
Abstract
Anemia is a global health issue with disproportionately high prevalence in women. In addition to being an independent risk factor for decreased quality of life and increased morbidity and mortality, anemia in women has been linked to unfavorable outcomes of pregnancy and other issues for children born to anemic women. Iron deficiency is the leading cause of anemia in many populations. Guidelines recommend proactive screening for anemia, particularly in the preoperative setting. Once anemia is diagnosed, treatment should be based on etiology (most commonly, iron deficiency followed, in order of prevalence, by inflammation or chronic disease). Iron supplementation (oral and intravenous) offers safe and effective treatment for anemia associated with iron deficiency. Anemia of chronic disease may be more challenging to treat, and attention must be given to the underlying disease, along with use of hematinic agents. Given its enormous impact on the health and well-being of women and the availability of simple and effective treatment options, anemia should never be left unmanaged.
Introduction
Anemia is an extremely common condition with a disproportionate prevalence in women. Globally, it is estimated that 1 of every 4 human beings is anemic. The prevalence increases to 30% in nonpregnant women and 42% in pregnant women across the world. 1 In the United States, according to the United States Centers for Disease Control and Prevention (CDC) data from 1999–2002, anemia affects almost 7% of reproductive-age women and up to 20% of women >85 years. 2 There is great racial disparity, with 3.3% of white, 8.7% of Hispanic, and 24.4 % of black women <50 years diagnosed as anemic. 2 Despite advances in healthcare, anemia remains a “global health problem” 1 as well as a public health concern in the United States, particularly affecting women.
Significance of Anemia
Regardless of gender or age, anemia has been identified in numerous studies as an independent risk factor for morbidity and mortality. 3 Additionally, anemia in women may be associated with decreased cognitive function, concentration, and attention (in women as well as their children) 4 –8 ; lower birth weight newborns and possible increased risk of preterm delivery; and disturbed postpartum maternal-infant interaction, 9,10 potentially leading to developmental deficits in childhood. 