
Abstract
Background:
Metabolic Syndrome (MetSyn) is one of the strongest predictors of type 2 diabetes (DM2) and cardiovascular disease (CVD). It is associated with a 4- to 10-fold increased risk of DM2 and a 2- to 3-fold increased risk of CVD. Low income and minority women have some of the highest rates of MetSyn. This study examines the effect of a unique, community based, primary prevention program on the rates of MetSyn and health habits.
Methods:
Sixty-four low income and minority women were enrolled in the HAPPY (Health Awareness and Primary Prevention in Your neighborhood) Heart Program in an eastern suburb of Boston. Over these 2 years, patients were evaluated by an interdisciplinary medical team: their primary physician, cardiologist, nutritionist, physical therapist, and health coach. The rate of MetSyn was measured at baseline, year 1, and year 2. Comparisons were made either using the paired t test for normally distributed variables or the Wilcoxon Sign test for non-normal variables.
Results:
The rate of MetSyn fell from 64.7% at baseline to 34.9% at year 1 (p=0.01) and 28.2% at year 2 (p<0.001). This was driven by increases in high-density lipoprotein (HDL-C) (p<0.001) and decreases in blood pressure (p=0.05). Fasting blood glucose trended down, but the hemoglobin A1c (HbA1c) reached significance (decreasing from 6 to 5.8, p<0.01). Nutrition and exercise habits trended toward improvement. There were significant decreases in anxiety (p<0.001), depression (p=0.006) and stress (p=0.002).
Conclusion:
This lifestyle intervention program is effective at decreasing MetSyn in a socioeconomically disadvantaged, largely minority, female population. This program also decreases anxiety, stress, and depression among participants.
Introduction
In the United States, more than 83 million Americans (30% of the population) currently live with cardiovascular disease (CVD). 1 In addition, 68 million have high blood pressure (HTN) and 71 million have high cholesterol (HL). 2 In recent decades, the mortality from CVD has decreased. However, the prevalence continues to be disproportionately high among women, racial and ethnic minorities, and socioeconomically disadvantaged groups. 3
Metabolic syndrome (MetSyn) includes risk factors for both type 2 diabetes (DM2) and CVD. Using the National Cholesterol Education Program/Adult Treatment Panel III (NCEP/ATP) 3 criteria, the presence of three of the following: abdominal obesity, hyperglycemia, dyslipidemia, and/or hypertension 4 confers a diagnosis of MetSyn and is an early risk factor for both DM2 and CVD. A diagnosis of MetSyn can identify “at risk” patients appropriate for aggressive lifestyle intervention. 5 –7 Even modest improvements in modifiable risk factors, such as the components of MetSyn, have exponential long-term benefits. 8 –10
Lifestyle intervention programs decrease CVD risk factors but it is unclear what, if any, effect they have on the rate of MetSyn. These programs contend that improvements in health will be more sustained if they result from fundamental changes in behavior, rather than pharmacologic temporizing. One of the first large lifestyle intervention programs for women, the WISEWOMAN study, showed a 7%–8% decrease in total cholesterol over 12 months in its North Carolina program and a 7%–9% decrease in hypertension over 1 year in its Massachusetts program. 11 Lifestyle programs typically include nutrition, exercise, and smoking cessation support. Newer programs incorporate relaxation, stress reduction, and aggressive medical management.
Unfortunately, many lifestyle intervention programs are only available as research pilots in large, academic medical centers. This decreases access for socioeconomically disadvantaged populations, which are often better served by community programs that minimize cost, transportation, language, and cultural barriers. 12, 13
Methods
Study design
The HAPPY (Health Awareness and Primary Prevention in Your neighborhood) Heart Study is a community based, lifestyle intervention program for low income and minority women, designed to decrease cardiovascular risk. It is based out of a community health center affiliated with Massachusetts General Hospital in the East Boston suburb of Revere, Massachusetts. The purpose of this study is to determine if a lifestyle intervention program can reduce the rate of MetSyn in a socioeconomically disadvantaged, largely minority population.
Inclusion criteria for the study, outlined in Fig. 1, include female gender, age 40–60 years, at least two CVD risk factors (as defined by the American College of Cardiology and the American Heart Association [ACC/AHA]), 14 income less than 200% federal poverty line (FPL), ability to speak Spanish or English, ability to consent, and a primary care physician at Massachusetts General Hospital. Exclusion criteria include history of coronary artery disease; peripheral vascular disease or stroke; significant renal, liver, or lung disease; valvular disease; ejection fraction less than 50%; cognitive dysfunction; and current/planned pregnancy.
