
Abstract
Background:
A simpler approach to cervical cancer screening could increase coverage, thus reducing cervical cancer mortality in the United States. Self-collection of specimens for screening tests may be one such approach. The aim of this study was to assess the acceptability of a self-lavaging device (Delphi Screener™, Scherpenzeel, The Netherlands) for cervical cancer screening. Self-lavage specimens have been shown to have equivalent sensitivity for detection of high-grade cervical intraepithelial neoplasia (CIN) when coupled with high-risk human papillomavirus (HPV) tests as clinician-collected specimens with cytologic review.
Methods:
Low-income women (n=198) who had recently received cervical cytologic testing in one of three participating clinics in New York City enrolled; 197 self-lavaged. Women answered open-ended and closed-ended questions on ease of use, level of comfort with the self-lavage and the pelvic examination, and future screening preference.
Results:
Ninety-six percent of women reported they were very/somewhat comfortable self-lavaging compared to 47% very/somewhat comfortable with the clinician collecting a specimen during a pelvic examination (p<0.001). The majority (79%) would prefer self-lavage the next time they need to be screened; only 8% would prefer pelvic examination by a doctor, and 14% had no preference. The main reasons for preferring self-lavage centered on convenience and comfort.
Conclusions:
Self-lavaging was highly acceptable to women in this study. Self-collection of specimens has the potential to simplify screening and reduce logistical barriers for many women, which could increase overall coverage of cervical cancer screening.
Introduction
As part of Healthy People 2020,
Factors that could affect cervical cancer screening uptake include financial and logistical barriers as well as psychosocial barriers, such as embarrassment from undergoing a pelvic examination for a clinician-obtained cytologic smear, the current U.S. standard of care. The introduction of self-collected cervicovaginal specimens for cervical cancer screening could reduce a number of these barriers, especially for women with limited access to medical care. We evaluated the acceptability of a self-lavaging device, the Delphi Screener™ (Scherpenzeel, The Netherlands) for cervical cancer screening among low-income women in New York City. The Delphi Screener is a plastic device, similar to a large tampon applicator, containing 5 mL of phosphate-buffered saline (PBS). 6 –8 A previous study, implemented in The Netherlands, showed that self-collected Delphi Screener specimens had equivalent sensitivity for detection of high-grade cervical intraepithelial neoplasia (CIN2+) when coupled with high-risk human papillomavirus (HPV) tests as clinician-collected specimens with cytologic testing (34 of 37 vs. 31 of 37, respectively, p=0.5). 6 The objective of the current study was to compare women's preferences and reports on quality of experiences using the self-lavaging device compared to clinician collection of specimens during a pelvic examination for cervical cancer screening.
Materials and Methods
We enrolled women who received standard cervical cancer screening at three clinics within the Ambulatory Care Network of the New York Presbyterian Hospital. The three clinics provide services to different populations of women: the Family Planning Clinic provides contraceptive services to young, reproductive-aged women, Associates in Internal Medicine provides primary care services to middle-aged women (mean age of 45), and the Infectious Disease Clinic provides HIV care services to HIV-positive women of all ages. All three public clinics provide cervical cancer screening services to women with Medicaid, the AIDS Drug Assistance Program, or no insurance.
Recruitment and eligibility
Clinicians from participating clinics distributed fliers to women receiving cervical cancer screening from September 2008 to August 2009. During a visit that included a pelvic examination with cytologic smear (Pap test), women were asked for verbal consent to be contacted by study staff. Study staff phoned a convenience sample of women who verbally consented to being contacted during their pelvic examination visit and scheduled a study visit or recorded reasons for refusal or ineligibility. Staff purposively enrolled half of the women with normal cytology and half with atypical squamous cells of undetermined significance (ASCUS) or worse.
To be eligible, women had to be ≥18 years, scheduled within 1–3 months after their initial cytologic smear from a pelvic examination, reading comfortably in English or Spanish, and not currently breastfeeding or pregnant. All participants provided written informed consent. Study materials were bilingual (Spanish and English) and were pretested among nine women. The study was approved by Columbia University's Institutional Review Board and is registered with
Study procedures
During the study visit, interviewers brought women to a private room for informed consent. Next, interviewers showed participants the device and administered a preuse paper questionnaire that included open-ended, closed-ended, and visual analog scale (VAS) questions on anticipated use and comfort. Women then received a sealed, sterile Delphi Screener with pictorial user instructions (Fig. 1) to use on their own once the interviewer left the room. Interviewers returned to the private room when the women had completed self-collection. Finally, participants responded to a second interviewer-administered questionnaire on demographic, sexual history, and postuse acceptability questions that also included open-ended, closed-ended, and VAS questions. Women responded to VAS questions, by marking an X on a 10-cm line between two extremes, such as very easy and very difficult, after the interviewer read the question aloud. The lines included tick marks at 0, 5, and 10 cm to act as visual anchors.
