
Abstract
Background:
Modification of traditional cardiac risk factors is an important goal for patients after an acute myocardial infarction (AMI). Risk factor prevalence and secondary prevention efforts at discharge are well characterized among older patients; however, research is limited for younger and minority AMI populations, particularly among women.
Methods:
Among 2369 AMI patients enrolled in a 19-center prospective study, we compared the prevalence and cumulative number of five cardiac risk factors (hypertension, hypercholesterolemia, current smoking, diabetes, obesity) by age, sex, and race. We also compared secondary prevention strategies at discharge for these risk factors, including prescription of antihypertensive or lipid-lowering medications and counseling on preventive behaviors (smoking cessation, diabetes management, diet/weight management).
Results:
Approximately 93% of patients had ≥1 risk factor, 72% had ≥2 factors, and 40% had ≥3 factors. The prevalence of multiple risk factors was markedly higher for blacks than for whites within each age-sex group; black women had the greatest risk factor burden of any subgroup (60% of older black women and 54% of younger black women had ≥3 risk factors). Secondary prevention efforts for smoking cessation were less common for black compared with white patients, and younger black patients were less often prescribed antihypertensive and lipid-lowering medications compared with younger white patients.
Conclusions:
Multiple cardiac risk factors are highly prevalent in AMI patients, particularly among black women. Secondary prevention efforts, however, are less common for blacks compared to whites, especially among younger patients. Our findings highlight the need for improved risk factor modification efforts in these high-risk subgroups.
Introduction
Eliminating health disparities and improving cardiovascular health through prevention, detection, and treatment of risk factors are national public health and research priorities. 1,2 Hypertension, hypercholesterolemia, cigarette smoking, diabetes mellitus, and obesity are well established and potentially modifiable risk factors for both the development of coronary heart disease (CHD) and adverse cardiac events and mortality. 3 –5 Clinical guidelines recommend modification of these risk factors with both discharge medications and secondary prevention programs, based upon their demonstrated efficacy in randomized clinical trials. 6 –8 The prevalence of these risk factors and secondary prevention efforts at discharge are well characterized among older adults, and a number of studies have assessed patterns in risk factors by age and sex, with some inconsistencies in conclusions. 9 –13 However, research is limited for younger and minority populations of acute myocardial infarction (AMI) patients, particularly women, and how their risk factor prevalence and secondary prevention treatments compare with older and white patients. There are few comparisons of risk factors among subgroups defined by age, sex, and race.
Identifying patients in need of multiple risk factor management, as well as understanding the utilization of discharge medications and other secondary prevention efforts post-AMI, may help target intervention strategies to decrease the risk for recurrent events and improve patient outcomes in more vulnerable populations. Accordingly, we compared the prevalence, cumulative number, and clustering of five potentially modifiable CHD risk factors by age (<55 or ≥55 years), sex, and race (white or black), using data from a multisite observational cohort of hospitalized AMI patients. Given our focus on modifiable risk factors, we also compared secondary prevention strategies at discharge, including both medication and counseling on preventive behaviors.
Methods
Participants
Between January 2003 and June 2004, 2498 AMI patients were consecutively recruited from 19 U.S. centers to participate in the Prospective Registry Evaluating Myocardial Infarction: Events and Recovery (PREMIER) study. The methods of PREMIER have been described previously. 14 In brief, eligible patients were age ≥18 years with elevated cardiac enzymes (troponin I/T or creatine kinase-myocardial band fraction above the upper reference limit of the recruiting center) within 24 hours of hospital admission and additional evidence supporting AMI (>20 minutes of ischemic symptoms or electrocardiographic ST changes). Patients must have presented directly to the enrolling site or been transferred within the first 24 hours of presentation. Patients who were incarcerated, developed elevated cardiac enzymes because of elective coronary revascularization, or did not speak English or Spanish were excluded. We limited study analyses to the 2369 patients who were of white or black race, because of the small proportion of patients representing other races (n=129 [5%]). Institutional Review Board approval was obtained at each participating institution, and patients provided informed consent for their study participation.