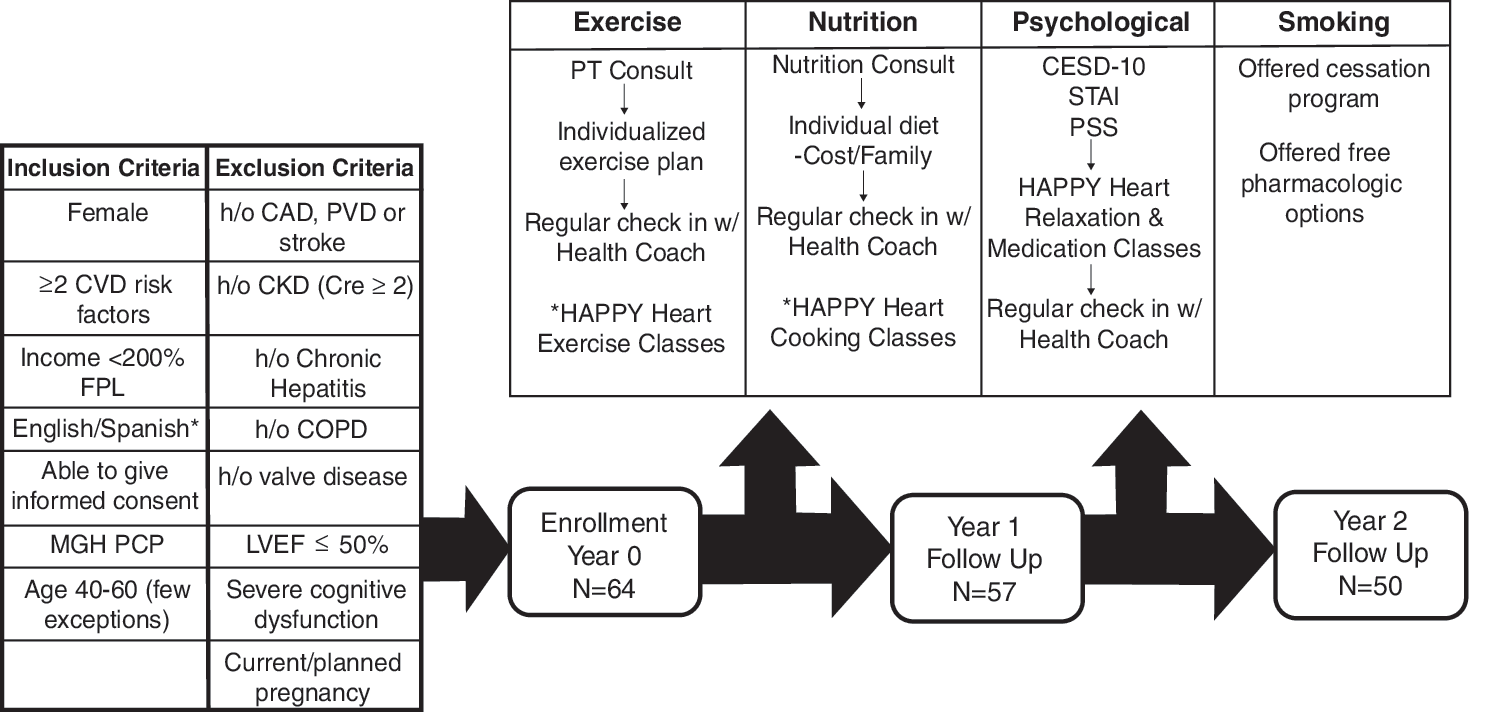
Overview of the HAPPY Heart Program. Patients were initially evaluated to determine if they meet inclusion/exclusion criteria. After enrollment, patients were set up with individualized exercise, nutrition, psychological and smoking cessation services as outlined above. At enrollment, 64 patients were included in the study. At year 1 there were 57 patients with complete data (7 lost/yr) and at year 2 there were 50 (7 lost/yr).
