
Abstract
Objectives:
To quantify the change in work productivity and activities of daily living in North American women with heavy menstrual bleeding (HMB) treated with estradiol valerate/dienogest (E2V/DNG; Qlaira®/Natazia®) compared to placebo.
Methods:
Women in the United States and Canada, aged 20–53 years with an objective diagnosis of HMB and no recognizable anatomical pathology, were treated with E2V/DNG or placebo for seven cycles (196 days). Main outcome measures included work productivity (i.e., productivity while at work) and activities of daily living measured using a modified Work Productivity and Activity Impairment Questionnaire (mWPAI) on a Likert scale from 0 to 10 (higher values denote higher impairment levels).
Results:
In both countries, significant improvement was observed between baseline and end of treatment in work productivity and activities of daily living impairment. The improvements in work productivity and activities of daily living with E2V/DNG treatment relative to placebo ranged from 37.2% to 39.2% across both countries. Monthly gains due to E2V/DNG treatment (net of placebo improvement) associated with improvement in work productivity were estimated to be US$80.2 and Can$70.8 (US$58.5) and those associated with improvement in activities of daily living were estimated to be US$84.9 and Can$73.5 (US$60.7).
Conclusions:
E2V/DNG was shown to have a consistent positive impact on work productivity and activities of daily living in U.S. and Canadian women with HMB. In addition, these improvements in work productivity and activities of daily living were associated with a reduction in HMB-related monetary burden compared to the placebo group.
Introduction
Heavy menstrual bleeding (HMB) is objectively defined as menstrual blood loss (MBL) of 80 mL or more per menstrual period. 1 However, because routine objective measurement of MBL is impractical and rarely undertaken except in clinical trials, treatment in practice is usually based on a woman's perceived (or subjective) MBL as being excessive enough that it interferes with her physical, social, emotional, and material quality of life. 2 Estimates of HMB prevalence vary depending on whether menstrual blood is determined objectively or subjectively—studies using objective assessment of MBL suggest prevalence rates between 4% and 14%, while those using subjective methods suggest higher prevalence rates between 20% and 52%. 2 The 12-month subjective incidence rate of HMB was reported as 13.3% in a U.S. cohort of women aged 18–64 years. 3
Although mortality or serious complications from HMB are rare, the burden of HMB on health-related quality of life (HRQOL) may be worse than with other chronic conditions, such as irritable bowel syndrome and type 2 diabetes. 4 –7 In addition, over 40% of women with physician-diagnosed HMB have anemia (i.e., hemoglobin level less than 12 g/dL). 8 HRQOL impairment due to HMB, with its associated increases in primary care consultations and specialist referrals, could give rise to a substantial economic burden. 9,10 Women with HMB also bear the burden of out-of-pocket expenses that are incurred for excess sanitary products and pharmaceuticals, which amount to US$333 per affected woman per year, 4 or the equivalent of 1% of U.S. median annual earnings for a woman. 11 Conservative estimates suggest direct and indirect annual economic costs of about $1 billion and $12 billion, respectively. 12
Treatment options for HMB consist of a range of pharmaceutical therapies and surgical interventions. 13 –15 The levonorgestrel-releasing intrauterine system, antifibrinolytic drugs (e.g., tranexamic acid), nonsteroidal anti-inflammatory drugs, progestins, and combined oral contraceptives are treatment options in the absence of organic pathology. Surgical treatments, such as hysterectomy or endometrial ablation, are generally recommended only for women who do not wish to preserve their fertility (i.e., no desire to conceive) or for whom medical treatment has failed or is intolerable. 16 Although hysterectomy eradicates HMB, it is associated with surgical risks that may have significant social and economic cost implications. 17 Endometrial ablation may be considered a less invasive surgical alternative to hysterectomy, but it does not eliminate the short- or long-term risks associated with surgery 18,19 and may not eradicate HMB in the long term. 20
Estradiol valerate/dienogest (E2V/DNG; Qlaira®/Natazia®, Bayer Healthcare, Berlin, Germany) is the first oral contraceptive approved for the treatment of HMB in women without organic pathology. The research consisted of two identically designed randomized, placebo-controlled, double-blind studies—one conducted in North America and the other in Europe and Australia. 21,22 These studies demonstrated that E2V/DNG was highly effective compared to placebo in reducing MBL, and that the reduction in MBL was accompanied by significant improvements in hemoglobin, hematocrit, and ferritin levels. Alongside these trials, the impact of treatment with E2V/DNG on HMB-related impairment of work productivity and activities of daily living was also prospectively assessed. In this paper, we present work productivity and activities of daily living outcomes from the North American study. Respective data from the Europe and Australia study are presented elsewhere. 23
Materials and Methods
A joint U.S. and Canadian multicenter double-blind, randomized, placebo-controlled phase III trial was conducted to assess the efficacy and safety of E2V/DNG treatment in patients with HMB over seven 28-day treatment cycles (196 days) compared with placebo. 21 Women ≥18 years with HMB, prolonged menstrual bleeding, frequent menstrual bleeding, or a combination of these, and without organic pathology, were eligible for inclusion. A normal endometrial biopsy was required from all women within 6 months before study entry or at worst, mild, simple endometrial hyperplasia. Those with uterine pathology that could be associated with heavy menstrual bleeding were excluded following transvaginal ultrasound assessment.