Data collection
Data were collected by medical chart abstraction and in-person patient interviews within 24 to 72 hours of hospital presentation. Sociodemographic factors included age (<55 or ≥55 years), sex, self-identified race (white or black), education greater than high school level, insurance type (Medicaid, Medicare, commercial/preferred provider organization, health maintenance organization, none/self-pay), reported avoidance of health care in the past because of cost, and household income <$10,000. Medical history data were abstracted for AMI, angina, percutaneous coronary intervention, coronary artery bypass graft surgery, congestive heart failure, cerebrovascular accident, peripheral arterial disease, and prior coronary stenosis >50%.
The presence of five potentially modifiable risk factors was determined using data from both the medical record (hypertension, hypercholesterolemia, diabetes, obesity) and the patient interview (current smoking). Hypertension was defined as systolic blood pressure >140 mmHg or diastolic blood pressure >90 mmHg within 48 hours of hospital discharge or a history of hypertension documented in the medical record. Hypercholesterolemia was defined as total cholesterol >240 mg/dL, a history of high cholesterol documented in the medical record, or use of lipid-lowering agents at hospital presentation. Patients reporting a history of smoking within the past 30 days were categorized as current smokers. Diabetes was considered present if documented in the medical record. Obesity was defined as a body mass index (BMI) ≥30 kg/m2 at hospital discharge, using abstracted height and weight data. In supplementary analyses, additional risk factor definitions were explored, including hypertension defined according to a documented history in the medical record and obesity categorized further into overweight/obese (BMI≥25 kg/m2) and morbidly obese (BMI≥40 kg/m2).
Secondary prevention efforts at discharge were abstracted from the medical record and included prescription of medications and counseling on preventive behaviors for patients with the corresponding risk factor. The receipt of secondary prevention was defined as a documented prescription at discharge for an antihypertensive medication (angiotensin-converting enzyme inhibitor, angiotensin II receptor blocker, beta blocker, calcium channel blocker, beta agonist, or diuretic) among patients with hypertension or for a lipid-lowering medication (statin or other antihyperlipidemic medication) among patients with hypercholesterolemia. For the remaining three risk factors, secondary prevention was defined as instruction on smoking cessation among reported current smokers, instruction on diabetes management among patients with diabetes, and instruction on diet and weight management among obese patients.
Statistical analysis
Patient sociodemographic characteristics, medical history, prevalence of individual risk factors, and receipt of secondary preventive medications and counseling at discharge were compared among subgroups defined by age, sex, and race, using Pearson chi-square tests. The cumulative number of risk factors was determined for each patient (possible range from 0 to 5) and compared among age, sex, and race subgroups. Because it is unclear whether obesity is an independent risk factor for CHD or correlated with known risk factors, 15 we excluded obesity in the cumulative risk factor count in sensitivity analyses. The observed and expected prevalence of each of the 32 possible combinations of the five risk factors was determined, with the expected prevalence calculated as the product of the individual probabilities of each risk factor in the cohort. Clustering occurs when the observed prevalence of a combination of risk factors is greater than the expected prevalence (i.e., observed/expected ratio >1.0). 16 Analyses were performed using SAS version 9.2 (SAS Institute Inc., Cary, North Carolina), and tests for statistical significance were two-tailed with α=0.05.
Results
The 2369 patients included in this study were, on average, 61 years old and were predominately male (67%) and white (78%). Approximately one-third of patients were under 55 years old, and 21% had experienced a previous AMI. Within each age-sex group, black patients were more likely than white patients to rely on Medicaid as their primary insurer, have no education beyond the high school level, have a household income of less than $10,000, and have a history of congestive heart failure (Table 1). Younger black men and older black women were more likely than their white counterparts to have avoided getting health care in the past, owing to cost, and have experienced a previous AMI. Black men, regardless of age, were more likely than white men to have had a prior cerebrovascular accident.
Approximately 93% of patients had at least one of the five risk factors on admission (Fig. 1). Hypertension was the single most common risk factor, with an overall prevalence of 64% and a range from 46% in young white men to 90% in older black women (Fig. 2). Within each age-sex group, a greater percentage of black patients than white patients had hypertension. This pattern remained unchanged when elevated blood pressure was removed from the definition for hypertension (data not shown). Black patients also had a greater prevalence of diabetes than white patients within each age-sex group; however, this race difference was not statistically significant for young women. Older black men had a greater prevalence of smoking than similarly aged white men, but no differences were observed in the younger age group. There was no significant race difference in the prevalence of hypercholesterolemia or obesity among any of the age-sex groups. Further categorization of BMI into overweight/obesity and morbid obesity revealed a greater prevalence of overweight/obesity among white compared to black men, regardless of age (young men: 83.9% versus 71.5%, p=0.001; older men: 76.9% versus 66.9%, p=0.017), but no race difference among women. No race difference in the prevalence of morbid obesity was observed for any of the age-sex subgroups.
