
Abstract
Background:
We conducted a systematic review of the literature to determine the amount and duration of blood loss 24 hours to 12 weeks after delivery.
Methods:
We searched MEDLINE, CINAHL, and PubMed for studies between the years 1950 and 2011 that prospectively evaluated the amount and duration of blood loss from 24 hours to 12 weeks after delivery. Excluded were those that were only case studies, retrospective studies, studies not published in English, studies outside of the time frame, and studies that included only subjects from special populations.
Results:
From the 333 identified studies, 18 met inclusion criteria. There was variability in how the amount of blood loss was determined, ranging from subject self-assessment to objective measures, such as pad weight and spectrophotometric readings of hematin concentration. The reported duration of normal blood loss after delivery varied among the studies. Whereas the average duration of blood loss in these studies ranged from 24 to 36 days, in only 1 study was bleeding followed to cessation.
Conclusions:
An understanding of bleeding patterns after delivery is important for clinicians to recognize deviations from normal, identify women at risk for delayed postpartum hemorrhage, and limit unnecessary interventions, yet studies reveal significant variability in amount and duration of normal lochial blood loss and methods of assessment that are inconsistent. This review draws attention to the need for the establishment of valid, reliable, and feasible methods to quantify normal and abnormal postpartum blood loss.
Introduction
Delayed or secondary postpartum hemorrhage (PPH) has been defined as excessive, abnormal, or heavy vaginal bleeding or bleeding in sufficient amounts to require medical attention occurring between 24 hours and 12 weeks after delivery. 1 –4 Secondary PPH is associated with significant maternal morbidity, including pain, interference with activities of daily living, anemia, and fatigue, and it can also be fatal, particularly in underdeveloped countries. 3,5 –7
Some bleeding between 24 hours and 12 weeks after delivery is expected and is called lochia. Women experience this bleeding after they are no longer under the direct observation of a nurse, midwife, or physician, yet standard references are not available for either patients or providers to discriminate between acceptable bleeding and bleeding that requires clinical intervention. Despite continued calls for sound estimates of what constitutes excessive lochial loss, there is a severe lack of normative data on secondary lochial loss, and there are no standard methods for quantifying or treating delayed PPH. 2,3,6,8 –14 Although literature that states that delayed PPH affects anywhere from 0.8% to 2% of all deliveries, the actual incidence is not known because of a lack of standard assessment, quantification, and clinical criteria. 7,15,16 This is in contrast to primary PPH, which affects approximately 2%–5% of all deliveries. 17 –20
This article provides a systematic review of the published literature on assessing lochial loss between 24 hours and 12 weeks postpartum in order to better understand the median duration and amount of lochial loss and variables associated with increased loss and duration. Such data are vital for the establishment of reliable criteria to differentiate between normal and pathologic states, for the diagnosis of delayed PPH, and for the development of guidelines for prophylactic treatment to reduce patient risk of delayed PPH and related signs and symptoms.
Materials and Methods
MEDLINE, CINAHL, and PubMed were searched for literature published between 1950 and 2011 using combinations of the following terms: delayed postpartum hemorrhage, secondary postpartum hemorrhage, lochial and/or lochia, blood loss, and puerperium. The bibliographies from the identified references were also reviewed to identify additional relevant studies. We identified 419 records through database searching, and 2 additional records were identified through other sources for a total of 421 records. Duplicate records were identified and removed, leaving 333 records for consideration (Fig. 1).
