
Abstract
Background:
Hypertensive disorders of pregnancy (HDP) are leading causes of morbidity and mortality and have been rising in incidence. Little is known about the effects of worker classifications on HDP. This large-scale study examines associations between occupational classifications and HDP.
Methods:
We examined 385,537 Texas Electronic Registrar Birth Registration 2005 birth certificates. Maternal occupations were coded using the Standard Occupational Classification (SOC). Crude and adjusted risks for HDP among working women within occupational groupings were analyzed and compared with risks of nonemployed women.
Results:
The risk of developing HDP varies across SOC occupational classifications. After controlling for known confounders, women employed in business, management, and the legal and social services, teaching, counseling, and healthcare professions are at higher risk for developing HDP than women employed in support industries, such as food preparation, housekeeping, cosmetic and personal care services, or nonemployed women. Women employed in computer, engineering, architectural, and scientific occupations also carry greater risks, although these increased risks do not affect women of normal weight.
Conclusions:
Worker classification is an independent risk factor for HDP. Additional work must be done to examine the complex interactions among individual maternal genetics, biology, and physical and mental abilities and how they affect adverse health outcomes. Examining job stressors may shed light on these occupational variations and their potential HDP associations. Strategies to mitigate job stressors in the workplace should be considered.
Introduction
Definitions and incidence
Hypertensive disorders of pregnancy (HDP) are the second leading cause of maternal mortality 1 and are worldwide leading causes of immediate and long-term maternal and fetal morbidity and early mortality. 2 –6 Previous studies have determined that risks for developing HDP increase with nulliparity, advanced maternal age, high prepregnancy body mass index (BMI), and black race. 7 –9 However, few large-scale systematic studies have been done to examine possible associations between HDP and employment classifications. This study, which is based on data derived from the Texas Electronic Registrar Birth Registration birth certificates for the year 2005, addresses how the risk for developing HDP is affected by ocupational classifications.
HDP include preeclampsia, eclampsia, chronic hypertension, and gestational hypertension. Preeclampsia is diagnosed when both hypertension ≥140/90 mm Hg and proteinuria ≥300 mg in a 24-hour urine collection develop after 20 weeks of pregnancy. Eclampsia occurs when seizures develop secondary to severe preeclampsia and multiorgan dysfunction. Preeclampsia and eclampsia can be life threatening to the mother and the fetus, particularly when they manifest before the 37th week of pregnancy, when the fetus is considered full-term. Chronic hypertension can be equally ominous because it refers to women who have been diagnosed with hypertension before the 20th week of pregnancy and can lead to superimposed preeclampsia if the pregnant woman develops proteinuria during her pregnancy. Gestational hypertension is the mildest form of HDP and is characterized when hypertension develops ≥20 weeks without proteinuria. 10
According to U.S. hospital discharge data, in 2003–2004, the crude incidence rate of HDP was about 61 cases per 1000 deliveries, a rate substantially higher than the 35 cases per 1000 deliveries that existed <20 years earlier. Preeclampsia/chronic hypertension and gestational hypertension each, respectively, accounts for about one half of HDP, with <1% of all cases progressing to eclampsia. 11 The increase in HDP is largely a result of the increasing comorbidities of obesity, chronic hypertension, and diabetes. 12
Three studies with sample sizes <1000 women found higher hypertension levels among women who were employed than nonemployed. 13 –15 The published literature also suggests that among women in the workforce, those who report that their jobs carry high psychologic demands coupled with low decision latitude, who report low job satisfaction, who express concerns about job safety and security, and who assert that there is an imbalance between job effort and reward appear to be at higher risk for HDP than other workers. 16 –22 Most of these published studies either focus more narrowly on specific occupational groupings or are based on small sample questionnaire data that cannot be controlled for known confounders. Our study, which makes use of the large sample size available from the 2005 Texas birth certificate data, has allowed us to overcome or minimize many of these limitations and to investigate specific occupational variations that have not been previously evaluated.
