
Abstract
Background:
This study evaluates the differences between women and men in medication use, medication adherence, and prescribing alignment with clinical guidelines.
Methods:
We conducted an analysis of pharmacy and medical claims for 29.5 million adults with prescription benefits administered by a pharmacy benefits manager in the United States, age 18 and older, between January 1, 2010, and December 31, 2010. Prevalence and intensity of medication use were evaluated by sex, age group, and medication type (acute vs. chronic). Medication adherence was measured by the percentage of patients with a medication possession ratio (MPR) ≥80%. The percentage of patients receiving guideline-based treatment was measured for diabetes and select cardiovascular conditions.
Results:
The study population comprised 16.0 million women and 13.5 million men with continuous pharmacy benefit eligibility. Women were significantly more likely than men to use one or more medications during the analysis period (68% vs. 59%, respectively, p<0.001), and women used more unique medications, on average, than men (5.0 vs. 3.7 medications per year, respectively, p<0.001). Differences in drug utilization were observed for all age groups and medication types. For all clinical metrics evaluated, women were less likely than men to be adherent in their use of chronic medications, and they were less likely to receive the medication treatment and monitoring recommended by clinical guidelines.
Conclusions:
There are significant disparities between women and men in their intensity of medication use, their adherence to medications, and their likelihood of receiving guideline-based drug therapy. These differences may indicate a need for more personalized drug selection and therapeutic management to improve clinical outcomes.
Introduction
S
Beyond clinical guidelines for diagnosis and treatment, there are many other variables that affect prescribing decisions and the outcomes of treatment. 8 Physician prescribing choices may be affected by perceptions of gender differences, 9,10 and the response to a drug can be strongly affected by a patient's adherence to the prescribed treatment. 11 –13 These factors may contribute to gender differences in treatment that increase the risk of suboptimal outcomes.
In this observational study, we evaluate sex differences in medication use, medication adherence, and guideline-based prescribing for a large, representative population of commercially insured adults in the United States. To our knowledge, no comparable large-scale analysis of sex differences in current medication practice has been reported. Our objective is to provide a benchmark of medication prescribing and adherence in the current practice environment, where sex-specific prescribing guidelines have not yet been widely implemented. It is important to understand the scope and sources of sex and gender differences in current clinical practice as a starting point for developing new clinical strategies and treatment interventions. 6
Materials and Methods
Study design
We conducted an analysis of de-identified pharmacy and medical claims data for a large population of adults in the United States during the time period from January 1 to December 31, 2010. The study population comprised all eligible members of pharmacy benefit plans managed by Medco Health Solutions (now Express Scripts) on behalf of plan sponsors throughout the United States. Plan sponsors included employers, health plans, government agencies, and union groups. Members included in the study had continuous pharmacy benefit coverage during the time period of the study, and they were age 18 or older at the onset of the study period. “Members” included all covered adults, not just the primary insured. All available claims during the 1-year study period were included in the analysis.
Prescription drug utilization, benefit eligibility, and patient characteristics were derived from data maintained by the pharmacy benefits manager. Pharmacy claims data included medication name and strength, date of fill, days' supply, and medication cost (average plan cost and patient out-of-pocket cost). Eligibility data included members' sex, date of birth, and dates of benefit eligibility. Medical claims were evaluated to identify medical conditions and laboratory test utilization during the study period, using data supplied by the medical plans.
Measures
The primary measures of drug utilization were prevalence of use (the percentage of members who used one or more medications during the study period) and intensity of use (the average number of distinct medications used during the study period). These measures were evaluated by age group (18–44, 45–64, and 65 years or older), by medication type (acute vs. chronic), and by sex (women vs. men). Medications were defined by chemical entity; a different dose or formulation of the same compound was considered the same medication. Chronic medications are commonly indicated for a chronic condition and are often used for more than 1 year, such as antihypertensives and oral diabetes medications. Acute medications are generally used on a short-term basis (less than 1 year), such as antibiotics and cough medications. For women, utilization rates for chronic medications were evaluated with and without the inclusion of hormonal contraceptives (oral, transdermal, vaginal, or injectable). Hormonal contraceptives are commonly assumed to be a primary driver of medication use in women aged 18–44 years. Plan members who used one or more medications during the year were considered to be “patients.” The average number of medications used by patients was evaluated by sex, age group, and medication type. Average annual drug costs were calculated on a per-patient basis. The analyses of drug utilization and cost spanned all classes of prescription drugs.
