI was 7.2% (22 of 306) (95% CI 4.8-10.6). Per 22 abnormal MBI examinations and 9 MBI-prompted biopsies, cancer was diagnosed in 4 patients, giving PPV1=18% (4 of 22) (95% CI 7.3-38.5) and PPV3=44% (4 of 9) (95% CI 18.9-73.3). Retrospective review of the raw data and reconstructed transaxial data from the myocardial perfusion studies did not lead to detection of any areas of abnormal uptake in the breasts.
The 7 patients excluded from analysis because of known breast disease included 5 patients with biopsy-proven cancers in the breast and 2 patients with biopsy-proven high-risk breast lesions scheduled for excision. The 5 patients with known cancer comprised 4 with breast cancer (all IDC), and 1 patient with non-Hodgkin's lymphoma with lesions in the breast. MBI was positive in 4 of 5 known cancers. In the fifth patient, the MBI demonstrated bilateral false positive uptake in skin keratoses, but MBI did not detect the known IDC initially diagnosed on mammography. Of the 2 patients with known high-risk benign lesions, 1 patient had a radial scar and 1 had ADH. MBI was positive in the radial scar and negative in the ADH. No cancer was found on final pathologic examination at excision of either high-risk lesion.
Discussion
This exploratory study was intended to provide preliminary information on how well MBI would perform as a screening technique in a population of women at average risk of breast cancer. We selected the population of women already receiving Tc-99m sestamibi injection for clinically indicated myocardial perfusion studies at Mayo Clinic. The results showed that the recall rate for MBI in this population (7%) was comparable to that reported in our prior study of MBI in women with dense breasts and additional risk factors for breast cancer (8%). 10 In that study, the specificity of MBI (93%) was comparable to that of screening mammography (91%). The low recall rate for MBI observed in the current work is an important confirmatory finding, as a high recall rate would significantly diminish the potential usefulness of MBI in a screening environment. Ongoing 17 and prior studies of MBI 10 in the screening environment have focused exclusively on its potential value in the population of women with dense breast tissue on mammography. As Table 1 shows, the range of mammographic densities seen in this study matches that of the general population. 18 Hence, with respect to specificity, this study would indicate that MBI may have a broader role as a useful imaging tool in other subgroups of the screening population and not just in those with the highest categories of mammographic density.
An unexpected finding of this study was the number of mammographically occult breast cancers detected on MBI. The addition of MBI resulted in a diagnostic yield of 13.1 cancers per 1000 patients screened (95% CI 5.1-33.2). The typical yield of breast cancers from screening mammography is ∼3–4/1000 patients screened. 19 Although the overall number of cancers detected in this study was small and, hence, subject to large statistical variation, it is interesting to note that the diagnostic yield in this study mirrors our prior findings in women with dense breasts and additional risk factors. 10 The prior study demonstrated a diagnostic yield of 9.6/1000 (95% CI 5.1-18.2) for MBI compared to 3.2/1000 (95% CI 1.1-9.3) for mammography. However, there are substantial differences between these two studies. The prior study was restricted to women with dense breast tissue, whereas the current study was open to all women undergoing myocardial perfusion imaging, of whom at least 50% did not have dense breast tissue. Risk assessment also showed that the current cohort comprised a very low number of women with elevated risk for breast cancer; nearly 50% had no additional known risk factors (Table 1). Hence, the current study was not expected to have a comparable diagnostic yield.
There are a number of possible explanations for the unexpected high diagnostic yield of breast cancer in this study. First, this was an older population (average age 64 years) compared to that in the prior study (average age 55 years) who, therefore, have an age-related increased likelihood of breast cancer by 50%. 20 There may also be self-selection bias in that women who considered themselves to be a higher risk of breast cancer may have been more interested in participating in this study. Finally, patients who undergo myocardial perfusion imaging are more likely to be obese and to smoke, factors that also place them at slightly increased risk of breast cancer. 21, 22
Breast cancer and cardiovascular disease (CVD) are two of the most important health issues for women in the United States. In a survey conducted by the Society for Women's Health Research, breast cancer and CVD were the two specific conditions that women most fear. 23 The clinical situation of women undergoing myocardial perfusion imaging presents a unique opportunity to evaluate the potential value of MBI as a screening technique in a subgroup of women not preselected because of breast density or additional risk factors for breast cancer. This is not a trivial population, as the number of myocardial perfusion scans performed annually in the United States was reported as 9,400,000 in 2008, 24 with approximately 40% of studies (3,760,000 studies) being performed in women. 25 By comparison, approximately 37 million mammograms are performed annually in the United States, with the majority of these being performed in women in their 40s–70s. Hence, this combined heart/breast scan would enable evaluation of a large population of women with minimal inconvenience.