Materials and Methods
The data used for this project came from the 2005 Texas Electronic Registrar Birth Registration, a register that contains 385,537 Certificates of Birth of all reported births in the state of Texas for the year 2005. The Texas Certificate of Birth contains data on >150 variables that are organized on the Certificate of Birth into 65 item areas.
According to Texas law, a Certificate of Birth must be filed within 5 days of the date of birth for every live birth in the state. A birth that occurs at a licensed institution is registered in the Texas Electronic Registrar by the attending physician or midwife, the hospital administrator, the birthing center administrator, or a designee of the appropriate administrator. The person trained for registering the birth at a licensed institution must obtain the information needed for completing the birth certificate from medical records, the mother's physician, the infant's physician, and worksheets that contain information supplied by the mother or, if necessary, by other family. This self-reported information is filled out by the mother or by a hospital employee who interviews the mother and fills in the information for her. A “Guide to Completing the Items on the Texas Certificate of Birth” instructs the hospital staff where in the medical record the information for each item can be found, although these guidelines acknowledge that the specific available records “differ somewhat from facility to facility.” When the birth occurs outside a licensed institution, the birth must be registered by the certified healthcare giver or, if no certified healthcare provider is present, by the father or mother of the child or the owner/householder of the premises where the birth occurred. In this case, documentation is required from the parent before a birth certificate may be filed.
The 65-item dataset of the Texas Certificate of Birth includes previous and concurrent obstetric history information, prepregnancy height and weight data, pregnancy health outcomes for both mother and child derived from medical records, and self-reported data on maternal and paternal demographic characteristics, including questions on the mother's occupation, specifically during the most recent 2 years, and on the type of business or industry related to this occupation. This is the first study to analyze the associations between the self-reported occupational data and the medical records-based pregnancy outcomes in the Texas Electronic Registrar Birth Registration.
In preparing the data for analysis, data were loaded from the 2005 Texas Electronic Registrar Birth Registration into IBM SPSS Statistics 20 software, where it was cleaned, codified, and transformed into the exposure (employment categories) and primary outcome (HDP) variables. Prepregnancy and delivery BMI data, as well as gestational weight gain information, were computed for the cases with complete height and weight data. The maternal occupation data were then coded using the Standard Occupational Classification (SOC) system, which classifies workers according to similar job duties into 23 major and 97 minor groups. 23 Cases with the occupation listed as Unknown (n=4332) and cases with missing occupational data (n=5743) were grouped into a generic category, Other occupations, a grouping that included occupations not referenced in the SOC system, occupations with nondecipherable spellings, and occupations listed only as Self-employed. Cases with the occupation listed as Homemaker or Housewife (or spelling variations of these words) were grouped with cases with the occupation listed as None to form the reference variable Homemaker. Because self-reported responses of Unemployed to the occupation question could signify the active intent of the mother to secure nonhousehold employment, these cases were not grouped with Homemakers but were analyzed as a separate category. Similarly, cases with the occupation listed as Student were analyzed as a distinct category.
SOC categories with small sample sizes were conflated into broader composite categories of occupations with similar characteristics, thus stratifying the women into the following major occupational categories: Homemakers, Students/unemployed, Farming & ranching, Support services, Skilled laborers, Scientists & engineers, All other jobs, Sales, Military & protective services, Educators, Business & management, Healthcare, and Legal & social services. Cases were classified as HDP if any of the following boxes on the birth certificate were checked: chronic hypertension, gestational hypertension, preeclampsia, or eclampsia.
Univariate analyses examined the frequency distributions of maternal characteristics that could be extracted from the Register. Included in these breakdowns were the population frequencies of biologic factors known to affect HDP (i.e., parity, gestational plurality, maternal age, race), and physiologic and socioeconomic factors (i.e., prepregnancy BMI, gestational weight gain, smoking history, previous preterm delivery history, in vitro fertilization (IVF) conception, marital status, maternal and paternal education, Women, Infants, and Children [WIC] recipient, payment type) that might be potential confounders on HDP (Table 1).
BMI, body mass index; WIC, Women, Infants, and Children.