9 –11 Anemia-related quality of life deficits include loss of vitality, fatigue, depression, diminished physical function, and impaired work performance. 12 –14 Restless leg syndrome 15 and pica 16 are also linked to anemia, specifically iron deficiency anemia (IDA). IDA can lead to decreased exercise and cold tolerance. 17,18 Although women typically do not volunteer many of these symptoms, 12 standardized quality of life assessment instruments reveal scores for anemic women comparable to those of patients with serious chronic diseases of major organ systems. 12,14,19 –21 These scores are directly proportional to the severity of anemia, 12 although generally out of proportion to symptoms (Fig. 1). 22 –26
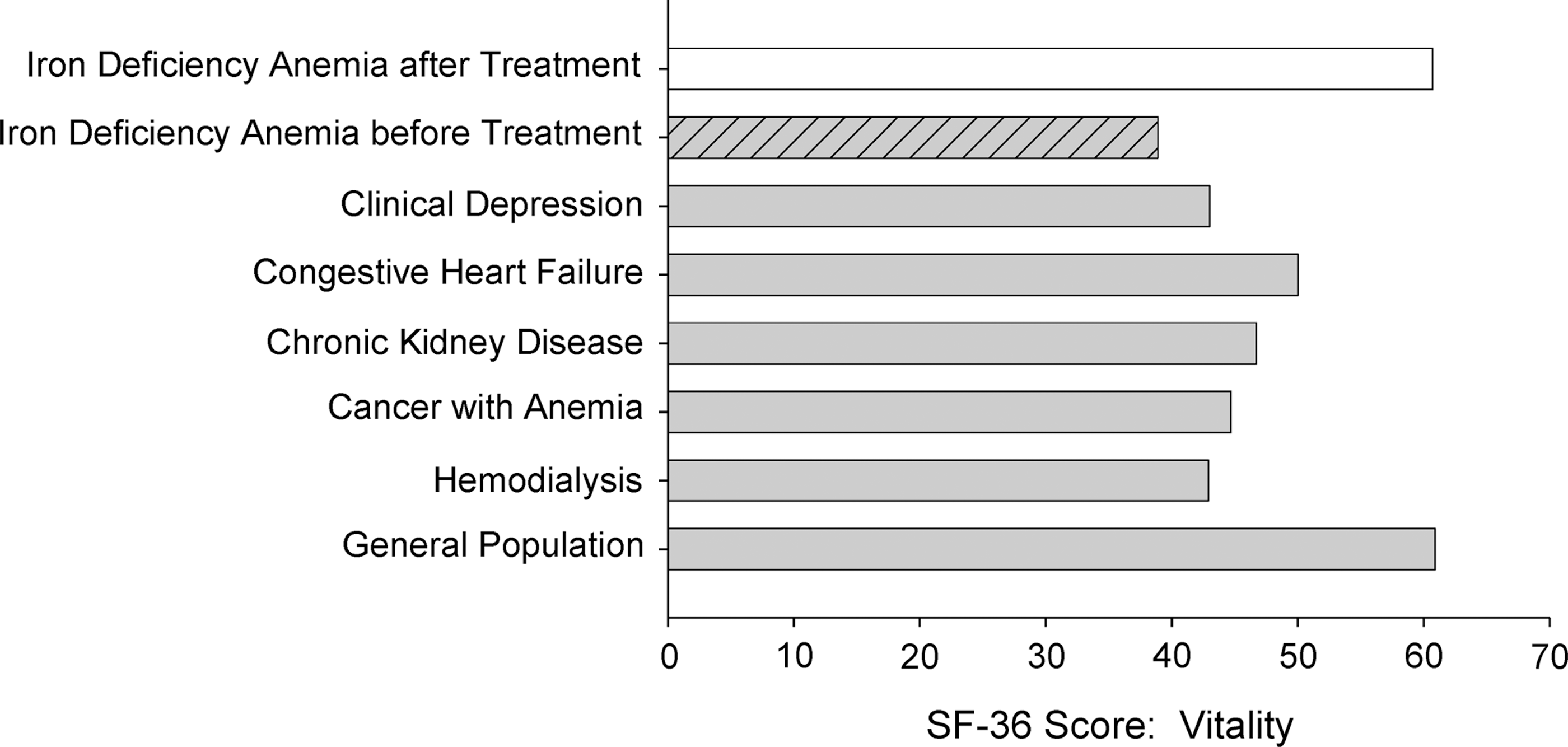
Short form-36 (SF-36) vitality scores in women with iron deficiency anemia (IDA) compared with scores seen in patients with other chronic illnesses. Data sources are as follows: IDA before and after anemia, 23 ; clinical depression and congestive heart failure (CHF) 24 ; chronic kidney disease, hemodialysis, and general population 25 ; cancer with anemia. 26
Despite its wide prevalence and significant consequences, anemia receives little attention from either the medical community or the public at large. It is the purpose of this report to summarize the current knowledge about anemia and its diagnosis and treatment at key stages of a woman's life, focusing on IDA, the most common type of anemia.
Childhood and Adolescence
Contrary to common expectations, 3.6% of U.S. children between 12 and 59 months old are anemic, with one third of them being iron deficient. 2 Iron deficiency is the most common cause of anemia in adolescents, affecting 10 times as many girls as boys. 27 The risk is greatest at the time of the somatic growth spurt, which in girls commonly coincides with the onset of menstruation. 28 Many adolescent girls experience anovulatory bleeding, often heavy and prolonged, compounding the problem through increased blood loss. Somatic growth, menstrual blood loss, reticence to discuss excessive menstrual blood flow, and body image and dietary issues all impact the ability to diagnose and prevent adolescent anemia.