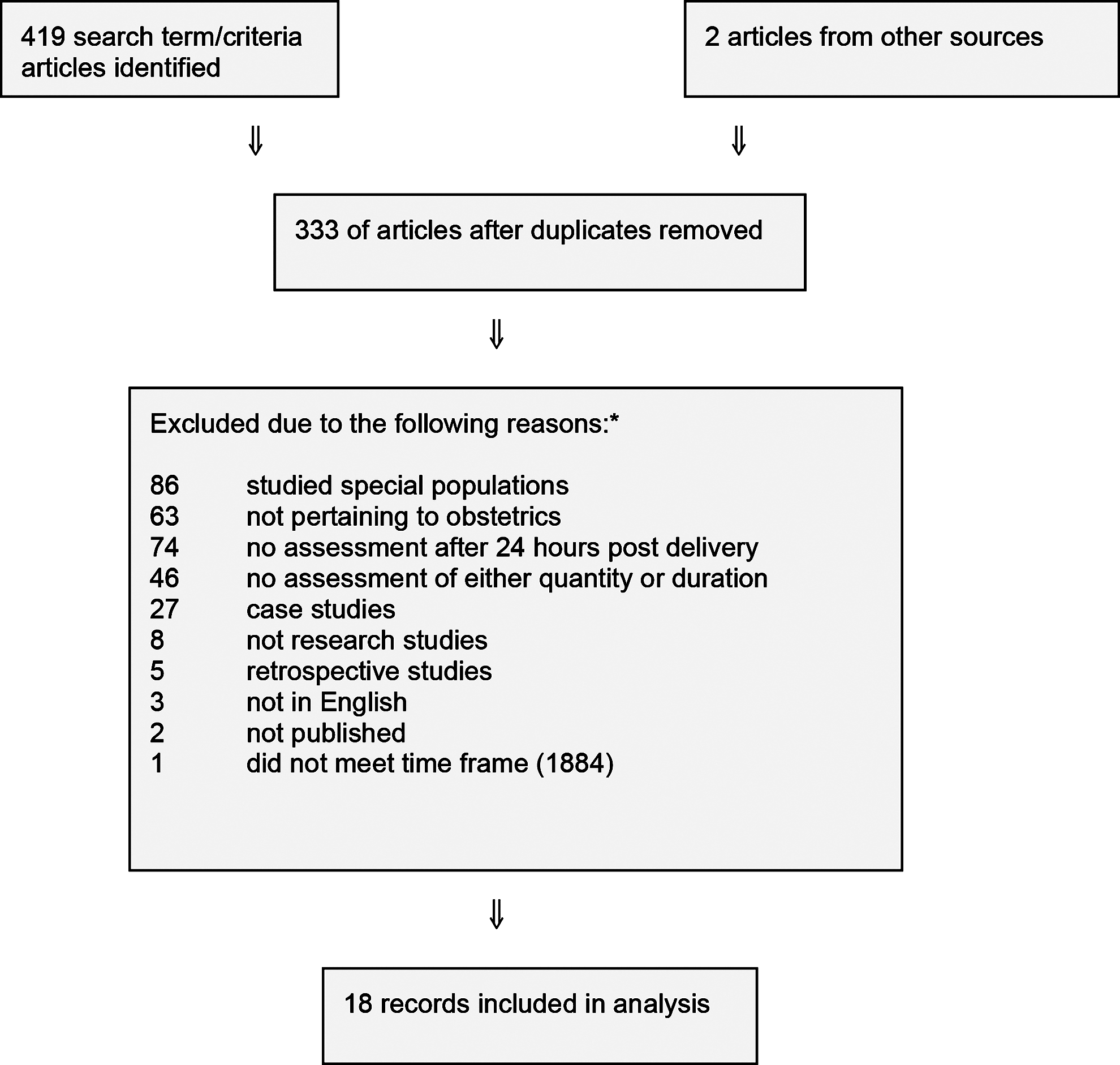
Study search and selection. *Some articles may have been excluded for multiple reasons. Only the initial reason for exclusion is cited.
Study selection
We considered all published studies that assessed the amount or duration or both of lochia loss between 24 hours and 12 weeks after delivery among normal patients. We excluded studies that investigated specific populations, such as patients with bleeding disorders or those with primary PPH. Studies were also excluded if they studied only special patient populations, did not pertain to obstetrics, did not assess lochial loss lasting longer than 24 hours postdelivery, did not specify a method to assess either amount or duration of loss, were case studies, were retrospective studies, were not published in English, or were published before 1950.
Studies assessing the amount of lochial loss 24 hours postnatal using self-report were included even if amounts were not quantifiable. Additionally, studies using self-report to assess duration of lochial loss were included even if averages were not determined. For the purpose of this article, lochia was defined as normal blood loss or discharge occurring between 24 hours and 12 weeks postpartum. Secondary/delayed hemorrhage was defined as clinically significant blood loss.
