
Abstract
Purpose:
The human papillomavirus (HPV) vaccine is of particular importance in American Indian/Alaska Native women because of the higher rate of cervical cancer incidence compared to non-Hispanic white women. To better understand HPV vaccine knowledge, attitudes, and practices among providers working with American Indian/Alaska Native populations, we conducted a provider survey in Indian Health Service, Tribal and Urban Indian (I/T/U) facilities.
Methods:
During December 2009 and January 2010, we distributed an on-line survey to providers working in I/T/U facilities. We also conducted semistructured interviews with a subset of providers.
Results:
There were 268 surveys and 51 provider interviews completed. Providers were more likely to administer vaccine to 13–18-year-olds (96%) than to other recommended age groups (89% to 11–12-year-olds and 64% to 19–26-year-olds). Perceived barriers to HPV vaccination for 9–18-year-olds included parental safety and moral/religious concerns. Funding was the main barrier for 19–26-year-olds. Overall, providers were very knowledgeable about HPV, although nearly half of all providers and most obstetricians/gynecologists thought that a pregnancy test should precede vaccination. Sixty-four percent of providers of patients receiving the vaccine do not routinely discuss the importance of cervical cancer screening.
Conclusions:
Recommendations for HPV vaccination have been broadly implemented in I/T/U settings. Vaccination barriers identified by I/T/U providers are similar to those reported in other provider surveys. Provider education efforts should stress that pregnancy testing is not needed before vaccination and the importance of communicating the need for continued cervical cancer screening.
Introduction
From 1996
In 2006, a quadrivalent human papillomavirus (HPV) vaccine was licensed for use in females aged 9–26 years. The quadrivalent vaccine protects against four types of HPV, two that cause the majority of cervical cancer (16, 18) and two that cause genital warts (6, 11). In 2009, a bivalent HPV vaccine was also licensed by the Food and Drug Administration (FDA) for use in females aged 9–26 years. The bivalent vaccine protects against HPV types 16 and 18. The Advisory Committee on Immunization Practices (ACIP) recommends routine HPV vaccination with either formulation for females aged 11–12 years old. Catchup vaccination is recommended for females aged 13–26 years who have not been previously vaccinated. The vaccine can be given as young as 9 years of age at the discretion of the clinician; pregnancy testing before HPV vaccination is not recommended. In 2009, a provisional ACIP recommendation allowed for vaccination of males aged 9–26 years old with the quadrivalent vaccine to reduce their likelihood of acquiring genital warts. 5 As not all types of oncogenic HPV are included in the vaccines, the ACIP recommends continued screening in vaccinated females. 6
The Indian Health Service (IHS) is the federal healthcare provider for eligible AI/AN people in the United States, with a network of IHS, Tribal and Urban Indian (I/T/U) hospitals and clinics serving AI/AN people in 35 states. The I/T/U network provides clinical services to 1.6 million of the 4.1 million U.S. AI/AN population. 7 The IHS is divided into 12 administrative regions called Areas (Fig. 1). Each IHS Area has unique tribal composition and varies in AI/AN population size and number of I/T/U facilities. All I/T/U facilities receive free vaccine through the Vaccines for Children (VFC) program for AI/AN patients < 19 years of age for all routinely recommended vaccines. Provision of vaccines recommended for adults, however, varies.

Indian Health Service Areas.
Given the high rates of cervical cancer among AI/AN women, it is particularly important to strengthen prevention efforts, including HPV vaccination. There have been studies 8 –10 examining the HPV vaccine knowledge, attitudes, and practices of healthcare providers following licensure in 2006, but none have focused on providers in I/T/U facilities. This study is the first to examine HPV vaccine knowledge, attitudes, and practices among providers working specifically with the AI/AN population.