Although data are conflicting, many studies show the possible negative impacts of anemia on young women. Iron-deficient adolescent girls, with and without anemia, score lower on standardized tests in mathematics than those with normal iron levels. 23 Iron supplementation in iron-deficient adolescent girls (even without anemia) improves cognition and school performance. 29 –31 A meta-analysis of randomized controlled trials on children and women showed iron supplementation improved the intelligence quotient (IQ) by 2.5 points in anemic patients. 32 Nelson et al. 33 reported in a British study that anemic 12–14-year-old girls had significantly elevated heart rates after a 2-minute step test compared with nonanemic girls. Notwithstanding all the potential confounding variables, it is postulated that such decreased physical performance capacity may adversely influence attentiveness and learning ability as well as the ability to maintain the levels of physical activity necessary for healthy physical development. 34
Pregnancy
Pregnancy is a time of increased demand on maternal resources, including the bone marrow. During pregnancy, plasma volume increases by 40%–50% until about the 30th week of pregnancy. During the same period, red blood cell (RBC) mass also rises, although only by 20%–30%. The net result of these changes is hemodilution, which causes the “physiologic anemia of pregnancy.” 35 Compounding the increased demands on the pregnant woman, the developing fetus requires iron to synthesize its own RBCs. There is a preferential transfer of maternal iron to the fetus, leading to further depletion of maternal iron stores. The combination of increased maternal and fetal erythropoiesis causes increased iron requirements. When the blood loss occurring during delivery is considered in addition to the increased pressures on maternal RBC production (often in context of low iron stores), it is no surprise that IDA develops in as many as 37% of pregnancies in the United States and as many as 80% of the pregnancies in the developing world. 27,36,37
Postpartum Period
The hemoglobin (Hb) level measured 4–6 weeks after delivery reflects the combined contributions of Hb and iron status during pregnancy, blood loss at delivery, and reversal of physiologic hemodilution. Median blood loss at vaginal delivery is about 250 mL, but >5% of deliveries are associated with >1,000 mL blood loss 24 ; blood loss >500 mL precipitates anemia in previously nonanemic women. 25 The expected drop in Hb of 0.1–0.6 g/dL at 3 days after normal delivery 26 is quickly reversed as postpartum diuresis eliminates the excess plasma volume, leading to rapid hemoconcentration and a brisk rise in Hb level from the third postpartum day forward. 38 By the fourth postpartum week, Hb levels generally return to normal. 39
Nevertheless, postpartum anemia remains strikingly common, especially in low-income, Hispanic and African American women. 40 Of the nearly 60,000 participants in the Special Supplemental Nutrition Program for Women, Infants and Children, 27% overall, 40% of the Hispanic, and 48% of the non-Hispanic African Americans were found to be anemic between 4 and 26 weeks postpartum. Even with normal Hb levels during pregnancy, 20% of low-income women were anemic at their first postpartum visit. Additional risk factors included multiparty, obesity, anemia during pregnancy, age <20 years, unmarried status, and not exclusively breastfeeding. 40,41 This increased prevalence of anemia persists up to 12 months postpartum. 42
