
Abstract
Background:
Chronic kidney disease (CKD) is associated with increased risk of cardiovascular (CV) events and death. However, the effect of cardiorespiratory fitness on the CKD-mortality relationship remains unknown, particularly in women.
Methods:
We used Cox regression to estimate hazard ratios (HR) for the effect of kidney function and fitness on all-cause mortality in a prospective cohort of 5716 women free of CKD and CV disease symptoms. Serum creatinine (Cr) was used to estimate glomerular filtration rate (eGFR), and spot urine protein and maximal stress tests were performed at baseline.
Results:
Mean age at baseline was 52.5±10.8 years, and 86% of the sample was Caucasian. Mean Cr was 1.11±0.14 mg/dL, and mean eGFR was 53.7±8.3 mL/min/1.73 m2 at baseline. The mean follow-up was 15.9±2.2 years, with 589 deaths identified. Cr <1.4 was associated with an HR of death of 1.59 (p=0.03). After adjustment for traditional CV risk factors and fitness, the risk of death decreased by 3% (p<0.001) for every mL/min/1.73 m2 increase in eGFR. Compared to women with an eGFR <45 mL/min/1.73 m2, the risk of death was reduced by 36% and 47%, for eGFR 45–59.9 mL/min/1.73 m2 and eGFR ≥60 mL/min/1.73 m2, respectively (p<0.001). At every level of eGFR, fitness remained an independent predictor of mortality, with the lowest level of fitness (<5 metabolic equivalents [METs]) at the highest risk of mortality regardless of eGFR level.
Conclusions:
Fitness remains an independent predictor of mortality regardless of eGFR. eGFR was a stronger predictor of mortality compared to Cr or the presence of proteinuria. These findings have important implications for clinical practice and health policy, as the level of cardiorespiratory fitness predicts risk of death in the presence of asymptomatic CKD.
Introduction
Chronic kidney disease (CKD), as defined by an estimated glomerular filtration rate (eGFR) of <60 mL/min/1.73 m2, affects over 20 million adults in the United States. 1 CKD is an independent risk factor for all-cause mortality and cardiovascular (CV) disease, and its prevalence is increasing. 2 –8 As the burden of CKD is growing worldwide, the importance of preventing end-stage kidney disease is of immediate importance to the individual, the population, and the healthcare community.
People with CKD represent the highest-risk group for CV events and mortality after a cardiac event. 9 –11 However, CKD is not well-recognized and is often not assessed when estimating CV risk, despite its association with all-cause and CV mortality. Despite numerous studies showing a strong and independent association between reduced GFR and poor prognosis, risk factor management is often not optimized in the community setting, 12 and screening for kidney disease is often limited to createnine (Cr). In addition, CV disease remains the leading cause of mortality among women; however, the assessment of kidney function is not included in the current American Heart Association (AHA) guidelines for heart disease prevention in women. 13,14
Despite the awareness that CKD is associated with an increased mortality, little is known about how to reduce the impact of CKD on mortality among women, particularly those with lesser degrees of CKD. It remains unknown if the level of cardiorespiratory fitness impacts the relationship between CKD and mortality among asymptomatic women. We evaluated the association between CKD, using eGFR, with all-cause mortality in a group of asymptomatic women. We further assessed the effect of baseline cardiorespiratory fitness level, measured by a maximal exercise stress test, on the relationship between CKD and all-cause mortality.
This study was approved by the St. James Hospital and the Ohio State University's Institutional Review Board.
Materials and Methods
Participants
This cohort of women is known as the St. James Women Take Heart (WTH) Project. The St. James WTH cohort has been described in full previously. 15,16 Briefly, in 1992, a call for volunteers from the greater Chicago metropolitan area resulted in a cohort of 5932 women who were free of CKD symptoms. Inclusion criteria were age ≥35 years, the absence of active CV disease (CVD), and an ability to walk on a treadmill at a moderate pace. Women were excluded if they were pregnant or had experienced typical anginal symptoms or myocardial infarction (MI) within the previous 3 months, weighed >325 pounds, or had blood pressures ≥170/110 mm Hg before initiating the stress test.