Materials and Methods
Provider survey
Survey questions were adapted from a provider survey by Daley et al., 10 and additional questions were developed by a team of IHS and Centers for Disease Control and Prevention (CDC) epidemiologists. The 35-item survey included questions about provider demographics, knowledge of HPV and the HPV vaccine, attitudes about the care of female adolescents, current provider vaccination practices, reasons for parental refusal or deferral, perceived barriers to HPV vaccination, and cervical cancer screening practices. The survey was reviewed and pilot tested with several IHS providers before distribution. The survey was distributed to a convenience sample of I/T/U providers who were members of the targeted IHS distribution lists for certain specialties during the survey collection period. Specialty distribution lists included family practice, pediatrics, advanced practical nurse, midwives, physician assistants, maternal child health, obstetrician/gynecologist, women's health, and immunization coordinators and represented 1422 healthcare providers. Respondents accessed the survey on-line between December 2009 and January 2010 using Survey Monkey software. The provider survey responses were analyzed using SAS 9.2 (SAS Institute Inc., Cary, NC).
Provider interviews
A semistructured provider interview guide was developed to further explore topics identified in the online survey. The provider interviews included 22 questions focusing on the different types of clinic visits where HPV vaccine is administered, use of HPV vaccination education materials, and provider attitudes about the importance of genital warts. The interview questions were reviewed by the same team of IHS and CDC personnel that reviewed the online survey questions. The provider interviews were conducted in person by three team members at two IHS conferences attended by providers working in I/T/U facilities and limited to providers currently administering the HPV vaccine. The provider interviews were voluntary and took approximately 15 minutes to complete. Data for all interviews were reviewed, and a coding frame was constructed by one team member for all open-ended questions to maintain consistency.
This study and the survey instruments were approved by the IHS Institutional Review Board.
Results
Demographics
There were 268 on-line survey responses and 51 provider interviews, with responses from all the 12 IHS Areas, representing 29 states. Based on the total number of eligible providers included in the initial distribution lists, we had an estimated 35% response rate for the on-line survey. Although only 16% of the providers participating in the interview had also completed the on-line survey, provider characteristics were similar in both the survey and interview groups (Table 1). A majority of respondents were physicians, female, between 40 and 59 years old, reported a specialty of family medicine, and worked at an IHS facility. Most providers saw both adolescent and adult patients, with 91% reporting that less than half of their patients were adolescents.
Other includes licensed practical nurse/licensed vocational nurse, pharmacists, community health aide.
Other includes urgent care, emergency medicine, public health, women's clinic.
Did not ask interview participants.
Provider knowledge (provider survey)
The percentage of correct responses to the true/false knowledge questions asked in the provider survey about HPV and HPV vaccination are shown in Table 2. Overall, the majority of providers answered the questions correctly, although 46% were unaware that genital warts are not caused by the same HPV types that cause cervical cancer, and 50% did not know the correct answer or mistakenly thought that a pregnancy test should be given before HPV vaccination. Compared to other specialties, a significantly higher proportion of obstetricians/gynecologists (85%) thought that a pregnancy test should be given before vaccination.
Provider attitudes (provider survey and provider interview)
The majority of survey respondents (58%) agreed that it was hard to establish continuity of care with female adolescents. Ninety-two percent of providers reported feeling comfortable discussing issues of sexuality with female adolescent patients, and most (72%) thought that adolescents were comfortable discussing issues of sexuality with them.
A majority of the survey respondents (78%) would recommend the HPV vaccine to females aged ≥ 27 years if the vaccine was licensed and recommended for that age group. Approximately 71% of providers who see males said they would recommend the HPV vaccine to males. According to the provider interviews, very few males had requested the vaccine; some providers suggested that patients are not aware that the HPV vaccine is available for males.
When asked about HPV vaccine preference, 54% of survey respondents preferred the quadrivalent vaccine, 45% had no preference, and 1 respondent preferred the bivalent vaccine.