Medication adherence was evaluated using a medication possession ratio (MPR), defined as the number of days of medication supply divided by the number of days between the first and last medication refill dates; the analysis period for each patient was variable up to 12 months. Medication adherence was measured for select classes of cardiovascular and oral diabetes medications. For combination treatment with two or more medications, such as multiple oral diabetes or antihypertensive medications, a weighted cumulative MPR was computed. Patients with MPR ≥80% were considered “adherent.” The use of prescription claims data as a basis for measuring medication adherence has been validated in prior studies. 14,15
The percentage of patients receiving guideline-based treatment for diabetes and cardiovascular conditions was evaluated for 14 metrics derived from evidence-based clinical practice guidelines. 16 –19 For diabetes metrics, patients were identified based on their use of oral or non-oral diabetes medications during the analysis year. Self-monitoring of blood glucose was identified based on pharmacy or medical claims for blood glucose test strips in patients who were taking insulin. Use of laboratory tests was identified using current procedural terminology codes in medical claims. For cardiovascular metrics, patients were identified based on use of cardiovascular medications and International Classification of Diseases, Ninth Revision (ICD-9) codes in medical claims data. Treatment alignment with the clinical metrics was evaluated using pharmacy claims, medical claims, or both. Rates of guideline-based care were compared for men and women.
Statistical analysis