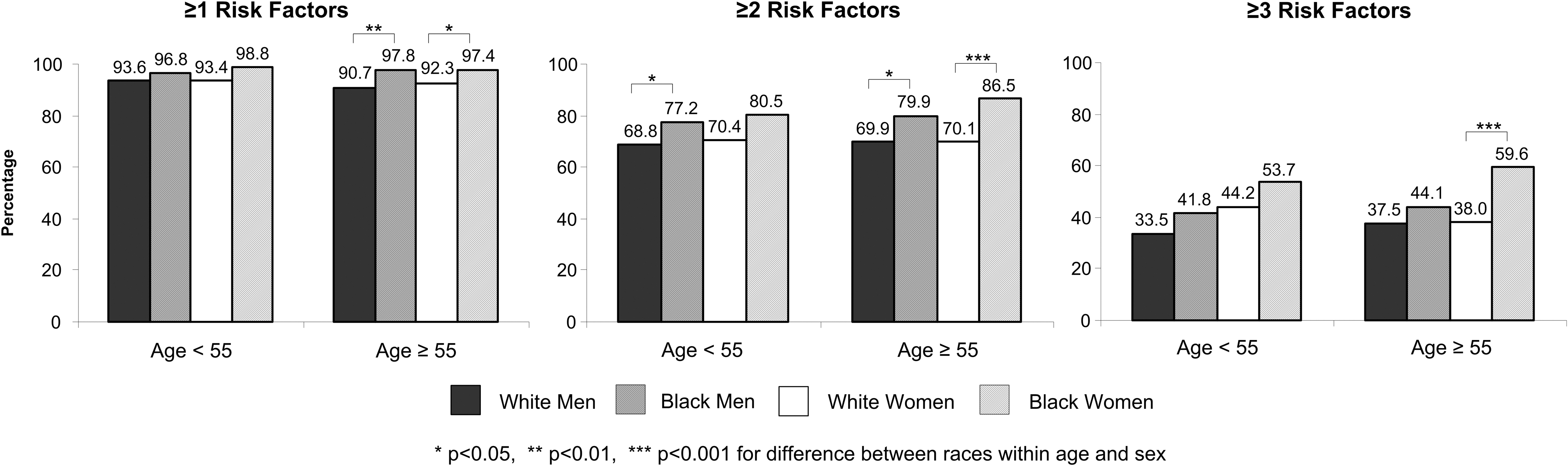
Prevalence of multiple risk factors by age, sex, and race. Percentage of patients with at least one, two, or three of the following risk factors: hypertension, hypercholesterolemia, current smoking, diabetes, and obesity.