The existence of maternal anemia in the postpartum period may have long-term consequences for the newborns as well. Although the conclusions are weakened by confounding variables, such as socioeconomic status, some studies suggest that uncorrected IDA may negatively impact maternal cognition, mood, and behavior, 11 which may lead to disturbed maternal-infant interactions and in turn to lasting deleterious effects on early childhood development. 9,11,35 Mothers with IDA may be less responsive to and more controlling of their infants than nonanemic mothers. 9 Infants of these mothers may be developmentally delayed at 10 weeks of age. Evidence that these developmental deficits persist long after maternal anemia correction suggests the possibility that postpartum maternal anemia may lead to long-standing impairment of early childhood development. 9
Perimenopausal Period
It is estimated that about 20% of women suffer excessive menstrual blood loss, accounting for 40 of every 1,000 medical consultations annually. 43 Blood loss due to menstruation is a common cause of IDA in perimenopausal women. Many women in their 40s note shortened or very irregular menstrual cycles and heavier, prolonged menses. Most often, these bleeding abnormalities are associated with uterine fibroids or anovulation. Using the definition of menorrhagia as menses lasting >7 days or blood loss of at least 80 mL (compared with average loss of 35 mL), two thirds of women with menorrhagia have IDA. 44
Many women with perimenopausal menorrhagia or anovulatory menometrorrhagia ultimately require either medical or surgical treatment. Despite the availability of many highly effective medical and minimally invasive surgical therapies, hysterectomy remains a common procedure to treat the problem. As many as 40% of the >500,000 hysterectomies performed annually in the United States 45 are done for bleeding. 44 Approximately 8%–9% of hysterectomies are associated with significant morbidity. 46 Ironically, bleeding and consequent anemia, the conditions that led to hysterectomy in the first place, increase that risk as well as the chance of requiring RBC transfusion, with its own potentially negative consequences. 3
Postmenopause and Later Life
Once women complete their reproductive years and enter menopause, anemia becomes far less prevalent. A systematic review of European and U.S. geriatric literature found the prevalence of anemia in elderly women ranged from 3% to 41%. 47 According to data from the Third National Health and Nutrition Examination Survey (NHANES III), 48 12.2% of women between the ages of 17 and 49 are anemic by World Health Organization (WHO) criteria (Hb<12 g/dL), whereas in the age range 50–64, only 6.8% have this diagnosis. As women continue to age, however the frequency of anemia gradually increases to the point that after age 85, about 20% have the diagnosis. Non-Hispanic black women are three times as likely to be anemic as their white counterparts. Among women residing in nursing homes, approximately 50% are anemic. 49