All participants underwent a physical examination, which included height, weight, waist and hip measurements, blood pressure, radial pulse rate, and auscultation of the heart and lungs. Body mass index (BMI) was calculated as weight in kilograms divided by the height in meters squared (kg/m2). During recording of the baseline resting electrocardiogram (ECG), supine blood pressures were measured by technicians using standard clinical procedures. 17 Standing blood pressures were recorded before the start of the exercise treadmill. Random urine and nonfasting blood assays were collected for laboratory analysis. Findings suggestive of congestive heart failure (CHF), valvular disease, or peripheral vascular disease were referred to the attending cardiologist. Study-specific exclusion criteria included (1) performance of the modified-Bruce Protocol (n=109), (2) presence of any cardiac disease, including previous MI, documented CVD, heart failure, or valvular heart disease (n=91), (3) incomplete data concerning cardiac risk factors (n=11), and (4) missing or incomplete data on kidney function (n=5). The final sample size use 5716.
All-cause mortality was determined using a Social Security Death Index search to identify all deaths following the baseline evaluation in 1992 through December 31, 2008.
Measures of kidney function
Creatinine
Serum Cr was measured on a single sample of unfrozen serum taken at the baseline examination.
Estimated GFR
We estimated the GFR at baseline with the use of the re-expressed four-variable version of the Modification of Diet in Renal Disease (MDRD) equation, 18 –20 using this updated formula: eGFR=175×(Cr)−1.154×(age)− 0.203×0.742×1.212 for black participants. The eGFR is measured in mL/min/1.73m2. A modified National Kidney Foundation classification of CKD was used, where the eGFR was classified in the three following groups: at least 60 mL/min/1.73 m2(stages 1 and 2), 45–59.9 mL/min/1.73m2 (stage 3a), and <45 mL/min/1.73m2 (stage 3b or greater). 21
Proteinuria
Urine protein was measured on a morning spot urine sample taken before the exercise stress test. The presence of proteinuria was assessed by standard urine dipstick examination. Proteinuria was considered to be present if the urine dipstick result was ≥1+ (approximately 30 mg per deciliter or greater).
Framingham Risk Score
The Framingham Risk Score has been described previously. 22 The scoring for women is calculated using a point system for total cholesterol level, high-density lipoprotein cholesterol (HDL-C), age, systolic blood pressure (SBP), diastolic blood pressure (DBP), the presence or absence of diabetes mellitus, and current smoking. The score ranges from −17 to +25, with higher scores indicating more cardiac risk factors.
We defined diabetes as either self-reported diabetes or non-fasting glucose level ≥11 mmol/L (200 mg/dL). 13 Total cholesterol was used for the Framingham Risk Score, as the blood collected was a random sample. HDL-C was assessed by the same blood analysis.
Cardiorespiratory fitness
Participants underwent a symptom-limited treadmill test using the Bruce protocol 23 with exercise ECG measurements. 24,25 Heart rate and blood pressure were measured, and a 12-lead ECG was recorded before exercise, at the end of each exercise stage, at peak exercise, and at 1-minute intervals during recovery. The test was discontinued for limiting symptoms (angina, dyspnea, fatigue), abnormalities of rhythm or blood pressure, or marked and progressive ST segment deviation. Target heart rates were not used as a predetermined end point.
The estimated cardiorespiratory fitness level was measured in units of metabolic equivalents (METs) and is an estimate of the maximal oxygen uptake for a given workload. 26,27 A MET is a measure of ventilatory oxygen consumption expressed as multiples of basal resting requirements, where 1 MET is one unit of basal oxygen consumption, which equals 3.5 mL body oxygen consumption/kg body weight/min for an average adult. The fitness level (in METs) was estimated by the speed and the grade achieved during the treadmill test. 28
Outcomes
All-cause mortality was the primary end point. A Social Security Death Index Search was performed to identify deaths up to December 31, 2008, identifying all-cause mortality and date of death.
Statistical analysis
Descriptive analyses of all variables were examined. For analysis based on eGFR, the participants were classified using a modification of the National Kidney Foundation guidelines, looking at survival based on eGFR at least 60 mL/min/1.73 m2 (stages 1 and 2), 45–59.9 mL/min/1.73 m2 (stage 3a), and <45 mL/min/1.73 m2 (stage 3b or greater). 21
Baseline characteristics stratified by eGFR were compared using one-way analysis of variance (ANOVA) for continuous variables and chi-square test for categorical variables. Stepwise Cox proportional hazards models were used to evaluate the prognostic value of eGFR (both as a continuous and as a categorical variable), Cr (both as a continuous and as a categorical variable, with Cr>1.4 compared to Cr≤1.4), and presence of proteinuria. Further adjustment was done for traditional risk factors, age, diabetes, tobacco use, total cholesterol, HDL-C, and blood pressure. Finally, assessment of the eGFR-mortality relationship by cardiorespiratory fitness was examined. The proportional hazards assumption was checked using residual plots, and tests for variable interactions were assessed.