One-way analysis of variance (ANOVA) procedures determined associations with 95% confidence intervals (CI) between the exposure variables and HDP, and graphs illustrating these variations were generated for subsets of the population. All tests were two-tailed, with p≤0.05 considered significant. Because equal group sample sizes and homogeneity of variance could not be assumed, in the analysis of subpopulations, the Games-Howell test was used to determine significance for multiple comparisons. Multivariable logistic regression was used to evaluate the association between the exposure variables and HDP. Two sets of analyses were conducted: a crude model and an adjusted model. In the crude model, occupational classification was treated as the only predictor of occurrence of HDP. In the adjusted model, adjustments controlled for the following potential confounders ascertainable from the birth certificate data: race, plurality, parity, maternal age, paternal age, parental age differences, prepregnancy maternal BMI, gestational weight gain, IVF conception, smoking history, preterm delivery history, marital status, maternal education, paternal education, WIC recipient, Medicaid recipient, and private insurance payment. Likelihood ratio was used as the entry and removal test for stepwise regression, with entry and removal probability set at 0.05 and 0.1, respectively. Covariates were treated like factors for the purposes of determining entry and removal hierarchical constraints. The Institutional Review Board at the University of Texas Health Care Center at Tyler granted administrative approval for this study as exempt research.
Results
Texas is a racially diverse state, with 49.6% of all births in 2005 to Hispanic women, 35.7% of births to white women, 11.2 % of births to black women, and 3.3% of births to Asian women. Of the subjects, 41% were on public Medicaid insurance, and 36% had private health insurance. Over 51% received WIC support during their pregnancy. The prepregnancy BMI of Texas mothers giving birth in 2005 was 5% underweight, 51% normal weight, 25% overweight, and 20% obese. The 20% Texas obesity rate among pregnant women was identical to the national average. 24 During pregnancy, 24% of Texas women gained >40 pounds, which is a slightly higher percentage than the 20% of pregnant women nationwide who gain in excess of 40 pounds. 25
The overall 5.8% HDP prevalence among Texas mothers was similar to the 6.1% national prevalence rate that was reported from 2003–2004 U.S. hospital discharge data. As expected, prevalence rates were significantly higher for multigestational and nulliparous pregnancies, for black and white women as opposed to Asian women, for women of advanced maternal age, for women with high prepregnancy BMI levels, and for women with gestational weight gain <20 pounds or >40 pounds. Measurements of socioeconomic status (SES) (i.e., marital status, maternal education, WIC recipient status, and payment source) had modest or no impact on HDP prevalence (Table 2).
The adjusted odds ratio (aOR) for each subpopulation is adjusted for the 11 risk categories outside the risk grouping of the subpopulation.
Significant differences at p≤0.05.
Nonsignificant differences.
The multivariate analyses of Texas birth registration data also demonstrated a strong linear relationship between occupational classification and HDP (Table 3). HDP prevalence among homemakers and nonhomemakers was 5.03% and 6.67%, respectively, indicating that employed women had a crude increased risk of about 33% above homemakers. The risk remained significantly higher for nonhomemakers when controlled for the known and potential confounders.
Adjusted for race, plurality, parity, maternal age, paternal age, BMI, gestational weight gain, smoking, preterm history, IVF, WIC, Medicaid, marital status, education, insurance.
Significant differences from homemakers at p≤0.05.
Nonsignificant differences.
Employment type also affected HDP risk (Fig. 1). The crude prevalence rate of HDP was higher for nonhomemakers in 10 of the 12 occupational categories examined and was statistically equivalent to the risk for homemakers in two categories. There were no occupational groupings with lower HDP risks than homemakers. The higher risks remained signifant in 6 categories after adjusting for confounders. Specifically, women employed in service industries, such as food preparation, housekeeping, cosmetic and personal care services, as well as women employed in agriculture, had relatively low HDP risks that were approximately equivalent to the HDP risks of homemakers. Meanwhile, women attending school or seeking employment; skilled laborers in the production, construction, or repair industries; women in the military or in the protective services; women in the sales force; and women employed as computer specialists, scientists, architects, and engineers were at modestly higher risk (15%–34%) for HDP than homemakers, although in each of these areas except the Student/unemployed category and women in the sales force, the increased risks associated with employment status disappeared when controlled for all the biologic, phsiologic, familial, and socioeconomic confounders. In contrast, women in business and management and women in the teaching, healthcare, and legal and social services professions were at substantially higher risks (48%–63%) than homemakers. These risks remained significantly higher than homemakers when controlled for the known and potential confounders (Table 3).