Although only 25% of survey respondents reported that genital warts are frequently seen in their practice, the majority of the providers who participated in the provider interviews believed it was very important for an HPV vaccine to protect against genital warts. Some of the providers interviewed stated that protection against genital warts was a selling point when recommending the HPV vaccine to their patients. Furthermore, providers thought protection against genital warts is very important to their patients but reported varying levels of patient awareness about genital warts.
Provider practices (provider survey and provider interview)
A majority of providers are vaccinating females aged 11–18 years; 48% reported providing vaccine to 9–10-year-olds. There was some variation in the age at which HPV vaccination was given, with more providers administering vaccine to the 13–18-year-old group (96%) than to the 11–12-year-old group (89%) (Fig. 2). Sixty-four percent reported providing the vaccine to females 19–26 years of age. In the interviews, providers reported that they used age to determine if a patient should receive the HPV vaccine, with some starting at 11 years as recommended and others waiting until 13 years of age to begin vaccination.
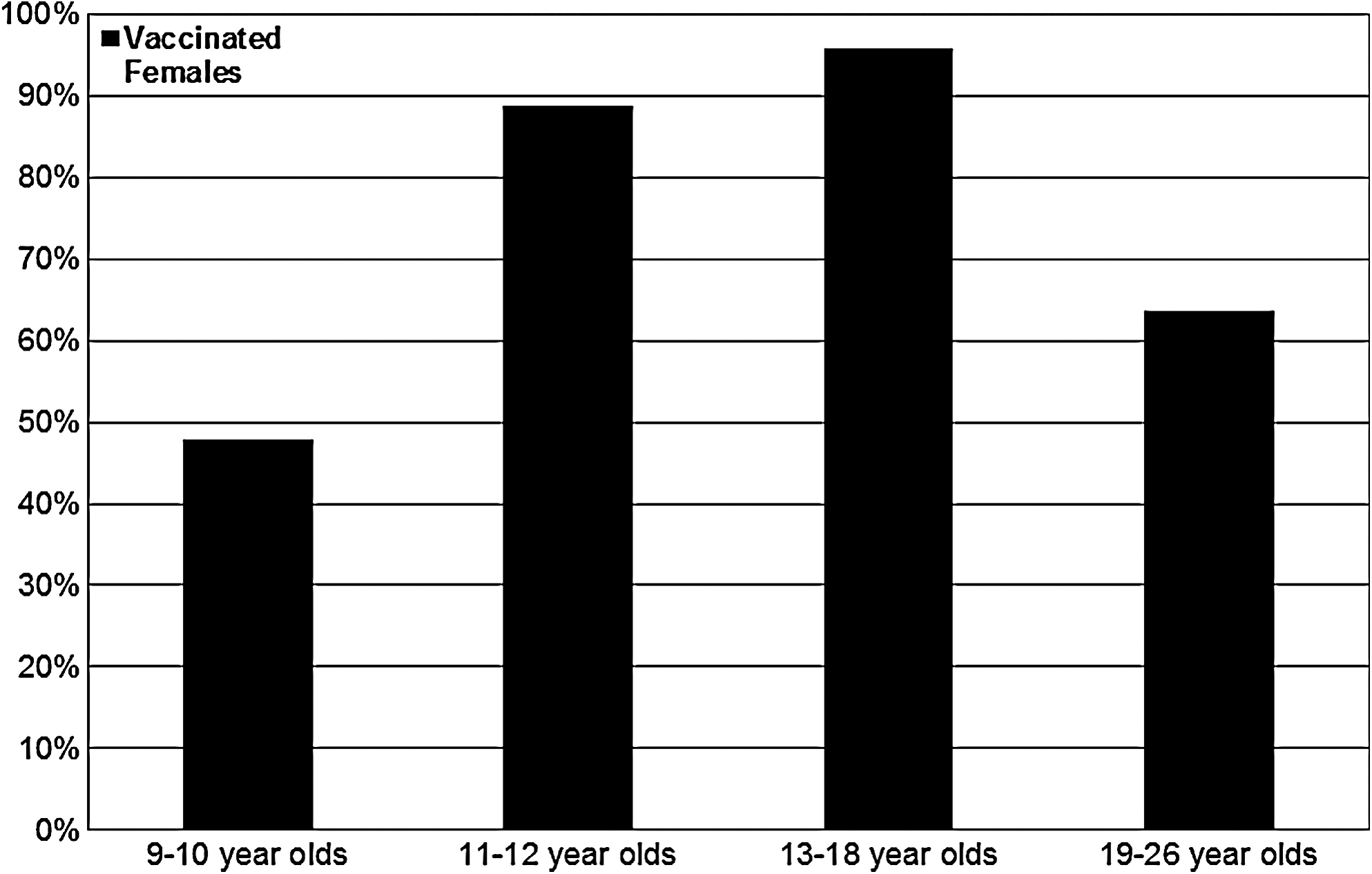
Provision of human papillomavirus vaccination among 9–26-year-old females, Indian Health Service Provider Survey, 2009.