Person-time was calculated for each woman from the date of the stress test to the date of death from any cause or December 31, 2008, whichever came first. Survival analysis was performed using Cox proportional–hazards regression models. All analyses were conducted using Stata version 9.0 (Stata Corporation, College Station, TX).
Results
Baseline characteristics
The baseline characteristics of this population have been described previously. 15 Of the 5716 women, 589 (10.3%) died over a mean follow-up period of 15.9 years. The mean age of the population was 52.5±10.8 years, and 85.5% were Caucasian. Mean Cr was 1.11±0.14 mg/dL, mean eGFR was 53.7±8.3 mL/min/1.73m2, with proteinuria noted in 117 women (2.0%). The relationship between Cr and eGFR was not linear (Fig. 1). The mean Framingham Risk Score was 5.6±5.9, and the mean cardiorespiratory fitness was 8.0±2.7 METs (Table 1).

Hypertension defined as known history of hypertension or systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg.
Diabetes defined as history of diabetes or random glucose >200 mg/dL.
Proteinuria based on spot urine dipstick; defined as present if greater than trace levels detected.
HDL-C, high-density lipoprotein cholesterol; METs, metabolic equivalents.
Women with a lower eGFR at baseline were older and were more likely to be Caucasian, hypertensive, diabetic, and nonsmokers and more likely to have proteinuria and a higher Cr. They were also more likely to have the metabolic syndrome and have a reduced fitness level, compared to women with an eGFR ≥60 mL/min/1.73 m2 (Table 1).
Outcomes
This cohort was followed for a total of 90,966 person-years. The risk of death from any cause reduced markedly among women with a higher eGFR. After adjustment for the Framingham Risk Score and cardiorespiratory fitness, there was a 3% reduction in mortality for every mL/min/1.73 m2 increase in eGFR (p<0.001). Similarly, compared to the reference category of eGFR <45 mL/min/1.73 m2, women with an eGFR of 45–59.9 mL/min/1.73 m2 were 37% less likely to die from any cause (p<0.001), and those with an eGFR ≥60 mL/min/1.73 m2 were 46% less likely to die from any cause (p<0.001), after controlling for traditional risk factors and fitness (Table 2 and Figs. 2 and 3). Proteinuria and Cr (as a continuous variable) were not independent predictors of mortality. Having a Cr>1.4 mg/dL was associated with 59% greater risk of death from any cause (p=0.025), after controlling for the Framingham Risk Score and cardiorespiratory fitness (Table 2). The hazards ratios (HRs) did not change significantly when adjusting for individual cardiac risk factors and age, in place of the Framingham Risk Score.
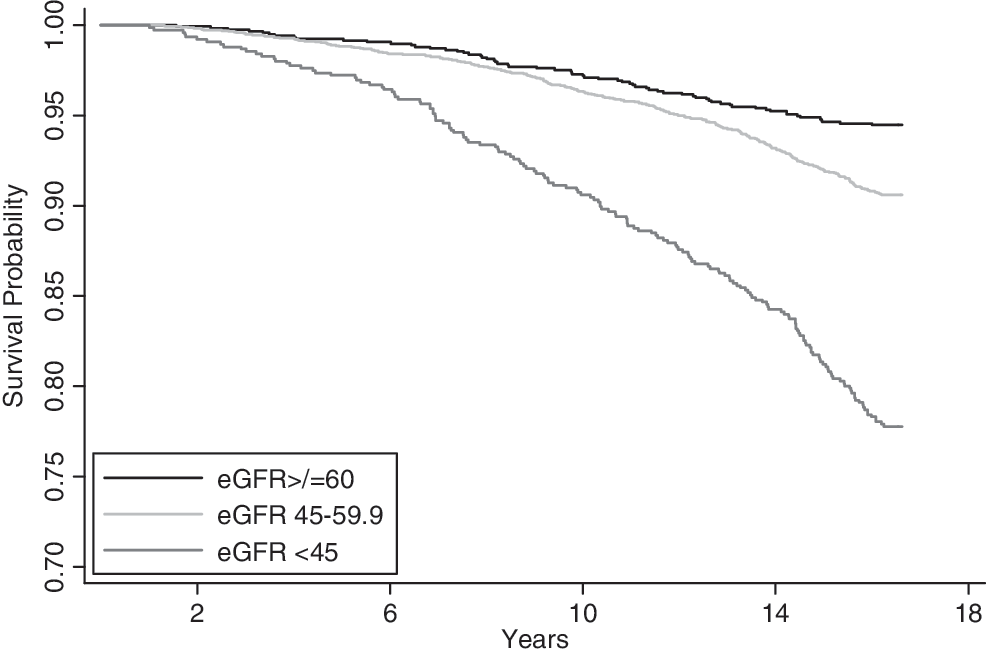
Kaplan-Meier survival curves according to the eGFR at baseline, after adjustment for traditional cardiac risk factors and cardiorespiratory fitness levels.