For prevalence and adherence measures, the statistical significance of differences was evaluated using z tests. Differences in drug utilization, drug costs, and treatment alignment were evaluated using two-sided t tests. Data analysis was conducted using structured query language (SQL), and statistical tests were performed in Microsoft® Excel® 2007 (Microsoft Corp.).
Results
Study population
The study population comprised 16,012,060 women and 13,458,395 men ages 18 and older who were members of prescription benefit plans in the United States during 2010 (Table 1).
Prevalence of medication use
The percentage of women who used one or more medications during the analysis year was significantly higher than the percentage of men (67.5% vs. 58.9%, p<0.001) (Table 2; Fig. 1). A significant prevalence difference was also found for acute medications and chronic medications, measured separately. The size of the difference varied by age group—there was a large sex difference in the overall use of medications by younger adults (ages 18–44; 64.1% of women vs. 48.6% of men, p<0.001), but the difference was much smaller in older adults (ages 65 and older; 71.9% of women vs. 69.4% of men, p<0.001). These age-related variations were observed for both acute medications and chronic medications.
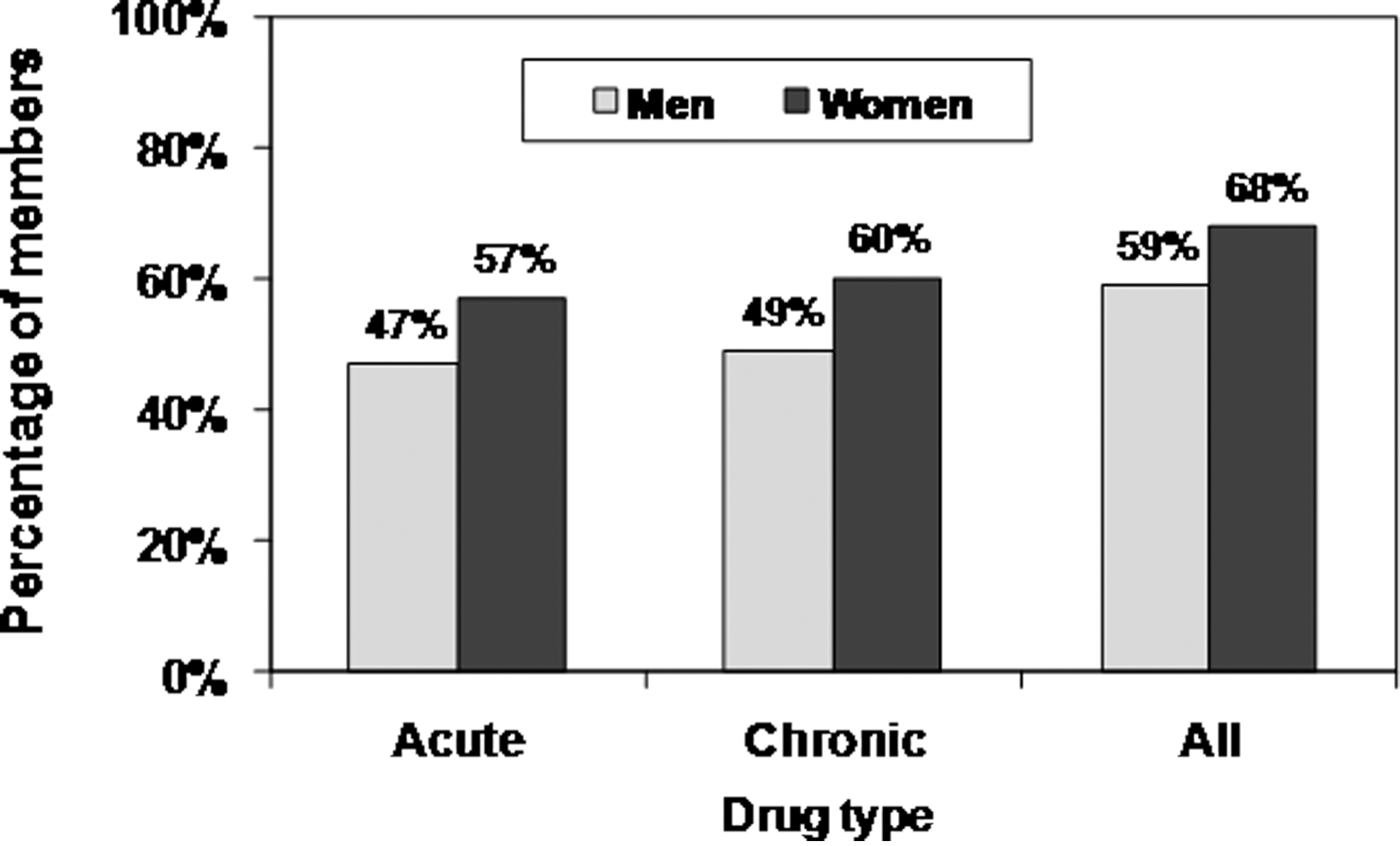
Prevalence of medication use by members of pharmacy benefit plans: United States, 2010.
Prevalence is the percentage of insured individuals who used one or more medications during the analysis year (2010). All pairwise differences between prevalence rates for women and men are statistically significant (p<0.001). Sample sizes are reported in Table 1.
HC, hormonal contraceptives.
Drug utilization: per-member analysis