Hypertensive disorders of pregnancy (HDP) among homemakers and other groups of employed women. CI, confidence interval.
Post hoc analysis of subpopulations of working women exposed subtle differences in the effect of occupational classifications on HDP. These differences carry important clinical implications. For example, the greater HDP risks associated with women working in computer, engineering, architectural, and scientific occupations affected only overweight and obese women, not women with normal or underweight prepregnancy BMIs (Fig. 2). Also of clinical significance are the variations in the effects of employment classifications on HDP among women in various predelivery risk categories. In most occupational categories, especially in those categories of professional women with likely high job strain, the increased HDP risks associated with employment were substantially higher among women in higher predelivery at-risk populations (i.e., overweight, gestational weight gain ≥40 pounds, black race) than in women with lower predelivery risks (normal weight, gestational weight gain <40 pounds, nonblack race). In sum, women in high predelivery risk categories, especially in weight-related risk groupings, were at even higher risk for HDP if they were employed in high at-risk occupations than other women in similar predelivery risk groups who were not employed in these higher at-risk occupations. Employment classification in high at-risk (and arguably high job strain) occupations also increased HDP risk among lower predelivery risk populations, such as normal weight women who gained <40 pounds during pregnancy, although the slope of the increased risk for these women was less severe (Figs. 3 and 4).