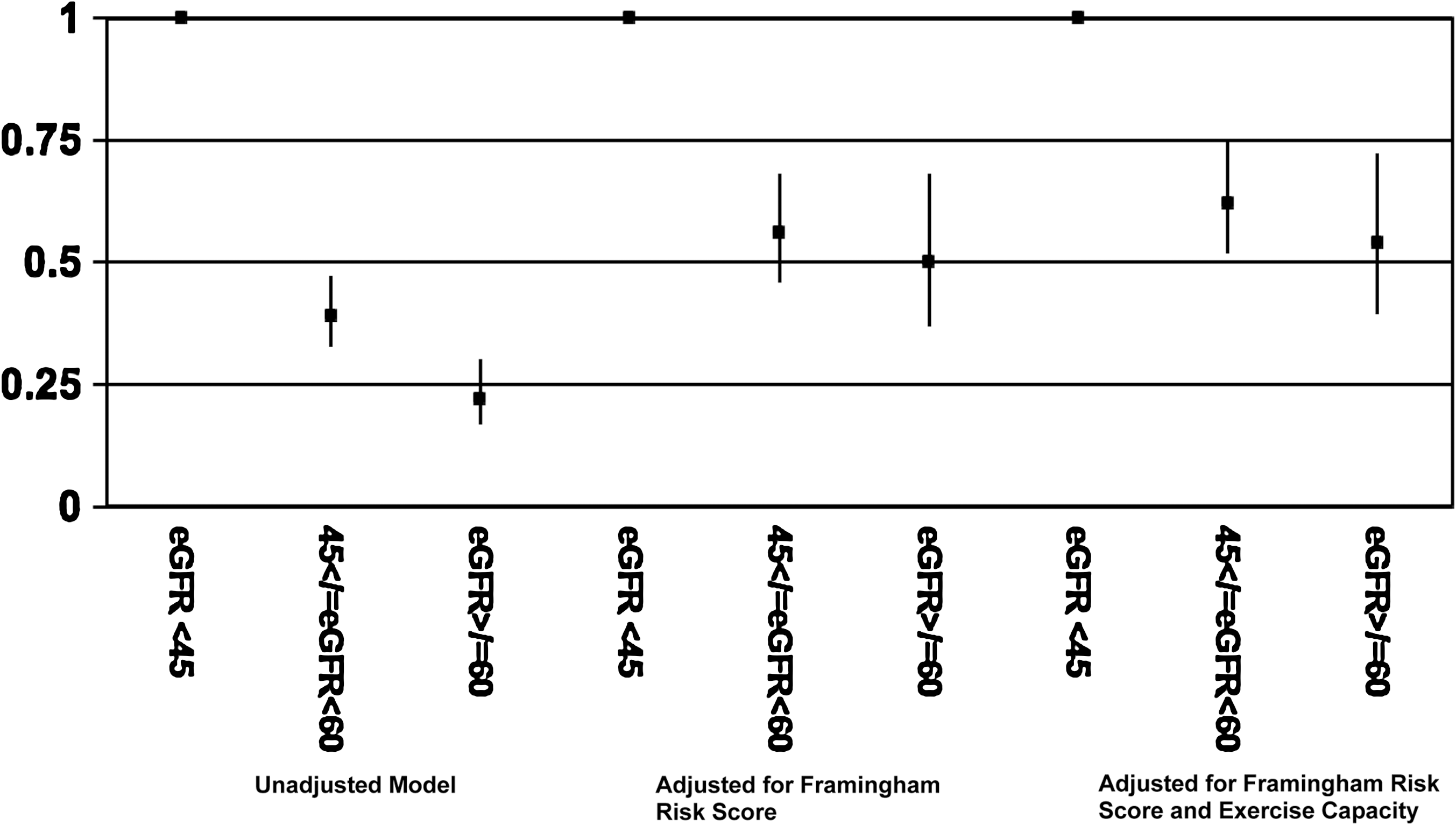
Hazard ratio (HR) of all-cause mortality in women, based on eGFR, unadjusted HR, adjusted for Framingham Risk Score, and adjusted for both Framingham Risk Score and cardiorespiratory fitness level. p<0.001 for all models at each level of eGFR.