All decisions were discussed and reviewed by the co-authors. Eighteen articles were eligible for inclusion in this review and a summary of these articles is presented in Table S1 (Supplemental material available online at
Results
The 18 studies included in this review were published between 1950 and 2007. Seven studies were from the United States, 1,2,4,10,21,22,28 four from the United Kingdom, 8,9,14,23 two from India, 3,6 one each from Sweden, 24 Mexico, 25 Israel, 29 and Egypt, 26 and one was a multinational study. 27 Four studies 6,10,25,28 were nonrandomized experimental studies assessing the impact of variables on postpartum lochial loss, which included the uterotonic agent oxytocin 1,25,28 or kutapressin (a nonsteroidal anti-inflammatory drug [NSAID]) 10 or an intrauterine device (IUD). 6 Although 2 studies included data on lochia immediately after delivery up to 24 hours postpartum, the information is not included in this review. 24,25 Results not specifically related to the amount or duration of lochial loss are not included in this review even if they were part of the original study.
The sample size of subjects ranged from 98 to 3955. 27 Although not all articles included patient ages, the youngest known age was <15, 3 and the oldest documented age was 42, 8 although other studies reported having patients in the sample who were >age 40. 4,9,10,14
Definitions related to clinically significant bleeding varied. Bang et al. 3 defined delayed PPH as the use of >5 pads a day 5 days after delivery or increased vaginal bleeding after bleeding had decreased or stopped or any increased use of pads by at least 2 after bleeding was less or none and found that 15% of the women reported delayed PPH in their study. Fronczak et al. 2 defined delayed PPH as passing fresh or clotted blood more than 3 days postpartum; 30% of participants in this study reported secondary PPH. Bleeding complications were defined by Sokol et al. 22 as any postpartum bleeding requiring medical intervention. No participants in their study reported complications.
Table 1 presents the 8 studies that reported the duration of normal lochial loss after delivery using tests of significance. 6,9,14,21 –23,27,29 The mean duration of blood loss reported in these studies ranged from 24 days 9 to 36 days. 29 The shortest recorded duration was 2 days, 27 and the longest was 90 days 6 (Table 1).
Only includes control groups.
Average lochial loss varied greatly depending on time frame and methods of assessment. There were 6 studies quantifying the amount of lochial loss. 1,4,8,24,25,28 Two studies weighed perineal pads as a means of assessing loss, 1,4 1 study used spectrophotometric readings, 24 and 3 used alkaline hematin methods for assessment. 8,25,28 Although all studies assessed lochial loss 24 hours postdelivery and longer, as required by our study inclusion criteria, there was great diversity in the time of initial assessment, with 2 studies including lochial loss during delivery. 4,25 Only 1 study measured lochial loss until cessation. 29
Five studies used only self-reported measures to assess quantity, providing a nonvalidated scale for light to heavy bleeding and clinically significant bleeding without comparison to an objective test. 1,2,26,28,29 None of the studies used identical definitions or parameters for operationalizing the terms light, moderate, heavy, excessive, or delayed PPH. One study used a modified Pictorial Assessment Blood Chart (PBAC). 14
Subjects in 1 study reported a moderate amount of lochial loss for an average of 4.6 days (±5.1) after delivery, a light amount for 15.2 days (±7.2), and scant amount for 36 days (±7.5). 29 In another study, 49% of subjects reported light bleeding at day 14, 9 % reported heavy bleeding at day 14, and 38% reported light bleeding at day 42 compared to 2% reporting heavy bleeding. 26 A third study using self-report compared women with and without an IUD. 6 Within the study group, 40% of the women with an IUD reported excessive lochia loss compared to 11% of the women without an IUD. A study examining postdelivery complications reports that primiparas were significantly more likely to report delayed PPH. 2
Significant relationships were found between variables examined and both duration and amount of blood loss. One study found a significant relationship between duration of blood loss and parity, with increasing parity significantly related to decreasing median duration of bleeding (p<0.05). 23 Five studies examined the relationship between duration of bleeding and birth weight. 8,14,21,23,27 Of these 5 studies, 2 found that increasing birth weight was significantly related to increasing median duration of bleeding (p<0.05) and birth weight was related to increased duration at two of the seven centers in the study by the World Health Organization (WHO). 23,27
Patient location, which may have been affected by differential reporting from various sites, was significantly associated with duration in the WHO study, with the two samples of white women from developed countries having the longest durations (Melbourne/Sydney, Australia, and Uppsala, Sweden)(p<0.001). 27 Significant relationships were also found between duration of lochia and the use of a nonhormonal IUD inserted postpartum. 6 IUD use was associated with longer duration of lochia.