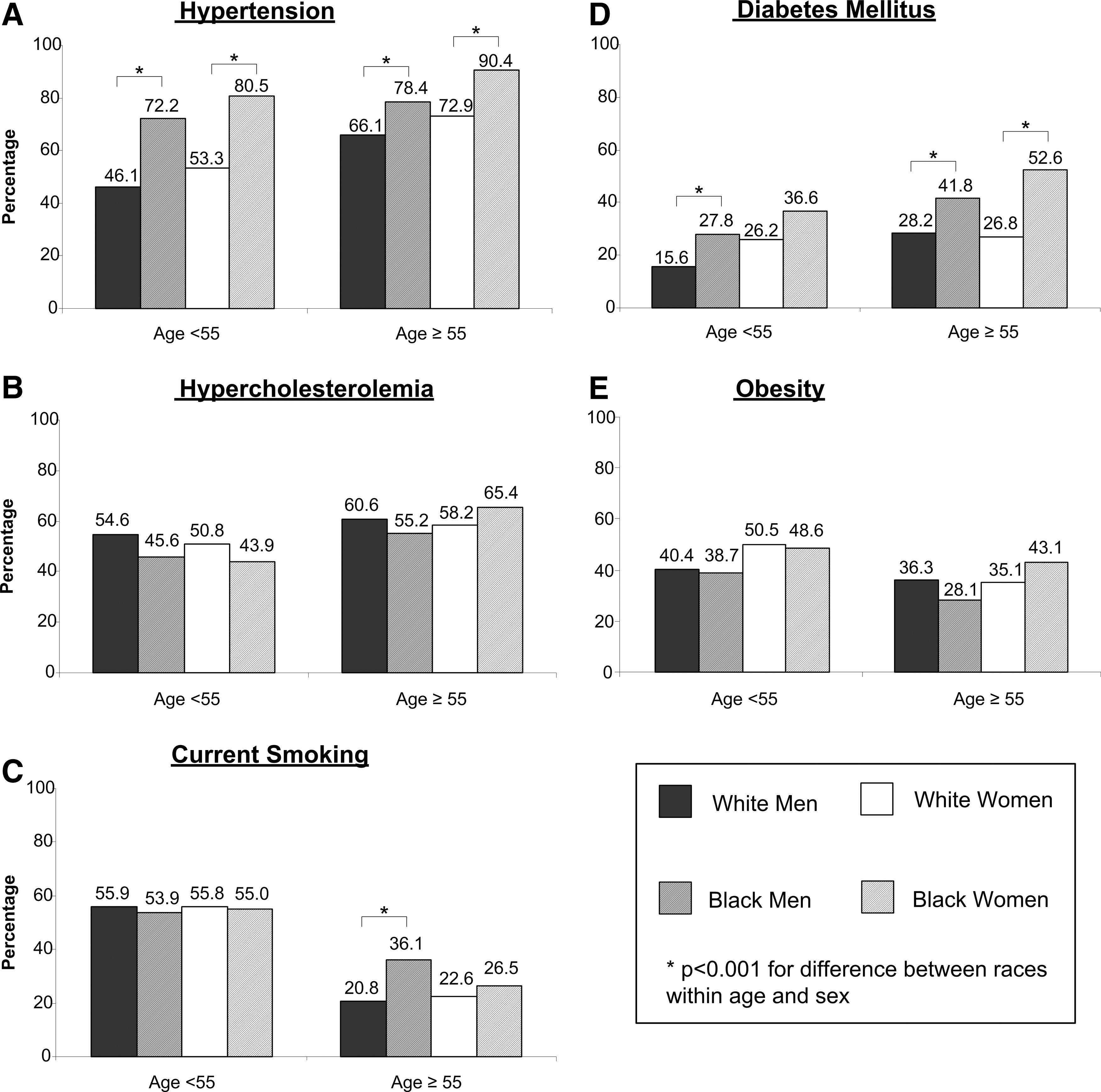
Prevalence of individual risk factors by age, sex, and race.
Risk factors frequently co-occurred (Fig. 1). Approximately 72% of patients had at least two risk factors, and 40% had three or more risk factors. Although only 2% of patients had all five risk factors, this combination occurred more frequently than that expected if the risk factors were independent (Table 2). Other potential clusters of risk factors included hypertension, hypercholesterolemia, diabetes, and obesity; hypertension, hypercholesterolemia, and diabetes; and smoking and obesity. Smoking was the only individual risk factor to occur in isolation more frequently than expected if the five risk factors were independent; diabetes was the least likely to occur in isolation.
+, presence of risk factor; −, absence of risk factor; E, expected prevalence of the combination of risk factors; O, observed prevalence of the combination of risk factors.
The prevalence of multiple risk factors was higher for blacks than for whites within each age-sex group, though differences did not reach statistical significance for all subgroup comparisons (Fig. 1). Black women had the greatest risk factor burden (60% of older black women and 54% of younger black women had three or more risk factors). Sensitivity analyses that excluded obesity showed consistent patterns across subgroups, with black women continuing to have the greatest risk factor burden.