Adjusted for Framingham Risk Score.
Adjusted for Framingham Risk Score and exercise capacity.
CI, confidence interval; eGFR, estimated glomerular filtration rate.
Cardiorespiratory fitness significantly modified the association between eGFR and mortality (p<0.001). When stratified by both eGFR and cardiorespiratory fitness, the mortality rate was highest in those with the lowest fitness level, independent of eGFR. Those with the lowest eGFR (<45 mL/min/1.73 m2) and the lowest fitness level (<5 METs) had a mortality rate of 7.6 deaths/1000 person-years, in contrast to a death rate of 0.56 deaths/1000 person-years in those with an eGFR ≥60 mL/min/1.73 m2 and a cardiorespiratory fitness level of >8 METs (Fig. 4).

Mortality rates stratified by eGFR and cardiorespiratory fitness level. For eGFR <45 mL/min/1.73m2, compared to cardiorespiratory fitness level >8 metabolic equivalents (METs) with mortality rate of 3.2/1000 person-years, mortality rate 3.8/1000 person-years for 5–8 METs (p=0.41), and mortality rate 7.6/1000 person-years for <5 METs (p<0.001). For eGFR 45–59.9 mL/min/1.73 m2,compared to cardiorespiratory fitness level >8 METs with mortality rate of 0.98/1000 person-years, mortality rate 1.8/1000 person-years for 5–8 METs (p<0.001), and mortality rate 3.1/1000 person-years for <5 METs (p<0.001). For eGFR ≥60 mL/min/1.73 m2,compared to cardiorespiratory fitness level >8 METs with mortality rate of 0.56/1000 person-years, mortality rate 1.18/1000 person-years for 5–8 METs (p=0.0.19), and mortality rate 1.69/1000 person-years for <5 METs (p=0.002).
Discussion
In this cohort of asymptomatic women with no known kidney impairment, impaired kidney function as estimated by GFR was highly prevalent. Among these women, we found that a reduced eGFR was a strong predictor of all-cause mortality independent of risk conferred by the presence of traditional cardiac risk factors and low cardiorespiratory fitness. No study to date has examined the association between the eGFR and cardiorespiratory fitness and their combined relationship with all-cause mortality. The WTH cohort demonstrates that both eGFR and cardiorespiratory fitness are independent risk factors for all-cause mortality, but there is a noted reduction of the effect of eGFR on mortality if the fitness level is high. The lower the fitness level, the higher the risk of mortality for any given level of eGFR. These findings suggest that there may be a protective effect of having a higher fitness level at baseline, independent of eGFR. Improved cardiorespiratory fitness lessened the mortality risk at all levels of eGFR.
Almost all the women in this study had a normal Cr, and only 1.8% of women had an elevated Cr (defined as Cr>1.4 mg/dL). In contrast, an elevated Cr was found in 3% of the Second National Health and Nutrition Examination Survey (NHANES II) respondents 29 and in 8.9% of Framingham Study participants. 4 When kidney function was expressed by eGFR in this cohort, the majority (79%) had grade 3 CKD or worse. The mean eGFR seen in this cohort of women is lower than seen in other population studies. 30 –32 This may be due in part to the formula used to estimate GFR, which would result in a higher eGFR when the older MDRD equation was used. 19 In addition, female gender has been shown to be associated with lower eGFR. 33 Certainly, there has been evidence that the MDRD estimation of GFR underestimates measured GFR in those with a measured GFR >60 mL/min/1.73 m2, causing an overdiagnosis of prevalent CKD when relying on the estimated GFR from the MDRD equation. 34,35 The GFR in those with a measured GFR >60 mL/min/1.73 m2 may be better estimated by using the Chronic Kidney Disease Epidemiology Collaboration Equation (CKD-EPI). 34 This was examined in our population, and it did not change our findings in any significant way, despite shifting the GFR to higher values, as would be expected of this newer equation (data not shown).