The E2V/DNG treatment cycle comprised E2V 3 mg on days 1–2 (1 mg of E2V is equivalent to 0.76 mg of estradiol), E2V 2 mg/DNG 2 mg on days 3–7, E2V 2 mg/DNG 3 mg on days 8–24, E2V 1 mg on days 25–26, and placebo on days 27–28. A full description of this trial and primary outcomes have been reported in detail elsewhere. 21 In brief, the study was approved by local institutional review boards and was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonization on Good Clinical Practice. All patients gave written informed consent and received compensation for participation in the trial. The study comprised 37 centers in the United States and 10 centers in Canada, with 190 patients in total (United States, 160; Canada, 30); 120 women were given E2V/DNG and 70 received the placebo. The primary efficacy variable was the proportion of women with a complete response (i.e., restoration of completely normal menstruation) during a 90-day on-treatment efficacy interval versus a 90-day run-in baseline interval; based on the presence and intensity of MBL as documented in electronic diaries and quantification of blood loss through hemoglobin extraction from used sanitary protection (alkaline hematin method). Complete response was strictly defined based on a composite of eight criteria. 21
Work productivity and activities of daily living were measured with a modified version of the Work Productivity and Activity Impairment: General Health Questionnaire (WPAI:GH). The original questionnaire is available from
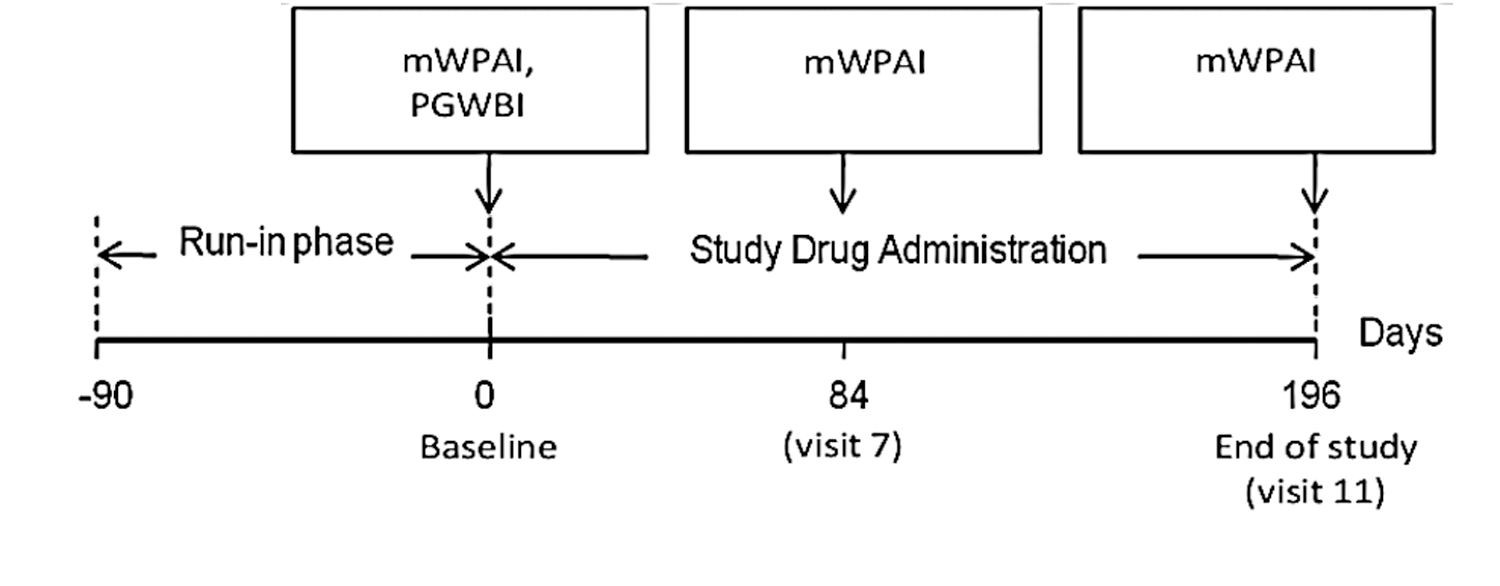
Clinical study flow. mWPAI, Modified Work Productivity and Impairment Questionnaire; PGWBI, Psychological General Well-Being Index.