Receipt of relevant secondary preventive medications and counseling varied across subgroups defined by age, sex, and race (Fig. 3). Young black men were less likely than young white men to receive antihypertensive medications, lipid-lowering medications, and smoking-cessation counseling. Similarly, young black women were less likely to receive lipid-lowering medications and smoking-cessation counseling than young white women. For both sexes, older black patients were less likely to receive smoking-cessation counseling than older white patients. No significant race difference in the receipt of diabetes or diet/weight counseling was observed for any of the age-sex groups.
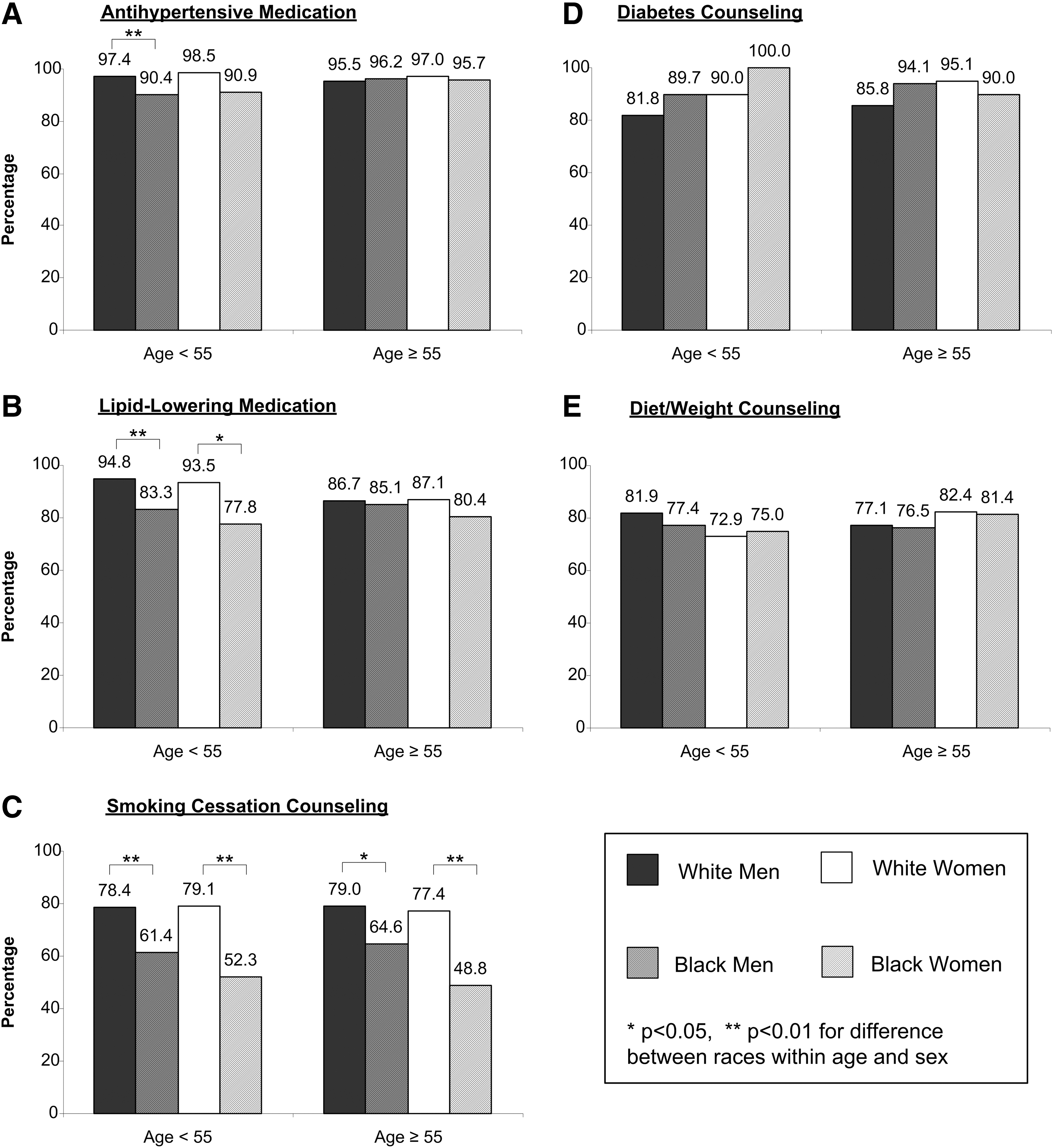
Receipt of relevant secondary preventive medications and counseling by age, sex, and race.