Providers identified various reasons in the survey for not providing vaccine to the different age groups. Young age was the main reason given for not providing vaccine to 9–10-year-olds (57%), followed by the fact that the ACIP recommends vaccination starting at 11–12 years of age (29%). Among providers not vaccinating 11–12-year-olds, the main reason was the belief that the patient was too young (27%), followed by efficacy concerns (19%). For the 19–26-year-old group, the up-front costs of purchasing the vaccine and inadequate reimbursement were reasons for not vaccinating this age group (43% and 42%, respectively). Approximately 10% of providers reported efficacy concerns or the fact that the patient was already sexually active as a deterrent to vaccination in the 19–26-year-old group.
Fifty percent of providers reported purchasing HPV vaccine for females 19–26 years old, and approximately 12% of respondents participate in the Merck Patient Assistance Program, which provides vaccine to uninsured, low-income individuals. 11 Among those who do not vaccinate females aged 19–26 years, 40% reported referring patients to outside clinics for vaccination.
In the interviews, providers reported that HPV vaccination is available at several different types of clinic visits, including general wellness visits, women's health visits, adolescent/well-child visits, acute care visits, and walk-in immunization clinics, with vaccine available during the same clinic visit if requested. Some providers reported that despite their facility offering adolescent health checkups, in general, they are not actively promoted.
Barriers (provider survey and provider interview)
Providers reported several barriers to vaccinating 9–18-year-olds. Sixty-seven percent of providers reported that parent concerns about the safety of the HPV vaccine was somewhat/definitely a barrier to vaccinating. Other perceived barriers were parent concerns that vaccination may encourage earlier or riskier sexual behavior (57%) and parent opposition to HPV vaccination for moral or religious reasons (57%). Forty-one percent of respondents reported parental concerns about the efficacy of the vaccine as a barrier to vaccinating. Provider concern about adding another vaccine to the schedule or concern over time spent to discuss HPV vaccination were not considered barriers by the majority of providers, and few reported provider concerns about the vaccines safety (15%) or efficacy (12%) as barriers to providing the vaccine.
When asked in the survey to identify reasons given by parents for refusing or deferring HPV vaccination for 9–12-year-olds and 13–18-year-olds, providers reported different barriers according to patient age. Contrasted with parents of 13–18-year-olds, providers reported that parents of 9–12-year-olds are more concerned about the adolescent's initiation of sexual activity and if the adolescent is too young to vaccinate. Concerns about the safety of the vaccine (41%) and the parent feeling the vaccine is too new (39%) were the most commonly reported barriers for the 13–18-year-old group (Table 3).
Other barriers identified by providers during the interview include adolescent forgetfulness to return for subsequent doses, HPV vaccination as a low priority to patients, transportation issues, and pain while getting vaccinated.