Among members, women used more medications than men during the 12-month study period (mean number of medications: 5.0 for women vs. 3.7 for men, p<0.001) (Fig. 2). The difference in use was larger for acute medications than for chronic medications; use of acute medications averaged 2.2 for women versus1.5 for men (p<0.001), but the difference was proportionately smaller for chronic medications. Women's use of acute medications was relatively constant across age groups, but their use of chronic medications increased sharply with age (Fig. 3). Hormonal contraceptives were a significant contributor to medication use by younger women (approximately 15% of medication use for women ages 18–44). Men's use of medications increased progressively with age for both acute medications and chronic medications (Fig. 4). The pattern of acute medication use was different for men and women. Younger men made far less use of acute medications than did younger women (ages 18–44, mean number of medications: 2.0 for women vs. 1.1 for men), but the use of acute medications by older men and women (ages 65 and older) was similar.

Average number of prescription medications used by benefit plan members: United States, 2010.
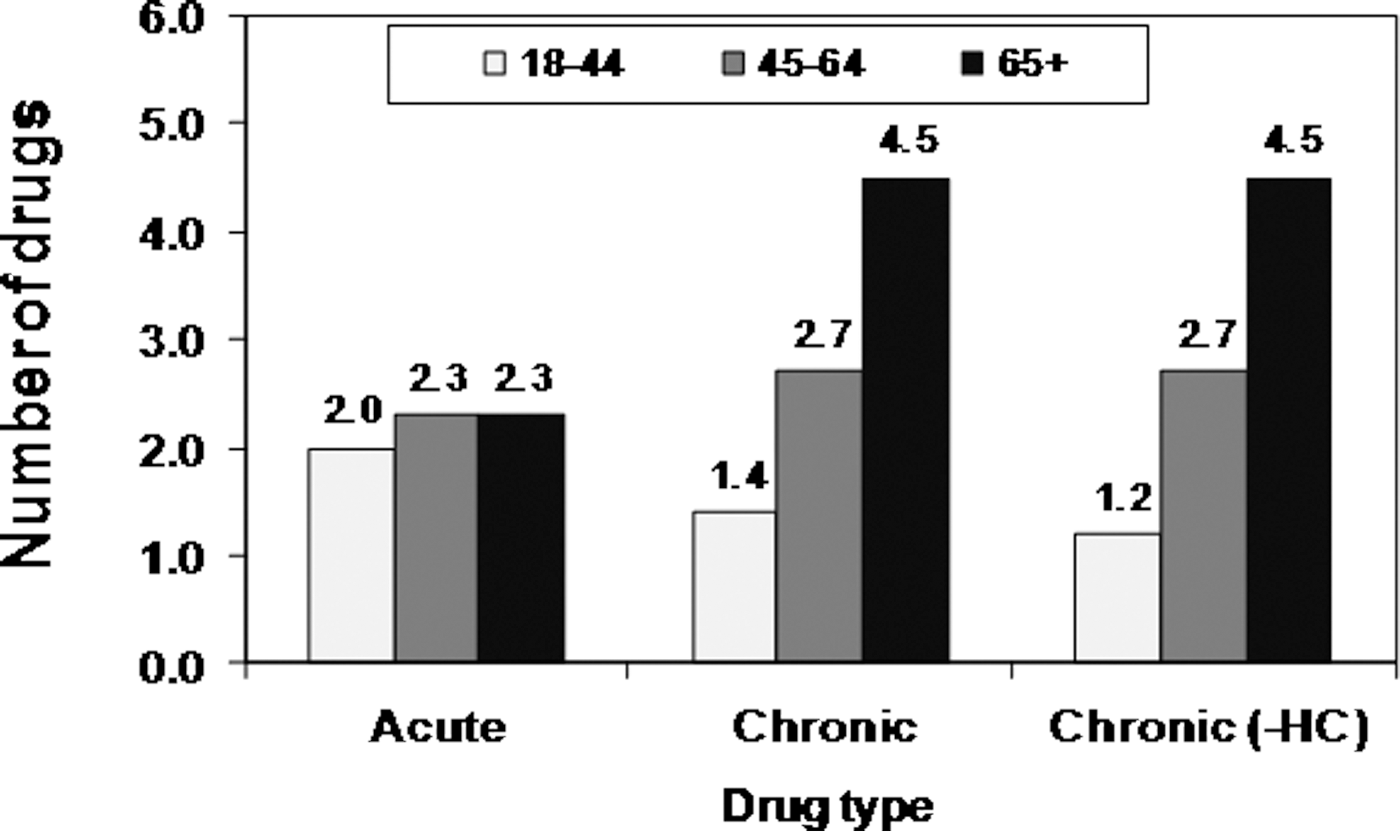
Average number of prescription medications used by women (per member per year), by age group. For chronic drugs, utilization is shown with and without hormonal contraceptives (HC).
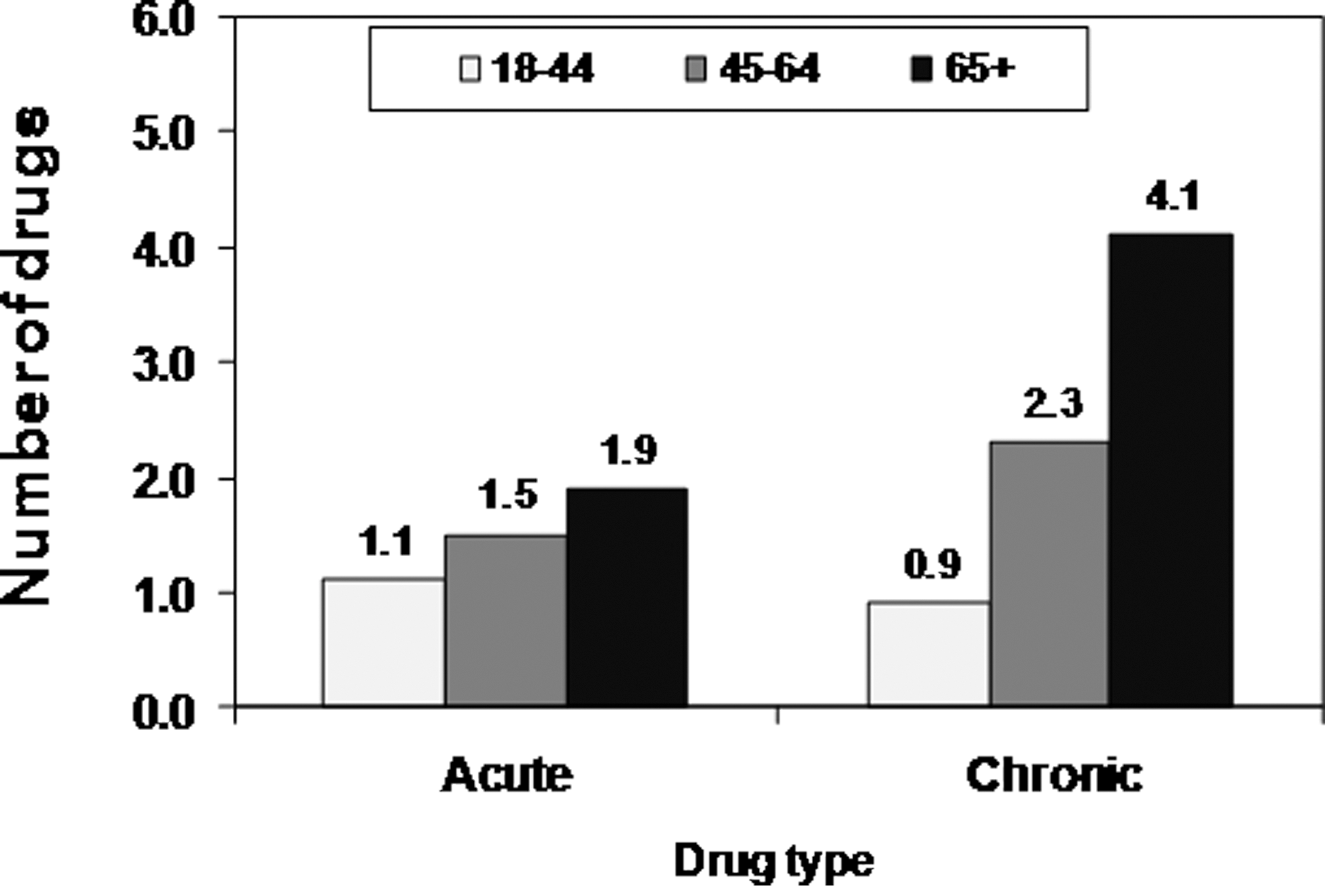
Average number of prescription medications used by men (per member per year), by age group.
Drug utilization and cost: per-patient analysis
Among adults who used medications, female patients filled prescriptions for an average of 7.4 distinct drugs during the analysis year, compared with an average of 6.2 drugs per year for male patients (p<0.001) (Table 3). Annual out-of-pocket costs for prescription drugs were higher on average for female patients than for male patients (Fig. 5), but plan costs and total costs were higher on average for male patients (Table 4). Female patients paid higher average costs for acute drugs, consistent with their higher intensity of use. Male patients paid higher average costs for chronic medications, in spite of their lower average intensity of use.