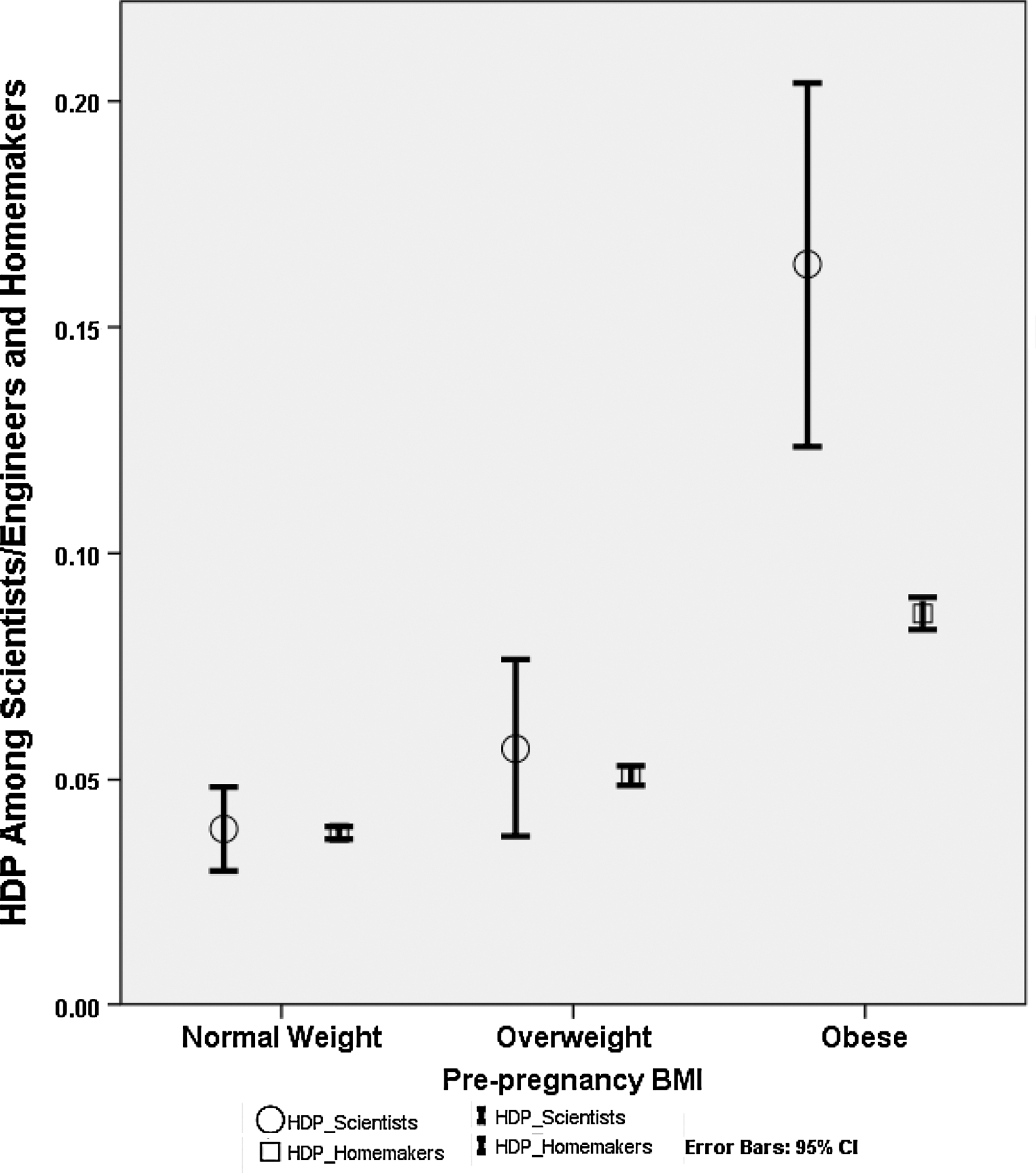
HDP among scientists/engineers, and homemakers by prepregnancy body mass index (BMI) Classification.
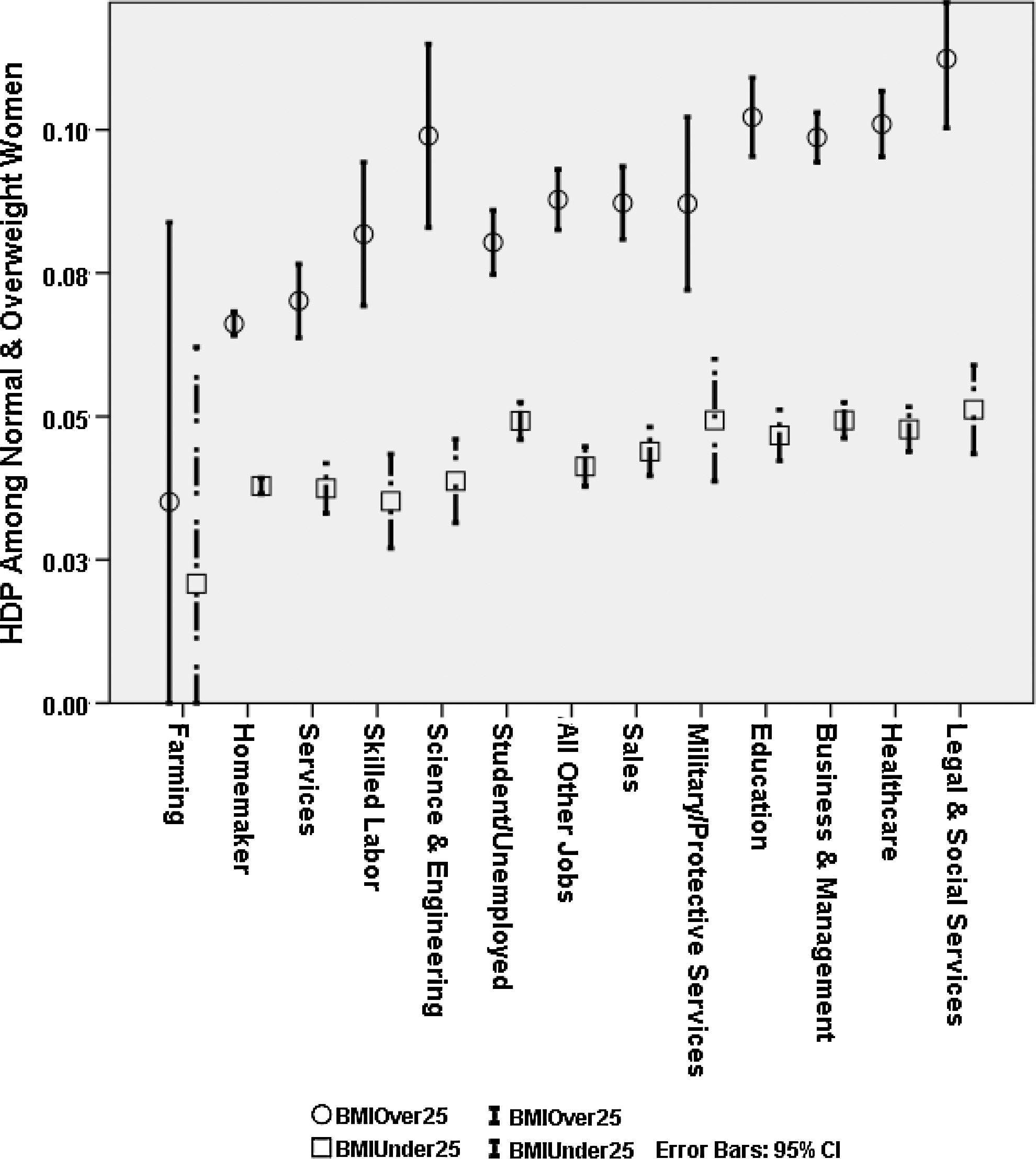
HDP among prepregnant normal and overweight women.

HDP among women with weight gain <40 and ≥40 pounds.
Discussion
Work stressors and HDP
Because our data came from a large, occupationally diverse cohort with robust medical and demographic histories, we have been able to control, to a greater degree than previous studies, for multiple known biologic and sociologic risk factors for HDP and to test to see if nonrandom associations between employment type and HDP remained. The results of this analysis identified the presence of nonrandom clusters of high HDP risk populations. After controlling for confounders, employment classifications shed light on HDP trends. Professional women employed in sales, business, management, education, healthcare, and the legal and social services professions were identified at higher risk for HDP than women employed as skilled laborers or women working in the services sector. Homemakers not employed outside of the home had even lower HDP risks. The adverse effects of employment in high at-risk occupations were even greater for overweight women, for women with a gestational weight gain of at least 40 pounds, and for overweight women with excessive gestational weight gain, suggesting potentially clinically significant interactions between metabolic risk factors and job-related risks.
The higher risk clusters among employed women, especially among women in the professional classes, and the minimal impact of lower SES on HDP, are surprising, given the multiple studies that associate lower SES with higher health risks. These results, however, are consistent with other studies that associate high prevalence of hypertension, cardiovascular disease (CVD), and HDP with workers exposed to high psychosocial and physical job stressors. 26 –31 At least among this population, the majority of whom received some prenatal care and WIC support, the data suggest that the higher risks associated with professional and business employment exceeded whatever protective benefits may be associated with higher socioeconomic class.
Several plausible physiologic mechanisms have been suggested for the association between job stressors and hypertensive disorders. The body can respond to stress by inducing vagal withdrawal that is accompanied by a decreased parasympathetic response and heart rate variability. 32 Subsequent increased sympathetic activity with increases of the stress hormones norepinephrine and cortisol can lead to increased production of serum proinflammatory cytokines that could alter maternal immune function. 33 One case-control study verified the hypothesis that nulliparous women undergoing job strain had slightly over twice the risk for developing preeclampsia and were a third more likely to develop eclampsia, likely secondary to heightened production of catecholamines leading to the development of HDP. 21 The pregnancy outcomes of Texas women appear to support the hypothesis that employment stressors may contribute to higher rates of cardiovascular disorders.