No study found a statistically significant relationship between duration of lochia and history of prior cesarean birth, duration of normal menses, gestational age at delivery, infant sex, mother's racial or ethnic background, mode of delivery, maternal weight, administration of oxytocic drugs, oral contraception postpartum, resumption of sexual activity, or smoking.
Of the 2 studies that examined the impact of oxytocic agents given immediately after delivery on the amount of lochia loss, one study reported no statistically significant differences between those women receiving oxytocin and those not receiving oxytocin, 25 whereas the other study reported that those receiving oxytocin lost significantly more blood than those not receiving it (p<0.05). 28
Results from the Bernstine and Bernstine study 4 suggested that the greatest amount of lochial loss was found among older mothers (40–45 years) and the least among the youngest mothers (16–20 years), although statistical tests of significance were not documented. The same study noted greater loss among nursing mothers, but the differences were not statistically significant. Results from 4 other studies comparing nursing and nonnursing mothers did not note any significant differences. 1,14,28,29 One study found a correlation between length of labor and mode of delivery with amount of lochia, 14 and another study found a correlation between having one or more risk factors and delayed PPH. 26 Risk factors included premature rupture of membranes (PROM), induced labor, oversized uterus, pregnancy-induced hypertension, antepartum hemorrhage, prolonged labor, operative delivery, obstructed labor, and precipititous labor.
Two studies assessed the color pattern of lochia over time using a graduated color slide including rubra (red-brown); serosa (brown-pink-brown), and alba (yellow-white). 23,29 In Oppenheimer et al., 23 the median duration of lochia rubra was 4 days (range 2–6), lochia serosa 22 days (16–35), and total duration of lochia was 33 days (23–48). Thirty-six percent of participants did not experience lochia alba. In the Sherman et al. study, 29 the median duration of lochia was 37 days (range 17–51). Three types of color patterns were identified: type 1 was a prolonged rubra phase, type 2 had two rubra phases, and type 3 had nearly equal rubra and alba phases. The rubra phase lasted 12.1±6.7 days in type 1, 24.8±5.0 in type 2, and 5.5±2.5 days for the first rubra in type 3. Although there were no statistically significant differences in overall duration of lochia, significantly more lactating women were in the type 1 group than type 2 (p<0.05), and women with higher parity were significantly more likely to have type 2 compared to type 1 (p<0.05). 29 The amount of lochial loss was not included in either of these studies.
Discussion
From the 18 studies included, the average duration of lochia was 24–36 days, although studies included in this review suggest lochial flow beyond the 6 weeks time period is not unusual. 21,23,27,29,30 The definition of duration of lochia was not consistent among the studies, as the majority of studies terminated the period of observation before the actual cessation of bleeding. Two studies followed the bleeding to cessation. 14,29 Because of the truncated period of observation, there is an inherent bias toward shorter duration, making the durations cited in these studies unreliable. Therefore, one cannot rely on 24–36 days as the average length until cessation of bleeding.
It is impossible to discern the average quantity of blood loss from the studies included in this review. In general, lochia diminished over time, but there is no universal way of measuring lochia. Very little can be said about the quantity of lochial blood loss, as no standardized and validated measures or scales exist. Whereas some of the studies used the weight of perineal pads or other objective methods to quantify the amount of blood loss, the majority of studies relied on the subjects' subjective description. A woman's own description of lochia loss ≥24 hours after delivery is often the sole determinant for seeking medical intervention, yet the use of self-report without standardized quantification has limited clinical value. Studies on menstrual loss and primary postpartum lochial loss (between delivery and 24 hours postnatally) suggest visual estimation of loss is often underestimated. 11,12,31
Some studies attempted to explore variables associated with lochial duration and amount. Results were conflicting, and no associations were found between many plausible variables and lochial loss. More than one study, however, found an association between birth weight and lochial loss and IUD use and lochial loss. Chi et al. 14 found that women with bleeding disorders, as well as women who had long labor and underwent instrumental delivery, have increased duration and amount of lochia. In general, when the duration and amount of lochia in normal women are not clearly established, the impact of various factors on the duration and amount of lochia is difficult to assess.