Consistent with the WPAI scoring manual, 25 a direct relationship was assumed between work productivity or activities of daily living impairment and the Likert Scale response from 0 to 10 in the calculation of the impairment value. For example, a response of 1 on the Likert Scale was assumed to be equivalent to a 10% work productivity reduction or activities of daily living impairment, and a response of 9 was assumed to be equivalent to a 90% productivity reduction or activities of daily living impairment. Total impairment of work productivity or activities of daily living due to HMB would be a response of 10 on the Likert scale. Thus, a patient having no work productivity or activities of daily living impairment due to HMB would have a response of 0 on the Likert scale. An individual reporting work productivity or activities of daily living impairment of 3 at baseline and 2 at the end of treatment would thus have a 10% point reduction in work productivity or activities of daily living.
In our study, work productivity refers to presenteeism, that is impairment while at work, or reduced on-the-job productivity. To provide estimates of baseline values appropriate for accurate statistical inference, bootstrapping was used to calculate baseline values including standard errors and confidence intervals for work productivity and activities of daily living impairment. Bootstrapping is a data-based simulation method that relies on random repeated resampling of the same data to create new sample populations, thereby simulating variations in model parameters introduced by the process of random sampling and allowing the required statistic to be recalculated with increased stability. In this study, 1000 samples were created and used to calculate baseline values, including standard errors and confidence intervals for work productivity and activities of daily living.
Multivariate analyses were undertaken with the Bayesian Markov Chain Monte Carlo procedure in WinBUGs 26 using pooled data from the two identically designed phase III E2V/DNG HMB studies in North America and Europe/Australia to obtain overall estimates of the impact of treatment on work productivity and activities of daily living impairment at visit 7 (day 84) and visit 11 (end of treatment). 21 –23 Bayesian analysis for the multinational dataset from the two studies was applied to address the issue of generalizability of health-economic data collected within the multinational setting and to allow for the reduction of uncertainty in the country-level parameter estimates. 27,28 Results of productivity data for European and Australia setting are reported elsewhere; this article reports results for United States and Canada. 23 Both work productivity and activities of daily living impairment at day 84 and at the end of treatment served as dependent variables within the model. Relevant covariates included in the model were race, education level, standardized blood loss at baseline, the baseline global Psychological General Well-Being Index (PGWBI) score, treatment arm, and country-specific random effects. The robustness of the findings was tested using different distributional assumptions of dependent variables; both normal and gamma distribution was assumed for the work productivity and activities of daily living impairment variables. The choice of covariates and distributional assumptions was informed by Deviance Information Criterion. 29
At baseline, the monetary value of work productivity and activities of daily living impairment was calculated first by multiplying the mean monthly full-time salary for both countries separately (obtained from International Labour Organization [
Results
There were no significant differences in the baseline characteristics of the treatment and placebo groups. 21 The mean age was 36.9 years in the E2V/DNG group and 37.0 years in the placebo group. The majority of patients in each group were white (59.2% vs. 65.7%), and the most common bleeding symptom was HMB (75.8% vs. 85.7%). The E2V/DNG recipients had a significantly greater mean MBL reduction compared to baseline than placebo recipients (353 mL vs. 130 mL reduction; p<0.0001). Overall, 145 women completed the baseline mWPAIs, had no missing covariate data, and were included in the current analysis (n=99 in the E2V/DNG group and n=36 in the placebo group).