Once enrolled in the study, all women underwent a comprehensive history and physical, including laboratory work, electrocardiogram, and echocardiogram. The components of MetSyn were assessed and compared to the ATPIII criteria. 15 Abdominal obesity was defined as waist circumference>88 cm. 15 Lipids, including triglycerides (TG) and high-density lipoprotein (HDL-C), glucose and hemoglobin A1C were collected via fasting blood test. Systolic (SBP) and diastolic (DBP) were determined in clinic with 2 measurements taken after 5 minutes of quiet sitting. The average of the two measurements was used for analysis. In addition, demographic, economic, and lifestyle habits information was obtained. Nutrition, exercise, relaxation, and smoking habits were assessed via self-reported surveys. Psychosocial anxiety, depression, and stress were assessed via validated psychological questionnaires: the STAI for anxiety, 16 Center for Epidemiologic Studies Depression Scale (CESD)-10 for depression, 17 and Perceived stress scale (PSS) for stress. 18 The primary endpoint was the prevalence of MetSyn and its individual components at baseline, year 1, and year 2. Secondary endpoints included improvements in nutrition and exercise habits, psychosocial stress, and smoking.
Overview of the HAPPY Heart program
The HAPPY Heart program used a multipronged approach to lifestyle modification and cardiovascular risk reduction: health coaching, exercise, nutrition, stress reduction and smoking cessation (Fig. 1). After the baseline evaluation, study participants met with a physical therapist who designed an individualized exercise plan, taking into account baseline fitness level, relevant injuries, access to a gym, and time constrains. Free exercise classes were provided. The women also met with a dietician to determine a nutrition plan. These individualized plans factored in financial, cultural, and family/children's needs. Free cooking classes were available. Psychosocial stress was addressed via relaxation, meditation, and tai chi classes available to women at no charge. Smoking cessation classes and pharmacologic support was provided at no charge to any women who smoked. A health coach was assigned to each study participant. The health coach met with the patient in person on the phone 1–2 times a week for the first 3 months, then once a month thereafter. Each year, the woman underwent a comprehensive evaluation including history, physical, and lab testing annually. The results of the screenings and annual testing along with suggested management strategies were provided in written form to the primary care physician.
Complete demographic and biophysical information was collected on 64 patients at enrollment/baseline, 54 in year 1, and 50 in year 2 (Fig. 1). Complete past medical history and medication data was available for 64 patients at baseline, 49 in year 1, and 43 in year 2. This difference was due to incomplete patient questionnaires. Over 2 years of the study, 14 patients were lost to follow-up. Ten dropped out during the first year and four during the second year. Most of these patients were not available for contact after leaving the study, but among those available, “time constraints” were the most frequently cited reason for attrition.
Statistical analysis
Fisher's exact testing was used to compare the prevalence of MetSyn at baseline to years 1 and 2. For the individual MetSyn criteria, the Shapiro Wilk test was used to determine normality. For normal variables, the paired t-test was used to compare data year to year. For non-normal variables, the Wilcoxon Sign Test was used to compare baseline to year 1 and 2. All metabolic syndrome data is presented as mean±standard deviation format. For lifestyle habit data (nutrition, exercise, relaxation, and smoking status), the Wilcoxon Rank Sum test was used to compare baseline to years 1 and 2 nutrition data. Psychosocial stress scores were compared using the paired t-test. The frequency of regular exercise and smoking is displayed as a percentage. SPSS was used for all data analysis and a p value of <0.05 was considered significant. Study was carried out using an intention-to-treat analysis.
Results
Baseline demographics
Demographic data for the study participants is presented in Table 1. The average age at enrollment was 51.3 years. Just over half of the women self-identified as Caucasian, 42.2% were Latino, and 3.1% were African American. Almost 25% of participants had not completed the eighth grade. The majority had less than a high school education. Only 3 had a college/graduate degree. Many of the women worked; 37.5% were employed, and 21.9% were unemployed. The remaining 5 were disabled and/or retired. All women in the study had household incomes of < 200% FPL.
There is a high minority (45.3%) and non-English speaking population (40.6%). Almost all patients do not have a college degree, and 21.9% do not have a ninth grade education. Many (37.5%) are employed, but all have an income <200% of the federal poverty line.
HTN, HL, and DM2 medical history and medication information
Participant's history of hypertension (HTN), hyperlipidemia (HL), and type 2 diabetes (DM2) was assessed at baseline; additionally, whether they met ACC/AHA diagnostic criteria for these risk factors and whether or not they were on any medications was assessed annually (see Table 2). Antihypertensive medications included angiotensin-converting-enzyme (ACE) inhibitors, angiotensin receptor blockers, beta-blockers, calcium channel blockers, and diuretics. Hyperlipidemia medications included statins and fibrates; fish oil and omega-fatty-acid supplements were not included. Diabetes medications included sensitizers, secretagogues, alpha-glucosidase inhibitors, and insulin.