One third of anemia in older adults is nutritional (due to iron, folate, or vitamin B12 deficiency), and it is often associated with gastrointestinal bleeding; one third is anemia of chronic disease (inflammation or kidney disease); and the remaining one third is unexplained. 48,49
Anemia in the elderly is associated with frailty, increased mortality, poor cognition, and decreased physical performance. 50 –52 It is also a potent comorbidity in heart disease 53,54 and chronic kidney disease. 54 When anemia is present in patients with chronic kidney disease, the relative 2-year mortality risk increases from 2.05 to 3.07. When added to congestive heart failure, mortality risk increases from 2.86 to 3.78, and when anemia complicates combined heart failure and kidney disease, the risk jumps from 4.86 to 6.07 (Fig. 2). 54
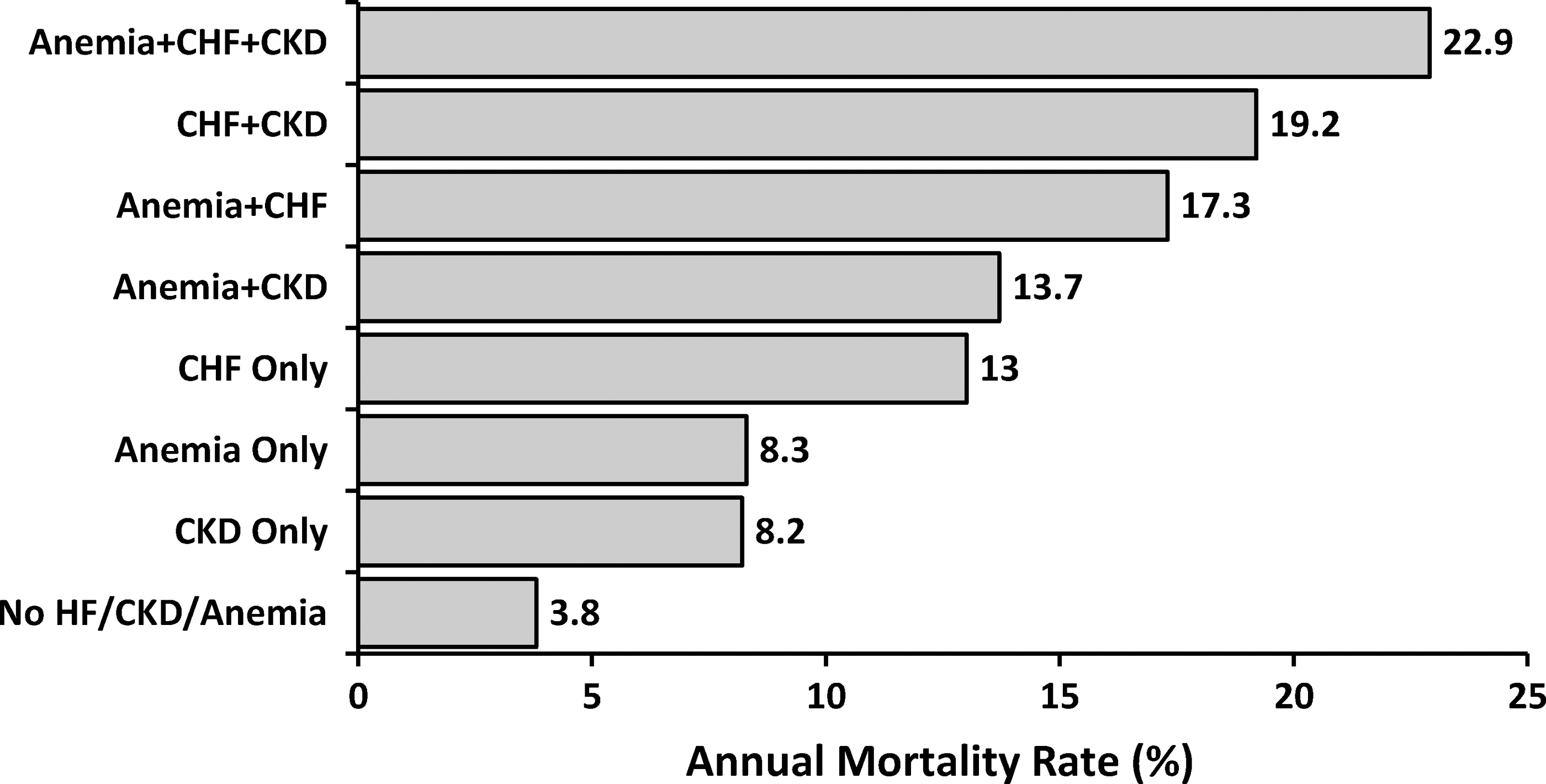
Anemia, a potent multiplier of mortality. Annual mortality rates in patients with various combinations of anemia, CHF, and chronic kidney disease (CKD). Data are derived from 1.1 million patients ≥67 years, representing a 5% random sample of the U.S. residents enrolled in Medicare during the 1996–1997 period. 54
Iron Requirements
Production of RBCs requires incorporation of iron into the Hb molecule. Iron requirements are met through a combination of orally ingested iron, stored iron, and iron recycled from the breakdown of senescent RBCs. If iron needs exceed supply, iron deficiency and IDA eventually occur. The average woman has approximately 40 mg/kg of total body stores, 55 which are maintained by a daily absorption of 1–2 mg of iron through the enterocytes in the duodenum. The body loses 1–2 mg of iron per day through the stool from sloughing of duodenal enterocytes, which absorb and store iron, and desquamation of skin cells. In women of reproductive age, the additional loss of an average of 1 mg iron per day (highly variable and for some women as high as 2 mg per day) through menstruation tips the balance toward the development of IDA. 56,57 Adolescents require additional iron to support the somatic growth spurt that immediately precedes and overlaps menarche. Pregnancy adds the demands of fetal iron needs and increased maternal erythropoiesis. Based on these factors, recommended dietary allowance (RDA) for iron in women varies from 7 to 10 mg/day from aged 1–13 years, 15 mg/day from 14 to 18 years and 18 mg/day in those 19–50 years old, returning to 8 mg/day after age 51. Regardless of age, the RDA for iron in pregnant women is 27 mg/day. 56
Iron Absorption and Metabolism
Humans have no mechanism to actively excrete iron. Therefore, iron homeostasis is dependent on a complex system of feedback regulation among body needs, passive losses, recycling, and iron absorption. 55 Dietary iron exists in the ferric and ferrous forms. Ferric iron must be reduced to the ferrous form by Fe-reductase in the gut before it can be absorbed by the cell. Absorption across the enterocyte cell membrane requires the action of divalent metal transporter 1 (DMT 1). Expression of Fe-reductase and DMT 1 is increased in states of iron deficiency and decreased in iron overload, thereby modulating iron absorption. As noted, the total amount of ferrous iron absorbed from the duodenum is 1–2 mg/day. The ferrous iron is then oxidized back to the ferric state by Fe-oxidase hephaestin in the cell membrane and is transported across the antiluminal section of the cell