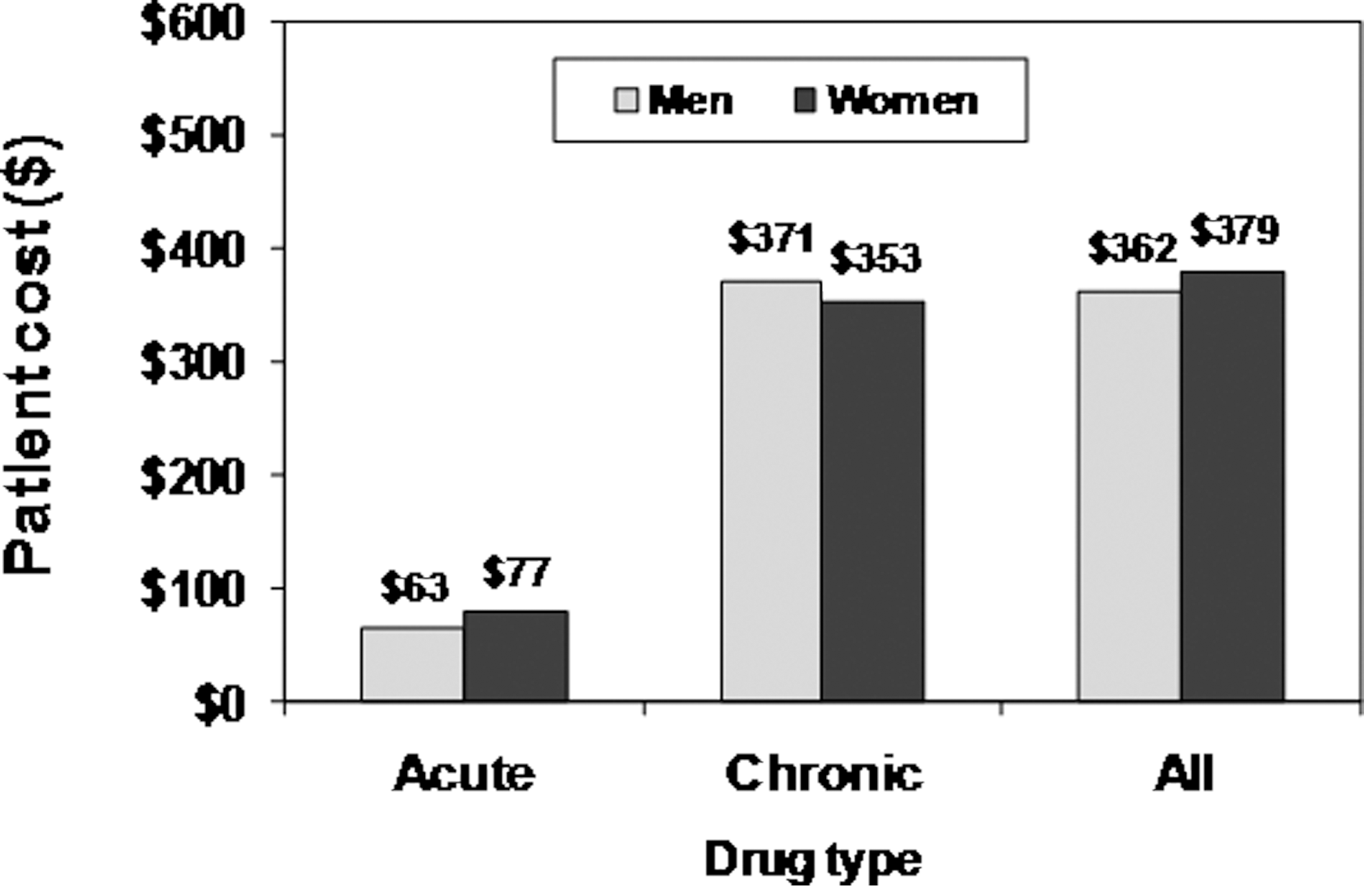
Average annual out-of-pocket costs (US$) for prescription medications (per patient).
“Patients” are insured adults who used one or more medications during the analysis year (2010). Drug utilization is the number of distinct drugs dispensed per patient during the analysis year. All pairwise differences between utilization rates for women and men are statistically significant (p<0.001). Sample sizes are reported in Table 1.
“Patients” are insured adults who used one or more medications during the analysis year (2010). Costs are the mean aggregate costs per patient for all prescriptions filled during the year. Costs are reported in U.S. dollars and are rounded to the nearest dollar; some totals may vary due to rounding. All pairwise differences between women and men are statistically significant (p<0.001).
Medication adherence
Female patients were consistently less likely to be adherent with their diabetes and cardiovascular medications, compared with male patients (Table 5). This difference was observed for oral diabetes medications, cholesterol medications, blood pressure medications, and antiplatelet medications. For example, for oral diabetes medications, 64.6% of female patients were adherent, compared with 67.5% of male patients. In the United States, where an estimated 12.6 million adult women have diabetes, 20 this could equate to more than 4.5 million women who may not reach treatment goals, assuming a similar level of adherence across all forms of medical management.