Assessed by patient report (history), cuff reading after 5 minutes of quiet sitting in clinic, or presence of at least one blood pressure medication.
Assessed by patient report (history), low-density lipoprotein level higher than recommended per American College of Cardiology -American Heart Association guidelines (based on other risk factors), or being on at least one hyperlipidemia medication.
Assessed by history; fasting blood glucose (FBG)>126; hemoglobin A1c (HbA1c)>6.5; either FBG>126 or HbA1c>6.5; or by being on at least one oral or injection diabetes medication.
Denotes significant value.
DM2, type 2 diabetes; HL, hyperlipidemia; HTN, hypertension.
At baseline, 62.5% of women had a history of HTN, 48.4% had a history of HL, and 21.9% had a history of DM2. These percentages did not change significantly year to year, but the overall trend decreased. The percentage of women with hypertensive blood pressure readings decreased significantly by year 1 and from year 1 to year 2. The number of women with a history of HL did not vary significantly year to year either, though again, the overall trend decreased. The percentage of women with low-density lipoproteins (LDLs) greater than goal (depending on diabetes status) decreased form baseline to year 1, but the difference did not reach significance. The percentage of participants reporting a history of diabetes did not change throughout the study. The number meeting DM2 diagnostic criteria by finger blood glucose (FGB) and hemoglobin A1c (HbA1c) values trended down but did not reach significance. Of note, there were more women meeting diagnostic criteria for DM2 using HbA1c criteria than by using fasting blood glucose (FBG) criteria.
The percentage of participants on antihypertensive medication remained stable over the 3 years. The use of statins and fibrates almost doubled, from 15.6% at baseline to 27.9% by year 2. The percentage of women on diabetes medications also increased from baseline (12.5%) to year 1 (20.4%) and then remained stable.
Metabolic syndrome at baseline, year 1, and year 2
The baseline prevalence of MetSyn in this population was quite high (62.7%). By year 1, the prevalence decreased to 34.9% (p=0.01), and by year 2, it decreased to 28.2% (p=0.001) (Fig. 2). After an extensive review of the women's medical records, despite the high prevalence of MetSyn among this study population, only 2 women had the phrase “metabolic syndrome” noted anywhere in their medical records.
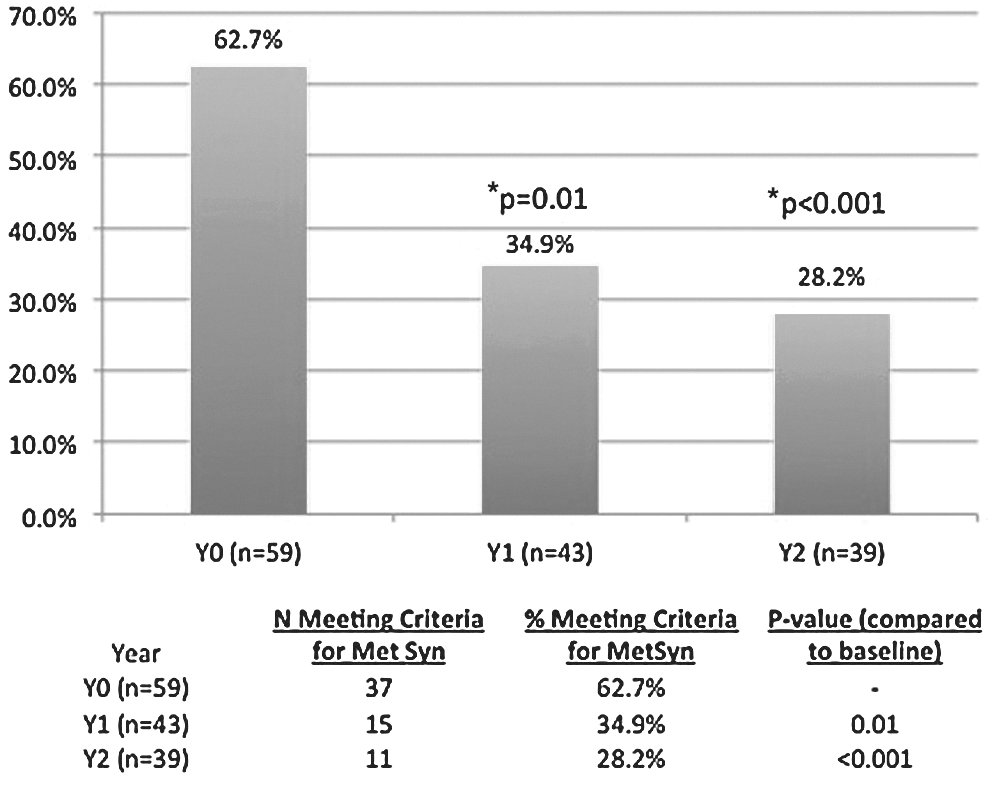
Rates of meeting diagnostic criteria for metabolic syndrome, i.e. having 3 of 5 components of metabolic syndrome, at baseline, year 1 and year 2. This figure displays the significant decrease from baseline to year 1 and from baseline to year 2 in the rate of metabolic syndrome. *Denotes significant value.