Strategies (provider survey and provider interview)
Providers use multiple strategies to encourage patients to complete the three-dose series. Approximately 69% of providers use an electronic database or registry to track when the next dose is due, over half request that patients schedule future appointments at the time they receive the first dose, and over half record when the next dose is due on a paper-based card maintained by the patient. Additional strategies identified in the interviews included mailing letters or postcards to remind patients of upcoming appointments. Providers also reported verifying the immunization status of all patients seeking care of any kind at the clinic and using public health nurses to immunize patients in the community, including at school-based health centers.
Educational material (provider survey and provider interview)
Survey respondents identified various sources of information for HPV vaccines, including the CDC (56%), such professional organizations such as the American Academy of Family Physicians (AAFP), the American College of Obstetricians and Gynecologists (ACOG), the American Academy of Pediatrics (AAP), and ACIP. To address parental concerns about the HPV vaccine, providers in the interview reported they use the Vaccine Information Statement (VIS) and various pamphlets. Some providers stated the literacy level of the available materials may not be appropriate for the AI/AN population. Suggestions from the provider interviews for materials include more posters and pamphlets explaining HPV vaccine that were “less text heavy,” had more pictures, and were written at an appropriate literacy level.
Cervical cancer screening (provider survey)
Thirty-six percent of providers reported routinely discussing the importance of initiating or continuing screening with vaccinated patients or their parents, whereas 38% reported having these discussions often. Twenty-six percent of providers discussed screening either sometimes, rarely, or never. When asked how the determination is made to start routine cervical cancer screening, nearly 80% responded by the onset of sexual activity, whereas 63% reported age of the patient as a criterion for initiating screening. The responses were not mutually exclusive (data for screening not shown).
Discussion
Findings from our survey were similar to those found in previously published studies. HPV vaccine recommendations appear to have been widely adopted by I/T/U providers, and providers are less likely to recommend the HPV vaccine to younger patients than to older patients. 10,12 –15 This reluctance to vaccinate younger patients may prevent adolescents from receiving the full benefit of the vaccine, as the vaccine ideally should be administered before potential exposure to HPV through sexual contact. 6 Consistent with past studies, our study also found providers preferred the quadrivalent vaccine over the bivalent vaccine. 12,13,16
Overall, I/T/U providers were knowledgeable about HPV and HPV vaccination. Nevertheless, additional education about HPV vaccination and pregnancy tests is needed, as nearly half of all providers and most obstetrician/gynecologist providers thought that a pregnancy test should precede vaccination. Although HPV vaccination is not recommended during pregnancy, a pregnancy test is not needed before vaccination, 6 and studies have found no negative effects on pregnancy outcomes in women who received HPV vaccine during pregnancy. 17 –19 Provider beliefs that pregnancy testing is required before vaccination could present a barrier to adolescents wishing to be vaccinated. Furthermore, more than a third of providers were unaware that the HPV types that can cause genital warts are different from those that cause cervical cancer, which could cause misinformation to patients about the protection provided by the quadrivalent vs. the bivalent vaccine. 20
Barriers to HPV vaccination identified by I/T/U providers in this survey are similar to barriers identified by providers serving other groups. 8,10 Providers reported that vaccine safety is a concern among parents of AI/AN adolescents. In addition, providers reported that some parents resist HPV vaccination on the grounds that their children are not sexually active and that provision of the vaccine might somehow encourage riskier sexual behavior. Further dissemination of educational materials to address parental safety concerns and emphasizing the HPV vaccine as a cancer prevention tool may help alleviate some of these barriers. Whereas funding is not a barrier for AI/AN adolescent vaccination, it is a barrier to vaccination for 19–26-year-olds, similar to what was found in other populations. 21,22 Although healthcare reform may help to address such inequities, the chronic underfunding of IHS may mean this continues to be an issue. 23
Despite the barriers reported by providers, HPV vaccine coverage reported by I/T/U facilities is high. According to the CDC's 2009 National Immunization Survey–Teen (NIS-Teen), coverage for the general U.S. population with ≥ 1 and ≥ 3 doses of HPV was 44% and 27%, respectively 15 ; I/T/U facilities reported coverage for doses 1, 2, and 3 among females 13–17 years old at 72%, 57%, and 40% as of March 2010. 24 In addition, the NIS-Teen found that coverage for one dose of HPV for NHW adolescents was 44% (95% confidence interval [CI] 41.8-46.1%) compared to 52% (95% CI 39.0-65.2%) for AI/AN adolescents. 15 Although both the I/T/U data and CDC data suggest that providers are successfully reaching AI/AN adolescents, completion of the series remains a challenge.