Study limitations
Trained persons gather data for the Certificates of Birth from hospital records, hospital staff, healthcare professionals, the patient's physician, the patient, and the patient's family. Depending on personnel to record the demographic, personal, occupational, and industrial data means that errors of omission, presumption, and misclassification can occur. In addition, the accuracy of self-reported information can be highly variable, owing to recall bias, miscommunication, and miscalculation. Physician and hospital errors in coding diagnoses and transfer of these diagnoses to the birth certificates can add to discrepancies and misclassifications. In particular, occupational exposures can be complex, heterogeneous, and difficult to define and characterize. Although every effort has been made to follow the guidelines and detailed instructions in using the SOC to classify occupations, and this study has coordinated occupational titles with industry, one recognizes that the misclassification of workers is possible. Furthermore, necessary categorizing of occupations does not allow for individual variations and responses within job classifications. Other factors that can affect exposure outcomes include the timing of exposures during pregnancy that can be key to determining the type and severity of maternal and fetal adverse health effects.
Fortunately, because accurate birth certificate data are needed for state data reporting, the Texas Department of State Health Services (DSHS) attempts to minimize birth certificate data error by using a comprehensive quality control system to validate the certificate entries. The DSHS quality control system includes computer-based edits to verify field entries, data quality and formats, legitimate values, corresponding field agreements, correct calculations, and nonduplicate records. DSHS verification of data may include making phone calls to hospitals, as well as working with the staff in the Vital Statistics and Information Technology Units. DSHS staff also review the birth data using guidelines from the National Center for Health Statistics. Although this quality control system is not error proof, it does help to ensure reliable and representative data.
Another limitation of most occupational studies is the healthy worker effect, a bias that results because workers tend to be better fit both physically and psychologically than the unemployed population. This type of bias potentially produces an underestimation of the association between occupational stress and disease. However, because the occupational classifications in this dataset do not require that the mother worked at the recorded occupation throughout her pregnancy but only that she worked at that occupation within the 2 years previous to data collection, the healthy worker effect for this dataset likely has been attenuated.
Conclusions
Our study provides objective data that occupational category is an independent risk factor for HDP and that it varies across SOC occupational classifications in predictable patterns. As mentioned, these findings are consistent with previous studies that have shown associations with certain job characteristics and HDP. Women employed in sales, business, management, and the legal and social services, teaching, counseling, and healthcare professions were at higher HDP risks than women employed in service industries, such as food preparation, housekeeping, cosmetic and personal care services, or nonemployed homemakers. These patterns remained significant when adjusted for plurality, parity, race, maternal and paternal age, prepregnancy BMI, gestational weight gain, smoking history, previous history of preterm deliveries, and multiple proxies of SES. Women employed in computer, engineering, architectural, and scientific occupations also carried greater HDP risks, although these increased risks did not appear to affect women of normal weight. Women in the military and in the protective services also carried higher HDP risks, although this analysis suggests that these risks may be more influenced by a combination of confounding factors than by employment status itself.
Further study is needed to understand the causes of these associations, but it appears that stressors at work may contribute to increasing one's risk for developing HDP. Future research needs to examine the types of stressors within certain occupations that seem more ominous and may contribute more significantly to higher risks of developing HDP. Considering ways to lower psychosocial stressors among pregnant women in the workplace, in particular, raising psychosocial support and increasing decision latitude while lowering job demands, makes sense, given the high morbidity and mortality associated with HDP. Improving one's coping strategies and responses to stress also may prove to be valuable in lowering HDP risks. In addition, more work must be done to examine the complex interactions among individual maternal genetics, biology, and physical and mental abilities and how these may affect perception of stress and HDP risks. Redesigning jobs and providing support to address these issues could improve productivity and morale of workers and perhaps decrease job strain. These changes might benefit all workers and increase worker efficiency and, thus, be valuable tools that businesses would want to adopt.
Footnotes
Acknowledgments
We thank Gene Willard and Janice Jackson at the Texas Department of State Health Services for the Texas birth certificate data and Edward F. Fitzgerald at the University of Albany, State University of New York, for assistance in locating the data. We also extend thanks to Debra Cherry at the University of Texas Health Science Center at Tyler for her assistance and review of this article.
Disclosure Statement
The authors have nothing to disclose.