Clinicians routinely measure Cr, although Cr has not been proven to be an accurate assessment of kidney function, particularly among the elderly. 36 –38 To date, there are conflicting data about the value of Cr as a prognostic marker. Increased Cr is associated with all-cause and cardiac mortality and CV events in some studies, 2,3,5,8,29,32,39,40 whereas other studies have not replicated these findings, particularly in women. 4,41 Many of these prior studies were performed in elderly populations, 2,42 among those with known renal insufficiency, 4,8,41,42 in persons being treated for hypertension, 5,6,40 or in patients after an MI. 12 As shown in this study, the association between Cr levels and eGFR is not linear, which may explain the difference in the value of eGFR compared to Cr. Estimates of GFR have been shown to be more accurate assessments of kidney function 36 and to have important prognostic implications. 7
Mild reductions in eGFR were shown in this cohort to be associated with increased mortality, a similar finding when compared to other populations. 7,29,32,43 Many studies have also demonstrated an increase in CV mortality and CV events associated with a decreased eGFR. 7,29,30,32,43,44 In the WTH cohort, we found that for every mL/min/1.73 m2 decrease in eGFR, there was an increase in mortality of 3%, after adjusting for traditional cardiac risk factors and cardiorespiratory fitness. The WTH Project also found an inverse association with eGFR and the presence of CV risk factors, aside from its direct relationship with tobacco use and its nonrelationship with BMI.
The implications of a low eGFR go beyond the possible progression to end-stage kidney disease and requirement for dialysis. CKD is a recognized independent CV risk factor by both the AHA 45 and the Joint National Committee for Detection and Treatment of Hypertension. 46 Although the majority of women in this cohort had kidney dysfunction as shown by eGFR, none were symptomatic. Unless kidney function is appropriately assessed, women with CKD will remain unaware of their increased risk. Detection of CKD needs to go beyond assessment of Cr. This recommendation is supported by the National Kidney Foundation. The use of eGFR should be the standard, 47 but, it is still not typically reported or used in CV risk assessment despite its availability and simplicity. The most recent AHA guidelines for heart disease prevention in women recognize CKD as a risk factor for women 45 and places these women at high risk for CVD, yet eGFR remains an underused CV risk marker and is not incorporated into our traditional assessment of CV risk. 22
There are few prospective studies that include large numbers of women who represent a broad age range and are without known heart or kidney disease that have assessed the relationship between kidney function and mortality. This is the first study to show that higher cardiorespiratory fitness is associated with a reduction in the impact of CKD on all-cause mortality. The mechanism by which cardiorespiratory fitness affords this reduction in mortality remains unknown and is an area for further research.
Our study has several limitations. Measurement of Cr was based on a single measure, which may be less reliable than the mean of a number of serial measurements. In addition, we were only able to estimate the GFR, although the accuracy of the this measure has been validated. 36 Also, body fat was not directly measured in this cohort. It is possible that those with a high eGFR and higher fitness level would have a leaner body mass, as best reflected by BMI or waist circumference, but this was not seen in our population. Proteinuria was assessed by a simple dipstick method, which not sensitive for detecting mild kidney disease, and this limits the findings related to estimates of proteinuria. There was no assessment of albumin excretion in this cohort, despite this being an established predictor of CV mortality. 30 Another limitation of this study is the nature of the cohort being studied. This is a volunteer cohort of predominantly white women who were be able to walk on a treadmill. These factors may limit the generalizability of our findings to other healthy cohorts of women without previous CV disease or CKD. Nonetheless, this overselection of healthy women suggests that the prevalence of CKD in the general population of women may be higher than suggested by prior studies.
In conclusion, CKD as measured by eGFR needs to be evaluated in women and interpreted as a prognostic marker regardless of Cr levels. Our results suggest that eGFR and fitness may be useful tools to prioritize management of CV risk factors and reduce risk of mortality. Targeting these patients for cardiac risk factor modification is currently recommended by the AHA. 11 Those with CKD could potentially benefit from exercise training and physical activity, which may ultimately improve their level of fitness and possibly cause improved outcomes. 48,49 Given the increased burden of CKD and CVD worldwide, there is an urgent need to make estimates of GFR and cardiorespiratory fitness, in addition to traditional CV risk assessment, a priority in women.
Footnotes
Acknowledgments
This work was supported by grants and research support from the Sarah Ross Soter Family of Columbus, Ohio. We thank Dr. Randi E. Foraker and Dr. Joy Lewis for their insight and comments. We gratefully acknowledge the commitment of the women who participated and continue to participate in the St. James WTH Project. Their continued contribution to the study of heart disease in women is immeasurable.
Disclosure Statement
None of this work represents a conflict of interest, and the authors have no financial relationships to disclose.