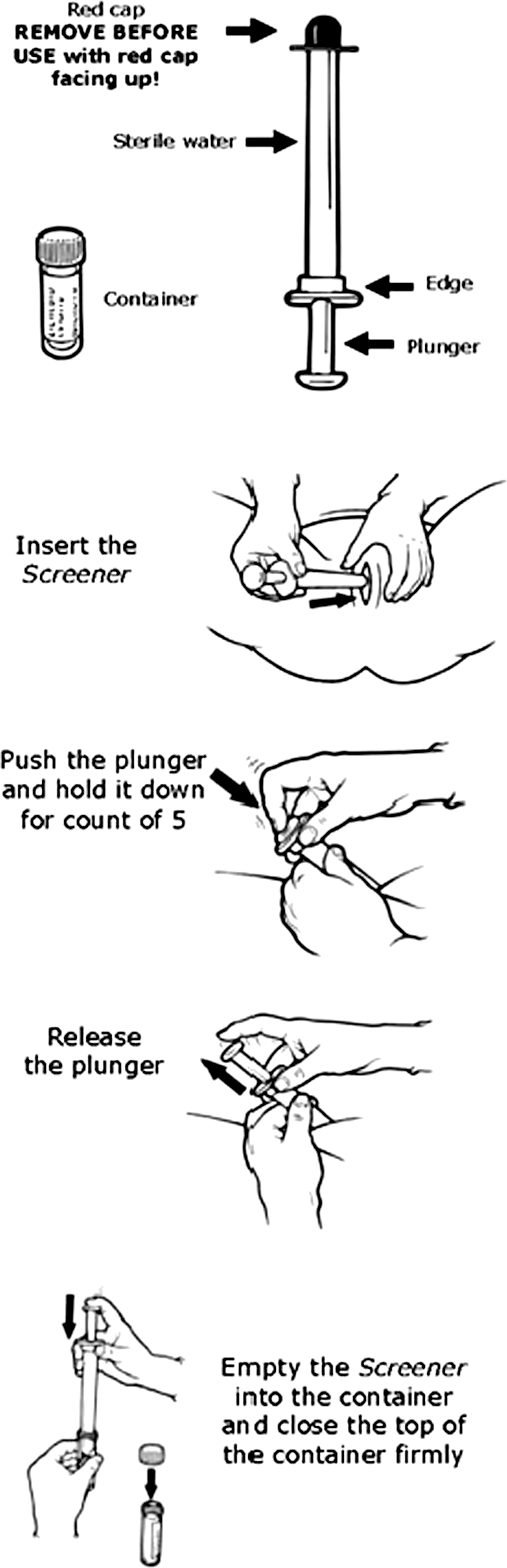
Abbreviated pictorial explanation of how to use the Delphi Screener™.
Measures
We measured acceptability both before and after use of the device in three ways. First, women responded to VAS questions on ease of use, understandability of instructions, discomfort experienced during the last pelvic examination and self-lavaging, and future screening preference coded as continuous variables to the nearest milimeter. Second, women responded to closed-ended questions about comfort and future preferences. Third, women answered open-ended questions about overall impressions of the Delphi Screener and reasons for stated preferences.
Analysis
We present proportions for precoded and thematically coded open-ended measures and medians with interquartile ranges (IQR) and histograms for VAS responses. We compared VAS responses before and after use as well as comfort with type of method collection using paired Wilcoxon rank sum tests, as Kolgorov-Smirnoff tests showed that all VAS distributions were nonparametric. We compared precoded measures on comfort with self-lavage and the pelvic examination using the McNemar's exact test. Finally, we compared responses by characteristics hypothesized to influence acceptability, including age, education, race/ethnicity, index cytology result (normal/abnormal), index clinic, parity (none vs. ≥1 births), menopausal status, recent sexual activity, use of home pregnancy tests, and tampon and vaginal medication use. We used the Fisher's exact test to compare categorical variables and the Kruskal-Wallis test to compare continuous variables.
Results
Of the 5509 women who had received cervical cancer screening during recruitment months, we invited 540 to participate; 202 (37%) declined, 122 (23%) missed scheduled appointments, 18 (3%) were ineligible, and 198 (37%) enrolled. The main reasons reported for declining participation were lack of time (48 of 202, 24%), did not like the idea of the study (n=31, 15%), not interested in hearing about the study (n=29, 14%), hung up the phone (n=29, 14%), or did not like the idea of self-sampling (n=26, 13%). Only 1 woman was not able to self-lavage because of obesity, leaving 197 women who self-lavaged and responded to acceptability questions. Most participants were Latina (84%) or African American (13%) (Table 1), a reflection of the overall clientele of participating clinics.