Components of metabolic syndrome at baseline, year 1, and year 2
Table 3 shows changes in the five components of MetSyn over the course of the study. When individually examined, decreases in changes HDL-C and blood pressure appear to drive the overall decrease in MetSyn. By year 2, improvements in HDL-C and blood pressure reached significance. HDL-C rose from a mean of 44.5mg/dL to 49.3mg/dL (p<0.001) and blood pressure fell from a mean of 129/79mmHg to 122/74mmHg (p=0.05). While the changes in waist circumference, TG, and FBG did not reach significance, the trends demonstrated improvement over time. Ultimately, the combined result of these changes resulted in a significant decrease in the overall MetSyn score at year 1 (p=0.017) and into year 2 (p<0.001).
Data displayed as mean±standard deviation.
The data show a significant decrease in high density lipoprotein (HDL) and blood pressure by year 2.
At year 1, the overall average number of metabolic syndrome components decreased and continued decreasing into year 2.
Hemoglobin A1c at baseline, year 1, and year 2
Given that diabetes is one of the most important predictors of future CVD in women and recent data suggests that HbA1c is a better marker of blood sugar over time 19 and a better predictor of future DM2 complications than FBG, 20 changes in HbA1c were examined separately (Fig. 3). There was a steady decrease in HbA1c during the study, which reached significance by year 2 (p<0.01).
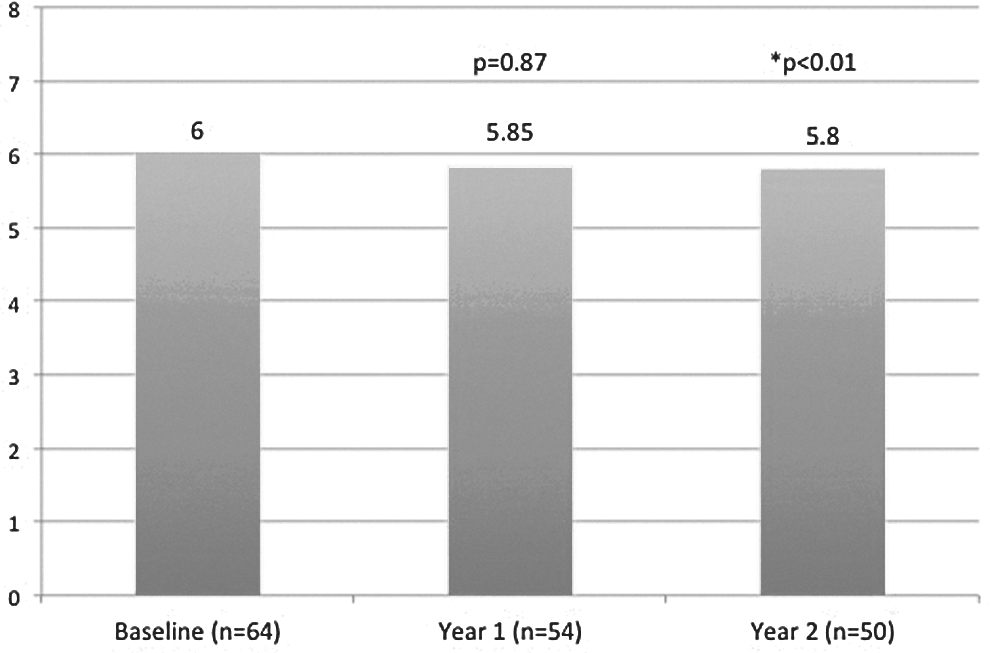
Average HbA1c value at baseline, year 1 and year 2. The decrease from baseline to year 1 did not reach significance but by year 2, the decrease reached significance.