membrane via the transmembrane protein ferroportin, present in all cells that store iron. The peptide hormone hepcidin inhibits the ferroportin-mediated release of ferric iron from enterocytes and other cells containing ferritin. The expression of hepcidin is decreased in states of iron-deficient erythropoiesis and increased in iron overload, thereby modulating iron release by the enterocyte. Once released into plasma, ferric iron complexes with transferrin. The transferrin-iron complex travels via the portal circulation to the liver and then the spleen, where it binds to transferrin receptors (TFR) on hepatocytes and macrophages. Iron is then stored in these cells as ferritin until released by ferroportin, primarily for heme synthesis in erythroblasts. Under conditions of iron-deficient erythropoiesis, hepcidin activity decreases, thereby increasing iron availability. 58,59
Diagnosis of Iron Deficiency Anemia
As a practical matter, anemia in reproductive-age women is generally easy to diagnose. A complete blood count revealing an Hb level <12 g/dL in a nonpregnant woman, <11 g/dL in the first or third trimester of pregnancy, or <10.5 g/dL in the second trimester is defined by the CDC as anemia. 27 A simple algorithm proposed by the Network for Advancement of Transfusion Alternatives (NATA) for detection and evaluation of anemia in the preoperative setting uses iron studies, renal function evaluation, vitamin B12/folic acid measurements, and additional workups that can also be considered in other settings. 60 Generally, if the serum ferritin level is low (<15 μg/L in adults), the diagnosis of IDA can almost certainly be made. 61 Women with this diagnosis should be evaluated for a source of blood loss (most commonly menstrual) and treated with iron supplementation. In postmenopausal women or in reproductive-age women whose menstrual bleeding does not seem to explain the anemia, a gastroenterologic evaluation should be performed. 62
When these laboratory values are not definitive and in women suffering from chronic medical or inflammatory conditions or in women who do not respond to appropriate iron therapy, a more complete evaluation may be necessary to diagnose the cause of anemia, which may include factors other than iron deficiency. Additional tests, such as serum vitamin B12, folate, iron, transferrin, transferrin saturation, soluble TFR, and cytokine levels can help determine the diagnosis (Table 1). Differentiation of IDA from anemia of chronic disease (ACD, also known as anemia of inflammation), the second most common form of anemia, can be difficult. 63 In IDA, there is inadequate iron for erythropoiesis, resulting in microcytic anemia. In contrast, ACD is generally a normocytic anemia, in which there is decreased iron absorption from the gut as well as sequestration of iron by the reticuloendothelial system, leaving it unavailable for erythropoiesis. The primary agent believed responsible for these changes is hepcidin, whose activity increases dramatically in inflammatory conditions, renal disease, and cancer. In addition, in ACD, there is commonly a blunting of the expected increase of erythropoietin production and its effectiveness in stimulating erythroid progenitor cells, further contributing to decreased RBC production.
ACD, anemia of chronic disease; IDA, iron deficiency anemia.