Work productivity and activities of daily living impairment at baseline and end of treatment are summarized across both countries in Table 1. In both countries, significant improvements were observed from baseline to end of treatment for work productivity and activities of daily living in women treated with E2V/DNG. Women in the placebo group also showed improvement, albeit to a much lower extent than that observed with E2V/DNG treatment. From Table 1, the improvement in work productivity from baseline to end of treatment with E2V/DNG treatment was 46% (i.e., a decrease from 4.12 on the Likert scale to 2.22) in the United States and 47% (i.e., a decrease from 3.97 on the Likert scale to 2.09) in Canada, while the improvement in activities of daily living was 53% (i.e., a decrease from 5.11 on the Likert scale to 2.40) in the United States and 56% (i.e., a decrease from 4.57 on the Likert scale to 2.00) in Canada. The improvements in work productivity and activities of daily living with E2V/DNG treatment relative to placebo ranged from 37.2% to 39.2% across both countries (Table 1). All differences between E2V/DNG and placebo for work productivity and activities of daily living at the end of treatment were statistically significant (p<0.05) as confirmed by multivariate frequentist analysis.
E2V/DNG (n=99) vs. placebo (n=36). Value of “0” indicates no impairment due to heavy menstrual bleeding and value of “10” indicates complete work productivity impairment or complete impairment of activities of daily living.
Likert-scale bootstrap values reported. Descriptive means for work productivity (presenteeism) were 4.10 (SD=2.80, United States) and 3.90 (SD=2.65, Canada). For activities of daily living, respective values were 5.10 (SD=2.88) and 4.50 (SD=2.61).
p<0.05 for E2V/DNG versus placebo using multivariate frequentist analysis.
EOT, end of treatment; E2V/DNG, estradiol valerate/dienogest.
The monetary gains (or savings) associated with improvements in work productivity and activities of daily living with E2V/DNG treatment are summarized in Table 2. Monthly gains due to E2V/DNG treatment (net of placebo improvement) and the associated improvement in work productivity were estimated to be US$80.2 and Can$70.8 (US$58.5) and those associated with improvement in activities of daily living were estimated to be US$84.9 and Can$73.5 (US$60.7).
Baseline and end of study bleeding days data at the country level were pooled between study arms. For the United States, the number of bleeding days were 7.1 and 5.7 at baseline and end of study, respectively, and for Canada these were 7.4 and 6.0, respectively. This approach led to a conservative estimate of the savings driven only by changes in mWPAI.
Discussion
Clinical data from this double-blind, randomized, placebo-controlled phase III trial showed that E2V/DNG was effective in treating HMB in the absence of underlying organic pathology, resulting in a large, rapid, and sustained reduction in MBL as well as improvements in iron metabolism and patient-reported outcomes (reported elsewhere 21 ). The decline in MBL with E2V/DNG was accompanied by significant improvements in hemoglobin, hematocrit, and serum ferritin concentrations. Furthermore, the proportion of women (excluding those subjects with missing data) defined as having a “complete response” to treatment was significantly higher with E2V/DNG than with placebo (35/80 [43.8%] vs. 2/48 [4.2%]; p<0.001). 21 The results reported in this article support the clinical findings and confirm that E2V/DNG also has a consistent, significant positive impact on work productivity and activities of daily living in U.S. and Canadian women with HMB. The improvement with E2V/DNG treatment exceeded 45% compared to baseline for both work productivity and activities of daily living outcomes across both countries.
Our results confirm that there is a substantial economic and social burden associated with HMB—baseline work productivity and activities of daily living impairment were close to or exceeded 40%. In addition, successful treatment of HMB with E2V/DNG increased work productivity and activities of daily living, an observation that is consistent with other studies demonstrating that successful treatment of HMB increases labor force participation. 31 –36 Overall, the direct cost of “abnormal uterine bleeding,” of which HMB is a subset, in the United States has been estimated to be $1 billion annually, with the estimate for indirect costs 12-fold higher. 12
U.S. data from a health plan perspective, showed treatment costs for dysfunctional uterine bleeding to be $513 a year with oral contraceptives, $3500 with first-generation ablation, $3000 with second-generation ablation, and $7500 with hysterectomy. 37 The annual value of lost income and lost household activities due to HMB/dysfunctional uterine bleeding has been estimated to be $2291 per affected woman in the United States. 4 In addition, there are also productivity losses associated with missed school or curtailment of educational pursuits as a result of HMB, but indirect cost data for absenteeism (or presenteeism) relating specifically to education (as opposed to employment) are lacking and thus constitute a gap in current HMB research.