Nutrition, exercise, relaxation, and smoking at baseline, year 1, and year 2
Table 4 shows improvements and trends in specific health behaviors over the 2 years. Nutritionally, the women skipped fewer meals, ate out less, and practiced portion control more (p<0.01). They ate fewer fatty (p=0.05) and sugary foods. They ate more fruits and vegetables. The number of women exercising regularly significantly increased by year 1 (p=0.02) but decreased somewhat again by year 2.
All continuous data presented as mean±standard deviation.
Nutrition question scales. Skips meals/portion control: Never=0; 1 × per week; 2 × per week=1; 3 × per week; 4 × per week=2; 5–6 × per week=3; daily=4.
Eating out: <2 × per week=0; 2–4 × per week=1; 5–7 × per week=2; >7 × per week=3.
Eat fatty/sugary/fruit/vegetables: Never=0; 1–2 × per day=1; 3–4 × per day=2; 5+× per day=4.
Relaxation Score Ranges. State-trait anxiety inventory (STAI) range, 20–80; Center for Epidemiologic Studies Depression Scale (CESD)-10 range, 0–30; Perceived stress scale (PSS) range, 0–40.
Denotes significant value.
The women had marked decreases in anxiety, stress, and depression at year 1 and 2. The state-trait anxiety inventory (STAI) scale ranges from 20 to 80, with higher scores indicating greater levels of anxiety. 16 The average score among participants fell from 33 to 25.5 over 2 years (p<0.001). The Center for Epidemiologic Studies Depression Scale (CESD)-10 score ranges from 0 to 30. Scores greater than 11 suggest depression. 17 The average participant score decreased from 10.5 to 7.5 in 2 years (p=0.006). The PSS stress score ranges from 0 to 40. Score greater than 12–14 suggest that a person is under stress. 18 The average score decreased from 17.78 to 14.15 (p=0.002).
There were many smokers in the study, 44% at baseline. The percentage of women who smoked trended down from 44% to 35% by year 1 and then plateaued at 33% for the second year.
Discussion
Despite advances over the last 50 years, CVD remains the leading cause of death among women, responsible for more deaths than all other causes combined. 14,21 Risk factors affect men and women differently. For example, in men, total cholesterol and LDL are the most predictive of future CVD. In women, HDL-C 22 and DM2, 23 not LDL, are the most powerful predictor of CVD. MetSyn is a strong predictor of both CVD 24 –26 and DM2. 27 –29 MetSyn has some advantages over traditional risk stratification models. It detects risk earlier than traditional models and can identify patients likely to benefit from early lifestyle changes. 6 While traditional risk assessment models underestimate CVD risk in women and minorities, MetSyn is more prevalent amongst women, minorities, and socioeconomically disadvantaged and may be more easily quantified and targeted for treatment by primary care practitioners. 30,31,32
There does continue to be controversy surrounding the predictive value of MetSyn. Some data suggest that after adjustment for obesity, MetSyn loses its predictive value for CVD, 33,34 and this has prompted the American Diabetic Association to issue a statement identifying eight concerns regarding the clinical utility of MetSyn. 35 While the predictive capacity of MetSyn remains in debate, the five risk factors, individually or in aggregate, are clearly markers for future CVD and identify patients in whom an aggressive management strategy should be implicated. More effective strategies to encourage and assess the adherence to lifestyle changes are also needed in this population.
When assessing patient history and medication usage, a decrease in self-reported “history” of HTN, HL, and DM2 was observed from year to year. Ideally, this reflects that as chronic diseases improve, patients view themselves as “cured” and may not report it. However, it is also possible that patients with chronic issues may be at the highest risk of attrition. More research is needed, since attrition is a major issue in all lifestyle/behavior programs. All of the women available for contact after dropping out of this study cited “time constraints” as a reason for attrition. This emphasizes the need for development and implementation of communication/assessment tools that do not require actual face-to-face visits, such as web-based programs and smart phone applications. In addition, 25% of the women in our study had limited education and/or were immigrants. They faced cultural, financial, and educational barriers. These factors must be considered when developing preventive strategies.