Medication adherence is the percentage of patients who were adherent (defined as MPR≥80%). Treatment alignment is the percentage of patients who received the medication or monitoring. recommended by treatment guidelines for the condition. All pairwise differences between women and men are statistically significant (p<0.0001).
ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CVD, cardiovascular disease; LDL-C, low-density lipoprotein cholesterol; MPR, medication possession ratio.
Guideline-based prescribing
Women were consistently less likely to receive the medications recommended for most patients by clinical guidelines for patients with diabetes and cardiovascular conditions (Table 5). For example, women were less likely than men to be prescribed a beta blocker following a myocardial infarction (63.4% of women vs. 69.3% of men), and diabetic women were less likely than men to be prescribed one of the recommended classes of antihypertensive drugs as part of their treatment. The most striking difference was for adults with a history of coronary artery disease, where we found that women were far less likely than men to be prescribed a cholesterol-lowering medication (59.0% of women vs. 71.5% of men).
For patients with diabetes, significant disparities were also observed in treatment monitoring (Table 5). Women with diabetes were less likely to have the recommended hemoglobin A1C testing or low-density lipoprotein cholesterol (LDL-C) testing versus men with diabetes. Similarly, among patients using insulin, women were less likely than men to self-monitor their blood glucose levels, as measured by utilization of glucose monitoring test strips. Even without adjustment or matching by disease severity, these lower rates of disease monitoring by women across the board are important to note, as it seems contrary to popularly held notions that women take better care of their health than men do.