We observed improvements in work productivity and activities of daily living with both E2V/DNG and placebo treatment, although the improvements were greater in the E2V/DNG group. It is possible that the close interaction with the study investigators may have had a positive impact on patients' perception and the management of the bleeding in both groups.
A major strength of our study is that the analysis drew upon randomized controlled trial data. Randomized trials are generally accepted as the gold standard in determining treatment effect because they not only provide the least biased evidence but also have high internal validity (the confidence with which the change in outcomes can be attributed to the treatment under investigation). 38 Randomization also minimizes systematic differences between placebo and treatment group that could influence outcomes. In addition, a controlled treatment environment minimizes systematic differences in the manner in which patients receive treatment. A shortcoming of clinical trials, however, is that they may not fully represent real-world populations (due to patient selection according to protocol inclusion and exclusion criteria) and practice (due to predefined treatment and observations schedule) and focus on the evaluation of clinical outcomes (thus not collecting information that is important from the economic perspective; e.g., costs). 39 Of note, the randomized sample represented approximately one fifth of the women screened; this can, however, be attributed to the stringent inclusion criteria, which rendered a large proportion of women with “perceived” HMB ineligible. 21
The main advantage of the WPAI instrument is its ability to be easily modified or adapted to measure lost productivity or impairment in daily activities associated with a specific disease. 40 Although we used a 12-week recall window with the mWPAI, the validity of using such a long recall window has not been established. The 12-week recall window was used in order to increase the likelihood of capturing the “average” effects of HMB on work productivity (presenteeism) and activities of daily living because the impact of HMB could vary across menstrual cycles depending on variations in bleeding duration and intensity. The last bleeding episode may not adequately reflect the average impact of HMB and account for the potential variability across cycles. However, this extended recall period, covering several bleeding episodes, may introduce the possibility of recall error as the variability between cycles may have been too great to obtain a meaningful average response. In addition, women may have difficulties rating the impact of their uterine bleeding, which causes problems only at certain times, over a duration longer than their actual bleeding of which many would be “well” days. 41 Other limitations of our analysis included our calculating mean group differences (rather than by individual), which makes no allowance for the fact some of the days of each period were likely to be on weekends. Further, each reduction in the Likert score was assumed to represent the same improvement irrespective of baseline starting level, and we assumed that all women worked full time and earned the national average salary. Finally, women randomized to placebo would have likely continued to experience heavy bleeding and may therefore have been relatively “unblind” to the fact that they were receiving placebo. This may have introduced a degree of bias that would clearly affect the WPAI responses.
Conclusions
In conclusion, E2V/DNG has a consistent, significant positive impact on work productivity and activities of daily living in U.S. and Canadian women with HMB. In addition, these improvements in work productivity and activities of daily living were associated with a reduction in HMB-related monetary burden compared to the placebo group. Observational studies in women with self-reported HMB (as opposed to clinical trials assessing HMB confirmed with objective measures) are needed to confirm our finding in the real-world setting.
Footnotes
Acknowledgments
This study was funded by Bayer Healthcare, Berlin, Germany, the manufacturer of the estradiol valerate/dienogest oral contraceptive. Editorial assistance with the preparation of this manuscript was provided by Richard Glover of in Science Communications, Springer Healthcare. Funding for this editorial assistance was provided by Bayer Healthcare.
Author Disclosure Statement
Radoslaw Wasiak, Donald E. Stull, and Steven Siak are employees of the United BioSource Corporation who were contracted to perform the analysis. David J. Vanness is contracted to United BioSource Corporation. Anna Filonenko, Kim U. Wittrup-Jensen, Amy Law, and Mark Jeddi are employees of Bayer Healthcare or its associated affiliated companies. Jeffrey Jensen has received payments for consulting and giving talks for Bayer HealthCare, a company that may have a commercial interest in the results of this research and technology. This potential conflict of interest has been reviewed and managed by Oregon Health & Science University. He is also a consultant for Merck and has received research funding from Abbott Pharmaceuticals, Bayer HealthCare, Warner Chilcott, the Population Council, and the National Institutes of Health.