To further confound the diagnostic dilemma, a number of patients with ACD are also iron deficient. Compared with those with pure ACD, those with both ACD and IDA more frequently have microcytes, and their anemia tends to be more severe. In both IDA and ACD, iron levels and transferrin saturation are low, but unlike IDA patients, women with ACD generally have normal to high ferritin and cytokine levels, low to normal transferrin levels, and normal soluble TFR levels. 63 Identification of those with combined IDA and ACD may be assisted by calculating the ratio of soluble TFR to the log of the ferritin level. A ratio of <1 suggests ACD, whereas a ratio >2 suggests IDA coexisting with ACD (Table 1), 64,65 although other cutoff values have been suggested, and more data are needed. 66,67
Treatment
The rationale for treating even mild IDA is to improve the well-being and quality of life of its sufferers and to reduce the associated morbidities and mortality. The effect of anemia treatment has been studied best in chronic renal failure patients. The reported 2-fold increased risk of death of those with a hematocrit <30% is eliminated when levels are corrected to ≥30%. 63 Anemic dialysis patients also demonstrate improved quality of life measurements after anemia is corrected. These improvements do not require complete correction to normal Hb levels but are observed at Hb levels around 10 g/dL. In fact, correction to Hb levels >12 g/dL is not associated with significant additional benefit and probably does not justify the risks of further treatment. 68
According to the NATA anemia algorithm, treatment should be based on the results of the diagnostic workup 60 and the clinical situation. Once the cause and type of anemia are established, treatment is usually straightforward and highly successful. This is particularly true in IDA. Oral iron is generally the first-line treatment. Although natural dietary sources of heme-iron (such as red meats) are better absorbed and tolerated, most women with IDA are treated with oral iron supplements. Oral iron taken on an empty stomach with additional ascorbic acid is highly effective in compliant nonpregnant 62 and pregnant women. 69 However, at least 20% 70 and perhaps as many as 40% of women cannot tolerate the associated gastrointestinal side effects. One alternative for patients who cannot tolerate daily oral iron is intermittent dosing. Although less effective than daily supplementation, it is preferable to no treatment and can improve Hb levels in women or children who cannot tolerate daily iron. 71,72 There are many different iron salts available, with the ferrous compounds generally better absorbed than the ferric salts. Women who cannot tolerate oral iron and those who do not have an adequate response to it should be treated with intravenous (IV) iron.
In the United States, there are currently five commercially available IV iron preparations, and a sixth, iron carboxymaltose (Injectafer) is in development. These are low molecular weight iron dextran (INFeD), sodium ferric gluconate complex in sucrose (Ferrlecit), iron saccharate (Venofer), high molecular weight iron dextran (Dexferrum), and ferumoxytol (Feraheme). All are iron carbohydrate complexes. The total dose required is determined using a formula incorporating the patient's body weight, current Hb level, and target Hb level. 73 This dose is then administered IV in fractions or as a total dose infusion (TDI) depending on the agent prescribed and the clinical need. Dosing frequency for each agent is largely dependent on rate of clearance from the plasma, which in turn is inversely related to the molecular weight of the specific iron-carbohydrate complex. Hence, iron sucrose and ferric gluconate clear faster than the dextran compounds and ferumoxytol. The dextran preparations release iron more slowly, however, based on their higher molecular weight and stronger iron complexes, thereby leading to a reduced risk of labile iron toxicity. As a result, the iron dextran preparations can be given as large single doses, up to 1–3 g in a single infusion, whereas iron sucrose should be limited to 400 mg and ferric gluconate to 250 mg per infusion. 73
Wide clinical use of IV iron therapy has been limited over the years by concern over severe allergic and anaphylactoid reactions. The nondextran formulations, ferric gluconate and iron sucrose, are considered to produce markedly fewer serious complications than the dextran preparations. 74 A 2006 retrospective analysis of Food and Drug Administration (FDA)-reported adverse events by Chertow et al. 75 indicated the rates of life-threatening adverse events were as follows: high molecular weight iron dextran (11.3 per million), low molecular weight iron dextran (3.3 per million), ferric gluconate (0.9 per million), and iron sucrose (0.6 per million).
In general, multidose regimens using the iron salts (gluconate and saccharate) are very safe and effective. Ferric gluconate and iron saccharate are usually given in doses of 125 mg and 200 mg IV daily, respectively, over a few minutes, each with minimal side effects and excellent efficacy. Some situations, however, call for more rapid treatment or require a more convenient treatment regimen. For instance, a severely anemic woman requiring surgery or an anemic pregnant woman near term may benefit from a TDI, which necessitates an iron dextran preparation. 73 We strongly recommend the use of the low molecular weight preparation of iron dextran for TDI because of its significantly lower rate of life-threatening adverse events compared to the high molecular weight iron dextran formulation.