Discussion
In this study of almost 30 million insured adults in the United States, we found that women were prescribed more medications than men, they were less adherent in taking their medications, and they were less likely to receive the medications recommended for most patients by national and professional clinical guidelines for diabetes and cardiovascular disease. The analysis evaluated current patterns in medication prescribing and utilization, using sex as the primary independent variable. Future cross-sectional studies will be needed to evaluate other possible covariates of medication use and prescribing, and longitudinal studies will be helpful in evaluating causality.
Drug utilization
There are several possible contributors to the observed sex differences in the level of medication use, including differences in patient behavior and differences in physician prescribing. The higher prevalence and intensity observed for women could be due in part to a higher likelihood that women seek treatment for their symptoms and medical conditions, leading to more treatment visits and more prescriptions. Women tend to seek out preventive care and gender-specific care more frequently than men, 21,22 and some studies have reported higher rates for women seeking out treatment for medical conditions. 23 However, in spite of the higher level of gender-specific care, a woman's reproductive potential does not appear to ensure ideal medication prescribing or health behavior. 24 Our findings suggest that disparities in treatment-seeking may be more prominent for acute conditions—younger men are far less likely than younger women to use acute medications, while prescription rates for chronic medications are more similar for men and women.
Another behavioral variable that could affect sex-based differences in medication use is the degree to which women and men fill the prescriptions they receive from their doctors. Pharmacy claims data reflect only the prescriptions that have been filled and dispensed, not every medication prescribed. An evaluation of differences in prescription fulfillment rates would shed light on the degree to which they may contribute to the sex-based differences observed in this study.
Sex differences in medication use could also be due to differences in physician behavior, including gender biases in what treatment is viewed as appropriate for a given patient. In the current environment, treatment protocols often derive from clinical trials with samples that were dominated by male participants and that failed to distinguish efficacy and adverse events by sex. 6 As a result, treatment choices may be less optimal for women, 7 yielding more frequent side effects that may require additional medication management, 25 or yielding suboptimal outcomes that may lead physicians to engage in more trial and error with different medications.
In some cases, different levels of medication use could also reflect sex differences in disease presentation or severity, or differences in the underlying prevalence of disease. 26 However, in aggregate, the greater use of medications by women should not be taken to imply that their overall health is worse than that of men. As noted above, the differences in medication use could be a sign of being more proactive in seeking healthcare, or a reflection of how women are diagnosed and treated by physicians. This study was not designed to evaluate the relative contribution of these variables to sex differences in medication use; a systematic assessment of these variables would be a fruitful area for future research.
Medication adherence
Improving medication adherence has been shown to decrease total healthcare costs and reduce the use of medical services for cardiovascular disease and diabetes in adult patients. 27 –30 In this study, approximately 60% to 80% of adults were adherent with their medications for these conditions, and average adherence levels (average MPR, not reported here) were even lower. We also found that women were consistently less likely than men to be adherent with their diabetes and cardiovascular medications. This is a surprising finding, given that women tend to be more proactive in obtaining preventive care and treatment for medical conditions.
Lower adherence rates for women have been reported in other studies, 12 and the reason for these differences remains a source of speculation. Adherence can be a challenge for people with large, complex medication regimens, 31 and this may be one factor contributing to reduced adherence for women, whom we found to be more likely to take multiple medications. Higher out-of-pocket costs for medications can also be a deterrent to maintaining adherence. 11,32 However, the differences in out-of-pocket costs for male and female patients in our study were relatively small (Table 4), and out-of-pocket costs for chronic medications were lower on average for women, so it is unlikely that relative cost was the primary determinant of the adherence differences we observed. It is also possible that female patients experience more side effects from their medications. 25,33 –36 Unpleasant side effects are a common reason for discontinuing medications, so higher rates of side effects in female patients could contribute to lower rates of adherence. Women may also face different expectations and priorities that affect the attention they pay to maintaining their own health. Some women may feel a primary responsibility to care for others in the household, and they may neglect caring for themselves in the process. 37
Treatment alignment with guidelines
Without exception, for each measure of medication treatment for diabetes and cardiovascular conditions, our data demonstrate that women were less likely to receive the treatment recommended by national and professional clinical guidelines. Women were less likely to receive the antihypertensive and cholesterol-lowering medications recommended by clinical guidelines for patients with diabetes, and they were also less likely to receive the recommended medications for coronary artery disease, myocardial infarction, and heart failure. For each clinical metric, the medications recommended by clinical guidelines were not prescribed equally to women and men with the same general condition as defined by their drug therapy or medical history. The reasons for this disparity are unclear. There may be differences in the clinical circumstances of individual patients (not discernible in medical claims data) that would support differences in treatment, there may be gender biases in how physicians apply clinical guidelines to women and men, or there may be gender differences in the likelihood of women and men filling prescriptions they have received.