Obviously, the potential societal benefits for a combined heart/breast procedure are dependent on multiple factors, such as availability of a dedicated breast imaging system in or adjacent to a nuclear cardiology facility, reimbursement for the added cost of the MBI scan, and its interpretation. There are benefits to the patient in that both tests can be accomplished in a single visit with only one injection of a radiopharmaceutical, thereby avoiding additional radiation exposure. The MBI procedure is generally well tolerated by patients; it involves only light breast compression and, in this setting, can be completed in <20 minutes (3–5 minutes/view). There is the additional advantage that MBI may be a more sensitive test for breast cancer than mammography, particularly in this subset of the population. Interestingly, the relatively low sensitivity of exercise ECG testing for heart disease in women can often cause preferential referral of women over men for nuclear cardiology stress testing. 26 The sensitivity limitations of routine screening mammography for breast cancer and exercise ECG testing for heart disease make this combined nuclear medicine approach particularly compelling in the appropriate setting.
On a practical level, several factors work in favor of a combined heart/breast study. First, Tc-99m sestamibi demonstrates rapid clearance from the bloodstream, allowing breast imaging to commence ∼5 minutes postinjection. Hence, the MBI study can be performed during the standard 30–45-minute waiting period after stress isotope injection. Second, Tc-99m sestamibi doses for cardiac studies are typically more than 4–5 times greater than those currently used for MBI, 27 allowing the total MBI study to be completed in 15–20 minutes, without extension of the cardiac study examination time or extending the patient's time in the laboratory. Third, the relative uptake of Tc-99m sestamibi in organs is dependent on both regional blood flow and mitochondrial activity. 15 Blood flow is significantly increased during the stress phase of a myocardial perfusion imaging examination, a factor that may have contributed to detection of breast cancers in this study. 28 Prior work by Fleming 29 demonstrated that administration of adenosine before breast scintigraphy increased isotope delivery to breast lesions and improved the ability to distinguish infiltrating breast cancer and precancerous lesions from normal breast tissue.
There were noteworthy limitations to this study. The study was not designed to compare MBI with mammography, and the timing of the MBI study was dictated by that of the myocardial perfusion scan and was not timed to match that of the patient's normal schedule for mammographic screening. We do not know if the cancers diagnosed as a result of the MBI would have been apparent on mammography at the time of the next scheduled screening, nor do we know if the earlier detection was associated with a mortality benefit. Of the four supplemental cancers diagnosed in asymptomatic patients, however, a median time of only 2.1 months (range 0.1–7.9 months) had elapsed since their last mammogram. Therefore, it is likely that these cancers were present but mammographically occult at the time of the previous screen. In 3 of 4 of these cancers, the previous mammogram was considered heterogeneously dense, and all 4 tumors were ≤1.2 cm, two factors demonstrated to correlate with reduced mammographic sensitivity and, thus, a reduced likelihood of these cancers being detected on subsequent screening mammogram. 3,30 A 1-year follow-up study was not performed in a substantial proportion of patients with negative or benign MBI findings, as it was outside the scope of this project. Thus, we cannot calculate true sensitivity without a reference standard, which is usually determined by negative or benign imaging at least 330 days after the initial study or by benign histopathology or by medical record review or patient interview confirming no breast cancer diagnosis. 31 Also, the number of cancers detected in this study was small and subject to a large statistical range. A more extensive study would be required to determine to what degree the above factors influenced the high prevalence of breast cancer found in this study.
Finally, it should be noted that the radiation dose associated with stress myocardial perfusion SPECT imaging is at least four times higher than that used for MBI breast imaging when done independently. Therefore, it is important that the indication for nuclear stress imaging of the heart be the primary driver of combined heart/breast sestamibi testing rather than the desire for supplemental breast imaging.
Conclusions
The addition of MBI to clinically indicated stress myocardial perfusion imaging studies in women results in a high diagnostic yield of newly detected breast cancers, while generating a low rate of additional unnecessary workup. In this population, MBI appears to have excellent specificity and may be a potential screening tool for breast cancer.
Footnotes
Acknowledgments
This work was funded by Mayo Foundation and a grant from Friends for an Earlier Breast Cancer Test. We gratefully acknowledge the study assistance provided by nuclear medicine technologists Thuy Truong, CNMT, and Carley Pletta, CNMT, and study coordinators Beth Connelly and Tamara Hudson.
Disclosure Statement
C.B.H. and M.K.O. receive royalties from development of technologies licensed to Gamma Medica. This is a competing company to GE Healthcare in the development of MBI. Mayo Clinic holds equity in Gamma Medica. D.J.R., D.A.C., C.L.T., and J.W.A. have no actual or potential conflicts of interest.