Column percentages are presented for the total, and row percentages are presented for preferences.
Fisher's exact test p-values.
Ease of use
Women generally expected the Screener to be easy to use, with clear instructions. VAS responses for ease of use and following instructions were all<1 cm on the 10-cm scale (with 0 being very easy) (Table 2). Reports for ease of use increased after use, with a median change of 0.2 cm (p<0.001). Only two women (1%) reported that instructions were unclear. Twenty-three (12%) women needed two devices because of a failed attempt with the first device. The main reasons were related to defects with the device (n=16), which led to changes in the manufacturing processes for next-generation models. Only 7 (4%) women used two because of difficulties with use, 6 released the liquid without full insertion, leaking it onto the table, and 1 took a second specimen to increase the amount of fluid collected. An additional 24 women (12%) asked staff if they had collected enough fluid after use.
Paired Wilcoxon rank sum test.
IQR, interquartile range.
Comfort
Women generally anticipated that the Delphi Screener would be comfortable to use, with a median of 2.2 cm (where 0=very comfortable) on the 10-cm VAS, and reported even higher comfort after use (median 0.4 cm, p<0.001) (Table 2). Women reported neutral levels of comfort with the pelvic examination (median of 4.9 cm both before and after self-lavage). Comfort with the pelvic examination exhibited more variability than self-lavage (Fig. 2). Comfort with self-lavage was significantly higher than with the pelvic examination (p<0.001). Almost all women (96%) reported they were very/somewhat comfortable with the self-lavage compared to 47% with clinician collection (p<0.001).

Density histograms of visual analog scale (VAS) responses to amount of discomfort experienced with pelvic examination and use of Delphi Screener. (0=very little/10=very much).
As only 4% of women reported being somewhat uncomfortable and 0% very uncomfortable, characteristics associated with comfort levels compared reports of very comfortable to somewhat comfortable. Women whose index cytology was normal were more likely to report being very comfortable with the Screener compared to women with abnormal cytology results (88% vs. 76%, p=0.04). Similarly, women with ≥1 births were more likely to report being very comfortable using the Screener than women with no births (86% vs. 74%, p=0.08). This pattern was also reflected in VAS measures before use, with no differences by parity after use (data not shown). Median anticipated comfort with self-lavage was 2.0 cm for women who had had sex in the last month, 1.6 cm in the last year, and 4.9 cm more than 1 year ago (10=very uncomfortable, p=0.05). However, no differences were found after self-lavage by sexual activity (p=0.71). Women who had ever inserted vaginal medication were also more likely to be very comfortable using the Screener than women who had never inserted vaginal medication (84% vs. 74%, p=0.09).
Women with less than a high school education were more likely to report being very comfortable with the last pelvic examination than women with a high school diploma or some college (30%, 24%, 10% respectively, p=0.03). Education was similarly associated with reported comfort with the pelvic examination in the VAS data (p=0.10). No differences in comfort with the Screener or the pelvic examination were seen by age, race/ethnicity, menopausal status, current tampon use, or ever use of home pregnancy test.
Future screening preferences
Most women (79%) would prefer to self-lavage for future screening; only 8% would prefer a pelvic examination, and 14% had no preference. These results were confirmed with VAS measures (p<0.001) (Table 2). The only characteristic associated with this preference was race/ethnicity, with African American women showing a stronger preference for self-sampling in the future than Latinas (92% vs. 78%, p=0.04) (Table 1).
Two main themes for self-lavaging preference were identified in open-ended responses. The first theme centered on comfort. Among women who preferred self-lavaging in the future (n=155), reasons cited were greater comfort (63%), less pain or discomfort (17%), more privacy (12%), and less stress or embarrassment (7%). For example, 1 woman stated, “It's so comfortable. You can do it at home and you don't have someone else going into your vagina.” Another woman reported, “It is intimidating when you go to the doctor. It is comfortable when you have privacy.” The second theme centered on convenience and simplicity. Women said it was easier (32%), faster (14%), could be done at home (5%), and could be done on one's own time (5%). For example, 1 woman said, “I avoid going to the doctor, as it is difficult with kids.” Another woman reported, “I think this Screener is a great idea. It's hard to take time off to go to the doctor's office all the time. This would be great because it would fit right into my busy schedule.”
For women who preferred the pelvic examination (n=15), the main theme centered on the benefit of seeing a clinician. Women reported feeling more secure (n=4) or more comfortable with the doctor (n=4), that the doctor is likely to make fewer mistakes (n=4), can take care of problems right away (n=4), and can answer questions (n=4). For example, 1 woman explained, “I would be able to ask questions, and if you need a prescription, it's easier to have a professional there.” Another woman stated, “I am used to the doctor doing that. They are professional and I am not.”