There was a significant drop in clinic BP readings, perhaps reflecting improved health or better medical management. Hyperlipidemia also demonstrated a downward trend. The decreases in FBG and HbA1c were smallest, reflecting the significant challenge of treating insulin resistance and diabetes. There was no change in the use of HTN medications but there was an increase in both HL and DM2 medications. This may reflect early improvement in blood pressure or simply the inherent variability of blood pressure measurements. The ongoing communication between the Happy Heart team and the primary care physician likely facilitated the more aggressive use of statins and hypoglycemic agents.
There was a high prevalence of MetSyn observed at baseline in this population, 62.7%, underscoring the need to develop effective risk reduction strategies for this population. The profound need is coupled with the challenge of providing care to patients with limited education and financial constraints. However, over 2 years, this program was associated with a significant drop in MetSyn prevalence, to 28.2%, driven primarily by increases in HDL-C and decreases in blood pressure. There were trends toward decreases in triglycerides, waist circumference, and FBG, but they did not reach significance. This observation suggests that even minor improvements in individual components of MetSyn (risk factors) can result in significant decreases in the rate of MetSyn. HbA1c was examined separately because it is more sensitive and better able to detect early diabetes and smaller changes in management. In this study both FBG and HbA1c trended down, and the decrease in HbA1c reached significance.
This study also examined lifestyle habits, specifically, nutrition, exercise, relaxation, and smoking. Nutrition habits tended toward improvement and there was an increase in the percentage practicing portion control. This is likely because it is one of the easiest and cheapest changes to make to a diet. Interestingly, there was a marked increase in exercise at year 1 but it tailed off into year 2, likely reflecting the initial enthusiasm surrounding a new exercise program and the subsequent evaporation thereof. Significant improvements were seen in all 3 areas of psychosocial stress at year 1 and continued into year 2. This is the first study of its kind to demonstrate simultaneous improvements in cardiovascular risk and psychosocial stressors in a lifestyle intervention study. More research is needed to define the relationship between these variables, particularly in socioeconomically disadvantaged populations, where baseline levels of psychosocial stress can be higher than average. Finally, little improvement was made in smoking habits, reflecting the challenging nature of treating addictions.
The HAPPY Heart study is significant not only because it shows the association between lifestyle intervention programs and decreases in the rate of MetSyn, but also because it does so in a challenging-to-treat population. The HAPPY Heart program had many unique features. First, it was centered in a community health center, geographically close to the women it served. This improved the ease with which women could attend appointments and classes. The program was organized and run by women working within the community. Education and exercise classes were available in English and Spanish, and a live interpreter was available for all appointments. There were no direct enrollment costs and all classes were free. The indirect costs of transportation, missed work, childcare, etc. were all minimized by the location and timing of the program's services. Finally, and perhaps most importantly, the women created a community of support for one another. The study focused on a specialized subset of the population, so many of outside stresses (financial stress, parent/child stress, social stress, etc.) encountered by the women, were common among the participants. In addition to becoming a place where the women came for education and exercise, the HAPPY Heart events and classes became a psychologically therapeutic experience for many of the women. These valuable lessons can be extrapolated to other and future lifestyle and prevention programs. Another unique component of the study was the interaction between the Happy Heart Team and the primary care physicians. The ongoing feedback provided to the team supports the notion that a more group-based approach to aggressive primary prevention may be feasible in this population. This team-based approach to a primary preventive strategy with emphasis on lifestyle changes and aggressive medical management when appropriate clearly affected the psychological and physical well-being of the participants in this study.
The primary limitation of this study is its small sample size at a single site. While this is due in large part to the challenging nature of the studied population (many of whom are single mothers and grandmothers providing full time childcare), it limits the generalizability of our results. Nevertheless, it provides a unique opportunity to develop an intervention to be refined in a larger population in the future. The study also has the potential to be influenced by selection bias given that the study was not randomized and this was not a complete census sample. Finally, the study follows the women only over 2 years. This is problematic for two reasons. First, it may not be long enough to observe all of the improvement resulting from the intervention or the collection of cardiovascular events. Also, is does not allow the sustainability of the results to be fully evaluated.
Future research will further refine intervention in a larger population in the attempt to replicate and validate these results. Ultimately, a randomized control trial of the HAPPY Heart Program would quantify the benefits of this type of intervention over “standard care,” incorporating a cost-effectiveness analysis to determine the large-scale applicability of this program.
Footnotes
Acknowledgment
The authors would like to acknowledge Linda Hemphill, MD, and Nandita Scott, MD, for their many contributions to this research.
Author Disclosure Statement
No competing financial interests exist.