If IV iron is not successful or if there is a time pressure as with pregnancy near term or impending surgery, the addition of recombinant erythropoietin is effective. This has been shown even after iron has failed, shortening the response time compared with iron alone in both pregnant and nonpregnant women. 76,77
When the diagnosis is ACD (with or without IDA), treatment can be more challenging. Treating these women should begin with treatment of the underlying inflammatory condition. When this is not possible or if anemia treatment cannot wait, use of recombinant erythropoietin is appropriate. These agents are currently approved for treatment of ACD in cancer patients undergoing chemotherapy, patients with chronic kidney disease, and HIV patients undergoing myelosuppressive therapy. Their effectiveness ranges from 25% to 95% depending on the underlying condition. 63 It should be noted that particularly in patients with cancer and ACD, there are reports on erythropoietin's possible effect on promoting the underlying malignancy, as well as reports of increased risk of thrombotic events, myocardial infarction, stroke, and death that call for additional caution (see current labeling for these agents). 78
There is some controversy about the use of iron in ACD. The concern is that because iron is an essential nutrient for microorganisms, giving iron may increase the risk of bacteremia. In a study of dialysis patients receiving parenteral iron, those with a transferrin saturation >20% and a ferritin level >100 ng/mL had a higher risk of bacteremia than did controls. 79 On the other hand, there may be benefits to iron therapy. 63 Iron may reduce disease activity in rheumatoid arthritis and end-stage renal disease. Patients with inflammatory bowel disease and anemia show significant rise in Hb levels in response to iron treatment. Because of the poor absorption of iron from the intestine in ACD, the parenteral route must be used when iron is warranted. Based on current data, in cases of absolute iron deficiency accompanying ACD, patients should receive IV iron therapy. It should also be considered in patients unresponsive to erythropoietin treatment because of functional iron deficiency and in those whose ferritin level and transferrin saturation have dropped significantly as a result of intense erythropoiesis induced by erythropoietin treatment. This is supported by studies showing increased Hb levels in the absence of infectious complications. 79,80 Based on current information, patients with ACD and a high or normal ferritin level (>100 ng/mL) should not be given iron.
Conclusions
Anemia affects an enormous number of women of all ages, with a predilection for the less affluent. Its consequences are potentially serious at any age, ranging from possible developmental and learning problems in children and adolescents to serious maternal risks in pregnancy to mother-infant problems in the postpartum period and ultimately to increased mortality when associated with other medical conditions in older women. The vast majority of anemia in women is nutritional, generally iron deficiency, which is readily diagnosable and easily treated. Even the more complicated anemia of inflammation is responsive to intervention, with potentially dramatic benefits to its sufferers. It is our hope that this review will stimulate healthcare providers' interest in the condition and lead to development of better strategies to identify IDA early and treat it aggressively in order to improve quality of life and decrease serious morbidity for women everywhere.
Footnotes
Acknowledgments
The authors are members of the multidisciplinary Group for Research & Education on Anemia Therapy in Women (the GREAT Women Project), an initiative developed to extend knowledge, increase awareness, and improve treatment of anemia in women. Funding for this project was provided through the University of Arizona Office of Continuing Medical Education, with support from American Regent, Inc., and Luitpold Pharmaceuticals, Inc., and the Society for the Advancement of Blood Management (SABM).
Disclosure Statement
A.J.F. has been a speaker with honorarium for American Regent. A.S. has been a consultant for Bayer, Luitpold, Masimo, Novartis, Novo Nordisk, OrthoBiotech, and Zymogenetics, has received research and grant support from Bayer, Novartis, Novo Nordisk, OrthoBiotech, Pfizer, and ZymoGenetics, and has been a speaker with honorarium for Bayer, Novartis, OrthoBioetch, Zymogenetics, and Masimo. He is a founding member of SABM, where he currently serves as the President Elect. The other authors declare no competing financial interests.