Discussion
Most women in this study found self-lavaging with the Delphi Screener easy and highly acceptable; over three quarters would prefer self-sampling with the Screener over a pelvic examination for future screening. Similarly, in a study in The Netherlands in which 91 women used the Delphi Screener at home, 75% reported preferring using the Screener to the pelvic examination for future screening with an HPV test. 7 A study among 89 women in Italy who used the Screener and underwent a pelvic examination also found that 78% prefer the Screener for future screening with an HPV test. 8 These results are in contrast to a study conducted in New York City among a clinic population similar to the current study, which found that only 32% of women preferred self-collection to the pelvic examination. 9 However, this study compared self-collection of a vaginal swab rather than a self-lavage to the pelvic examination 9 ; self-lavage may be more acceptable. The Italian study found a stronger preference for self-lavage than for self-collected brush. 8 Regardless of the exact estimate, a sizable proportion of women prefer self-collection over clinician collection in both clinical and home settings.
Evidence has shown that women who do not get screened regularly are at increased risk for cervical cancer. 10 Further, randomized control trials (RCTs) have shown that offering underscreened populations the opportunity to self-collect specimens at home increases screening uptake. 11 –13 An RCT among women who had not responded to scheduled invitations for cervical cancer screening in The Netherlands, for example, found that 27% of 26,886 women returned self-collected specimens using the Screener at home compared to 17% of 277 women who responded to letters to attend clinic appointments. 12 A pilot study among an underscreened population in Mississippi found higher response rates among women who chose self-sampling at home with a device similar to a tampon over those who chose referral to a doctor (80% vs. 40%, respectively). 14 Clearly, self-sampling, particularly in home settings, coupled with mail-in or clinic dropoff of specimens could increase screening uptake in underscreened women.
Nevertheless, some women (8% in our study) prefer to be examined by a clinician. A small qualitative study in London among Muslim women, a group thought to have particularly negative perceptions of the pelvic examination, 15 found women hypothetically preferred going to a doctor to self-swabbing or self-lavaging. 16 Further, although women in our study reported less comfort with the pelvic examination than with self-sampling, they reported neutral levels of discomfort with clinician-collected specimens. Women with less education had lower rates of discomfort with the pelvic examination than women with a high school diploma or greater. The study conducted in New York City among low-income women from similar clinics similarly found that less educated women prefer clinician collection over self-collection. 9 In both studies, fear of making mistakes during self-sampling was cited. Some women prefer having a doctor perform the test, and self-sampling should never completely replace the pelvic examination.
The consistency of responses among precoded questions, VAS measures, and open-ended questions is a study strength that suggests high validity of our acceptability measures. However, the study has some limitations. Although the VAS data were internally consistent, interpreting the significance of differences in centimeters can be difficult. Nevertheless, these data clearly indicate the direction of preferences. Self-reported acceptability measures may also have been affected by social desirability bias. Women had experienced a pelvic examination 1–3 months before the study visit; thus, reports on this experience may have been subject to recall bias. Additionally, women who enrolled in the study may have been predisposed to self-sampling, resulting in overestimated acceptability measures. About one quarter of refusals were potentially related to perceptions of self-collection, although only 13% of refusals explicitly cited this as a reason for nonparticipation. However, the RCTs of self-collected vs. clinician-collected specimens suggest acceptability for self-sampling is higher than clinician-collected sampling for many women. 11,12 Finally, we used a convenience sample of women, rather than a random sample, so our results may not be representative.
Conclusions
Introducing self-sampling as a cervical cancer screening option in the United States has the potential to expand coverage to the targeted 93%. 1 The Delphi Screener is one self-sampling modality to consider introducing into programs, given its high acceptability, as shown in this and other studies, 7,8,12,13,17 and comparable sensitivity for CIN2+ when combined with HPV testing. 6 Some evidence suggests the sensitivity for HPV may be slightly lower for self-collected specimens compared to clinician-collected specimens, 18 although other evidence suggests sensitivity is comparable. 19 Self-sampling should most likely be provided as an option for women for whom provider collection is a barrier. Introduction of self-sampling would require effective follow-up strategies for women with abnormal results to ensure improved performance of screening programs.
Footnotes
Acknowledgments
We thank Herjan Coelingh-Bennink, René Hol, Maarten Wiegerinck, and Marloes Voll from Delphi Bioscience for their input on study design and Irene Raju from Columbia University for impeccable study implementation.
Disclosure Statement
Delphi Bioscience funded this study. Delphi staff commented on study design and preliminary results. Study investigators made all final decisions for design, analysis, and presentation of results independently. None of the investigators have any financial interests in Delphi Bioscience. No competing financial interests exist.