We also observed consistent sex differences in treatment monitoring rates for patients who use diabetes medications. Female patients were less likely to have routine laboratory tests for LDL-C and A1C levels, and they were less likely to do ongoing monitoring of their blood glucose levels. These differences may indicate a lower level of self-care behavior for female patients, compared with male patients, at least in the case of self-monitoring of blood glucose. Routine lab testing can require initiative both by the patient and by the physician, so differences in those measures might reflect self-care behavior, treatment bias, or other variables.
In our analysis of treatment alignment with national and professional clinical guidelines, we assumed that the treatments we evaluated would be equally appropriate for women and men. Our findings showed consistently lower treatment alignment for female patients, which may reflect a larger systems-based problem that could challenge the assumption that equal application is clinically appropriate. Many of the guidelines for medication treatment available today have been based on research trials that lack the specificity to identify and adjust for sex-based differences. Many study populations have been biased toward male subjects, 38 especially in early phase research, and in many clinical trials the efficacy results and adverse event rates have not been differentiated by sex. The paucity of information on differences by sex prevents the development of evidence-based guidelines incorporating these differences. In future research, it would be informative to evaluate the impacts of implementing clinical guidelines where gender-neutral application is likely to be inappropriate.
As advances are made in understanding sex-based differences in disease progression and medication response, it is becoming clear that these differences need to be evaluated from the earliest stages of drug development through the post-marketing analysis of treatment response. This study offers perhaps the largest review to date of how unidentified variables within an insured population may be putting women at a disadvantage. Further reporting of such differences will provide the basis for more informed clinical guideline development, supporting treatment approaches that are more tailored to a patient's sex and other important gender-specific characteristics.
Study limitations
The study is based on a large, representative sample of adults with pharmacy and medical benefits, so the results are likely to have strong external validity for treatment patterns in insured individuals in the United States. However, the findings may not generalize to uninsured populations, where utilization rates, out-of-pocket costs, or treatment patterns may differ from those observed here. As in any analysis based on pharmacy claims, the findings are based on prescription medications that are dispensed under a patient's benefit plan, and they do not include other prescription or over-the-counter drugs that patients may have used during the study period. Prescribing rates may be underestimated to the extent that patients fill prescriptions through other plans, pay the full cost without using insurance (e.g., generic drug discount programs), use complimentary samples, receive medications in a hospital setting, or fail to fill a prescription at the outset. Sex differences in any of these factors could contribute to measured differences in drug utilization or treatment rates.
Pharmacy and medical claims data are a powerful starting point for large, population-based analyses of sex differences in medication use, but the interpretation of these differences is ultimately limited by the data elements available. Although claims data generally include demographic elements such as sex, age, and geographic region, they do not generally include sociodemographic variables (such as income and education) that may also be associated with patient behavior and physician prescribing. Also, claims data generally do not include specific information on disease severity or other clinical measures that may play an important role in a physician's treatment decisions. An observational study of this type can identify broad sex-based differences in medication use, but an evaluation of the contributions of sociodemographic and clinical variables to these differences will require more targeted analysis in separate studies.
Conclusions
In this large, national observational study of adults with prescription drug benefits, we found that women tend to be prescribed more medications than men, but they are less adherent in taking medications for chronic conditions (such as diabetes and cardiovascular disease), and they are less likely to receive the medication treatment recommended by current evidence-based guidelines. Our goal is to raise awareness of the notable differences observed between men and women in medication prescribing and use. To reduce the associated risks for suboptimal care, it is critical to consider the effects of biological sex and gender traits on the patient's response to medications. Research, regulatory science, study publication, guideline development, and evidence-based prescribing must continue to evolve based on advances in personalized medicine, coupled with trends noted in large observational studies such as this. Ultimately, all healthcare professionals will need to incorporate the treatment implications of sex and gender differences into their prescribing decisions for both women and men.
Footnotes
Acknowledgments
The authors would like to thank the Society for Women's Health Research (SWHR) for their support and encouragement during the development of this study. One of the authors, Marie Manteuffel, was employed by SWHR during the design and analysis phase. We would also like to thank Merri Pendergrass, MD, PhD, for her assistance in reviewing the manuscript, and Shannon E. Denison, MA, for her assistance in the early design concept.
Disclosure Statement
No competing financial interests exist.