Discussion
In this multicenter study of hospitalized AMI patients, more than 90% of patients presented with at least one risk factor, and 40% presented with three or more risk factors. The burden of multiple factors was highest for black women, with 6 out of 10 older women and 5 out of 10 younger women having three or more risk factors on admission. Despite the generally higher risk factor burden for black patients, secondary prevention efforts for smoking cessation were less common for black than for white patients, and younger black patients were less often prescribed antihypertensive or lipid-lowering medications than were younger white patients.
Our results are consistent with multiple studies reporting that 80% to 90% of AMI patients present with at least one traditional CHD risk factor. 9,11 –13 Prior studies examining the prevalence of multiple risk factors have generally shown that 50% to 60% of AMI patients present with at least two factors and that 20% to 30% present with at least three factors. 9,11,13 We observed slightly higher rates in our cohort, with 72% of patients having two or more risk factors and 40% having three or more risk factors. In part, these differences likely reflect differences in patient populations and choice of risk factors. For example, one of these prior studies analyzed a geographically limited population, 11 one included only four risk factors, 13 and one included family history rather than obesity as the fifth risk factor. 9
The cumulative number of risk factors varied across demographic subgroups in our study. Although a number of prior studies have compared risk factors among AMI patients by sex and age, 9 –13 with some inconsistencies as to whether patterns differ by these characteristics, few studies have made comparisons by race. 9,13 Reports from both the National Registry of Myocardial Infarction (NRMI) 9 and the Can Rapid Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the American College of Cardiology/American Heart Association Guidelines (CRUSADE) National Quality Improvement Initiative 13 show that AMI patients with multiple traditional risk factors are younger and more often of minority race; however, the rates were not reported by age, sex, and race subgroups. Our results show unfavorable risk factor profiles across age-sex-race subgroups, as well as highlight the disproportionate risk factor burden for black women.
Our study also found marked variation in receipt of smoking-cessation counseling, antihypertensive medications, and lipid-lowering medications for black patients, particularly younger patients. Such secondary preventive efforts at discharge are recommended by clinical guidelines and are used as quality-of-care measures for AMI patients. 8,17 –20 Our findings, in concert with those of prior studies showing variation in these important secondary prevention efforts by demographic characteristics, 21 –25 highlight missed opportunities for targeted risk factor modification efforts, especially for younger black patients.
Several issues should be considered when interpreting our results. We relied primarily on data recorded in the medical chart, and it is possible that differences in documentation of risk factors, medication history at presentation, or prehospital care may influence the ascertainment of risk factor status. Additionally, we focused on the presence of modifiable risk factors rather than level of control. The documentation of counseling may not be an accurate reflection of whether risk factor counseling indeed occurred. 21,26 Although patients were recruited between 2003 and 2004, the patterns by age and sex are consistent with recently published findings reflecting a similar time period, 9,10 and they build upon prior work by providing detail by age-sex-race subgroups. Finally, results from this multicenter study of hospitalized white and black AMI patients, which included a variety of institution types and geographic locations across the U.S., may not generalize to AMI patients seen at other institutions, patients who do not speak English or Spanish, and those who are not of white or black race.
Conclusions
Currently, there are an estimated 15.4 million Americans with diagnosed CHD 27 for whom risk factor modification can reduce the risk of recurrent events and death. 20 Our study has shown a high prevalence of multiple traditional, and potentially modifiable, CHD risk factors among patients hospitalized for AMI. There was heterogeneity across demographic subgroups in the prevalence of these risk factors, as well as the receipt of secondary prevention strategies at discharge. Our results highlight missed opportunities for both prevention of traditional risk factors and management of the risk factors following AMI, particularly for women and minority patients. Given the importance of secondary prevention, 6 –8,17 –19 identifying the factors that contribute to effective risk factor management among demographic subgroups is critical.
Footnotes
Acknowledgments
PREMIER was supported principally by CV Therapeutics, Inc., with funding for all analyses from CV Outcomes, Inc. We also acknowledge Mitra Daneshvar for her invaluable assistance in the review of the literature and preparation of tables and figures for the manuscript.
Author Disclosure Statement
No competing financial interests exist.