Provider responses regarding cervical cancer screening practices suggest a need for providers to encourage patients receiving HPV immunization and their parents to adhere to screening recommendations. The survey was administered shortly after ACOG updated cervical cancer screening recommendations, which included initiating screening at age 21 without regard to onset of sexual activity. 25 Although the updated recommendations were released only recently at the time of the survey, provider responses indicated a reliance on sexual activity as a guide for initiating screening. Promoting education for providers to apply the updated recommendations should decrease the number of unnecessary screenings and expose fewer young women to risks of treatment for cervical lesions likely to regress spontaneously.
Although high HPV vaccine coverage among the AI/AN population can largely be attributed to the VFC program, there are also several strategies employed by I/T/U facilities that likely contribute to high coverage rates. The IHS supports an electronic health record called Resource Patient Management System (RPMS) that includes an immunization component facilitating the recording and tracking of all immunizations. The system not only generates provider reminders, but also supports patient reminder/recall activities and allows sites to monitor immunization coverage levels in the community. In addition, many I/T/U facilities employ public health nurses who track and follow up with patients due for immunizations and, in some cases, even provide vaccinations outside of the clinical setting. Given the lower third dose coverage, promoting use of the reminder/recall functions in the RPMS immunization component and further dissemination of follow-up strategies are particularly important.
Limitations
Our survey and interviews are subject to several limitations. A complete list of all providers in the I/T/U healthcare facilities does not exist, and, therefore, we could only estimate a response rate. However, it is not uncommon for HPV vaccine acceptability surveys and other surveys to use such a convenience sample. 26 Almost two thirds of all published articles about HPV vaccine acceptability used convenience samples, and a response rate was not reported or calculable in over 90% of them. 27 Another limitation is that the provider surveys and interviews were self-reported data and subject to reporting bias. Similarly, selection bias is possible in that nonrespondents may have different knowledge, attitudes, and practices about HPV vaccination compared with our respondents.
Conclusions
HPV vaccination will play a critical role in addressing the increased burden of cervical cancer experienced by AI/AN women. Understanding barriers to vaccination and strategies to overcome these barriers is essential. Although HPV vaccination alone is not sufficient to address the disparities in cervical cancer incidence and mortality experienced by the AI/AN population, it is an important strategy. As evidenced by the relatively high HPV vaccination coverage levels, I/T/U facilities have made considerable progress in increasing the uptake of vaccine in this population. Further dissemination of AI/AN educational materials, including CDC-developed preteen immunization materials and brochures on genital warts and HPV, may help to address some of the barriers identified by providers in our survey. 28 Additional education for providers about HPV and HPV vaccination may help eliminate unnecessary obstacles to HPV vaccination. Increasing adolescents' access to services generally through the implementation and promotion of the AAP/AAFP-recommended routine Adolescent Health Check Up, implementing standing orders, promoting recommended vaccines, using the reminder/recall functions in the RPMS, and expanding provision of vaccines to nonclinical settings may help further increase coverage levels and ensure series completion. Finally, addressing financial barriers that prevent the provision of HPV vaccine to older females are needed. Increasing funding to IHS to support healthcare reform initiatives, such as ensuring the provision of all ACIP-recommended vaccines, will be important to ensure the availability of HPV vaccine to women 19–26 years of age.
Footnotes
Disclosure Statement
The authors have no conflicts of interest to report.