The lack of standard definition as to what constitutes clinically acceptable lochial loss during this period is evident from this review. For example, light or small bleeding was defined as < a 4-inch stain on a perineal pad, 29 similar to menstrual bleeding, 26 or < a 2-inch stain on a sanitary pad. 9 Heavy bleeding was operationalized as requiring more than four pads per day for ≥ 10 days 26 or a saturated perineal pad within one hour. 29
There was also variability among studies defining delayed PPH. Marchant et al. defined delayed PPH as “any abnormal or excessive bleeding from the birth canal occurring between 24 hours and 12 weeks postnatally,” 9 while Bang et al. operationalized delayed PPH as “after five days post delivery, the use of more than five pads a day” or “increased bleeding after bleeding had decreased or stopped” or “any increase in use of pads by two or more after it was less or none.” 3 The definition used by Fronczak et al. 2 was passing fresh or clotted blood more than 3 days postpartum.
These findings are consistent with a recent review of common obstetric terms. 32 In their review of 17 sources (including student textbooks, medical dictionaries, and midwifery textbooks) for common obstetric terms, the authors noted the lack of consistency in defining delayed PPH among the 12 sources that included a definition of delayed PPH and stated the need to quantify delayed or secondary PPH. 32 It is, therefore, difficult to draw any conclusion from these studies because methods of quantification were so disparate, with no validated forms of measures and no validated scales. Such variability among definitions and methodologies make determination of clinically significant lochial loss difficult to assess for patients, clinicians, and researchers.
A lack of guidelines contributes to the inconsistency in defining, assessing, and treating delayed PPH. 7,11,12,14,15 Hospital admission data suggest the incidence of delayed PPH is 0.8%–2.0%, 7,15,28 but the variability of definitions used and the lack of consistent methods to assess lochial loss cast doubt on these figures. It also puts into question incidence data on women with bleeding disorders in relation to delayed PPH. Results from this review confirm findings by others that practitioners lack adequate knowledge about normal blood loss during the postpartum period and that, consequently, treatment of abnormal postpartum bleeding may be suboptimal. 33,34
There are limitations to this systematic review. The studies included investigated different study populations and used different outcome variables and assessment techniques. There was also a lack of standardized assessment (e.g., standardized pads, valid surveys) and lack of strong methodology. Changes in diagnosis, assessment techniques, and tools are partially due to the variable time periods in which the studies were conducted; methods did strengthen in studies conducted since 1999. 2,3,14,22,27 Most of the limitations are inherent in the studies themselves and, although these limitations are noted, the strength of this review is that we have systematically reviewed research studies on delayed PPH and are able to bring attention to the lack of clinically relevant standards for assessing abnormal postpartum bleeding and delayed PPH. This review also draws attention to the need for the establishment of valid, reliable, and feasible methods to quantify abnormal postpartum blood loss for patients, medical providers, and researchers.
We recommend further studies using methods similar to that used by Chi et al. 14 to compare the amount and duration of lochia in women with and without inherited bleeding disorders. Patients in this study used standardized predetermined sanitary pads and completed a booklet consisting of weekly modified PBACs to assess the amount of lochia loss. These methods are consistent with those suggested to improve measuring blood loss by Jacobson et al. 11 and Luegenbiehl et al. 12 Randomized studies using standard sanitary pads in which saturation levels have been predetermined and standard amounts of loss per PBAC categories have been validated would allow for a more objective measure of blood loss.
Although the need for sound estimates of what constitutes excessive lochia loss has long been cited, without valid clinical guidelines, determining normal bleeding vs. bleeding requiring medical attention cannot be differentiated in a reliable manner. This lack of information restricts clinicians' ability to determine if rehospitalization is required. Without adequate knowledge of lochial loss, clinicians are also limited in identifying those women who may be at risk for delayed PPH. Risks associated with this lack of clinical criteria include the potential for serious postpartum morbidity; lack of readmission for patients in need; unnecessary hospitalization for others, thereby increasing burden on families and costs; unnecessary stress to patients and families based on this ambiguity; and failure to provide adequate prophylactic treatment for those known to be at risk for hemorrhage. 14,31
Footnotes
Disclosure Statement
No competing financial interest exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.