
Abstract
Background:
Studies of the relationship between vitamin D and inflammation are equivocal. This may be due to unaccounted confounding. Hormonal contraceptive (HC) use is associated with elevated circulating 25-hydroxyvitamin D [25(OH)D] in Caucasians and African-Americans, but its effects on 25(OH)D in other ethnicities are unclear. HC use is associated with elevated C-reactive protein (CRP), an inflammatory biomarker. Our objectives were to assess the effect of HC use on 25(OH)D across ethnic groups, and to examine the association between HC, 25(OH)D and CRP in an ethnically diverse population of young adults.
Methods
Results:
Across ethnic groups, women HC users (n=280) had higher 25(OH)D and CRP than women HC non-users (n=695) and men (n=428) (p<0.008 and p<0.0001, respectively). Circulating 25(OH)D was positively associated with CRP in the entire population in models not accounting for HC use (β=0.010±0.003; p<0.0001). There was no association when men and women HC non-users were examined separately. Among women HC users, there was no association after accounting for hormone dose. A positive association between 25(OH)D and CRP among individuals above the median 25(OH)D (≥51.9 nmol/L) was not significant after adjustment for HC use. No association was observed among individuals below the median.
Conclusions:
HC use and 25(OH)D were positively associated across ethnic groups. We found no association between 25(OH)D and CRP when HC use was accounted for. HC use confounds the association between 25(OH)D and CRP.
Introduction
There is great interest in the potential preventive and therapeutic effects of vitamin D on numerous chronic diseases, such as type 2 diabetes, cardiovascular disease, various cancers, and autoimmune disorders, such as multiple sclerosis and rheumatoid arthritis. Chronic inflammation, characterized by elevated circulating concentrations of pro-inflammatory cytokines, such as interleukin 6, and hepatic acute phase proteins, such as C-reactive protein (CRP), is a common feature of these diseases. 1 –4
Growing evidence from in vitro and animal studies supports a role for vitamin D in innate immune responses and inflammation. 5,6 However, epidemiological studies and clinical trials have yielded inconsistent results. On the one hand, cross-sectional studies carried out in diverse populations have found an inverse association between circulating concentrations of 25-hydroxyvitamin D (25(OH)D) and CRP. 7,8 Certain intervention trials also found that oral supplementation with vitamin D resulted in increased concentrations of 25(OH)D and decreased concentrations of CRP and other inflammatory markers. 9,10 On the other hand, some other cross-sectional and intervention studies found a null association between 25(OH)D and markers of inflammation, including CRP, 11,12 and one recent study reported a positive association between 25(OH)D and CRP among vitamin D-sufficient adults. 13 Circulating 25(OH)D, the metabolite used clinically to determine vitamin D status, captures both dietary vitamin D intake and endogenous production after exposure to sunlight, 14 while CRP is considered a robust marker of systemic inflammation. 1
The discrepancies between studies have been attributed partially to differences in vitamin D dosage as well as nutritional and disease status of the populations surveyed. However, a number of biological, lifestyle, and demographic factors affect circulating 25(OH)D concentrations, such as skin color, sun exposure behaviors, geographical location, seasonality, genetic variation, and use of certain medications. 14 –18 These and other factors may play a role as confounders in the relationship between vitamin D and inflammatory biomarkers.
A number of studies have reported a positive association between estrogen and 25(OH)D in women who use estrogen-containing hormonal contraceptives (HC) or hormone replacement therapy (HRT). 16,19 –22 However, most studies were conducted in individuals of European or African ancestry, and the effects of these medications on 25(OH)D in other ethnic groups are less well understood. In addition, use of HC and HRT has also been associated with deleterious health outcomes, such as increased risk of cardiovascular disease and cancer, as well as a worsened metabolic profile, thrombosis, and elevated inflammation. 23 –28 A recent study examining the association between HC use and the plasma proteome identified a number of novel pathways that are affected by HC use, suggesting that the effects of HC on disease-associated metabolic pathways may be widespread. 29 Use of these medications may, therefore, confound the association between 25(OH)D and various health outcomes. Indeed, one study from the Women's Health Initiative trial found that HRT modified the effect of calcium and vitamin D supplementation on colorectal cancer, 30 and an analysis of data from a large German cohort showed that HRT use attenuated an inverse association between 25(OH)D and breast cancer. 22 The use of HC in particular has been associated with elevated concentrations of CRP and other inflammatory biomarkers. 23,24,28,31 These effects are apparent after only 3 months of continued HC use, 24 and are thought to result from first-pass hepatic metabolism of estrogen-containing HC, which may affect hepatic production of CRP and other pro-inflammatory acute phase reactants. 31 However, despite these well-known effects on inflammation, no studies have directly investigated whether HC use, which is widespread among premenopausal women worldwide, modifies the association between 25(OH)D and inflammation. Accounting for this potential confounding effect may help explain the unexpected positive association between 25(OH)D and CRP observed in a previous study. 13
The objectives of this study were to assess the effect of HC use on 25(OH)D concentrations across different ethnic groups and to examine the interaction between HC use, 25(OH)D concentrations, and CRP in a large, ethnically diverse population of young adults.
Materials and Methods
Study design and participants
Study participants were from the Toronto Nutrigenomics and Health Study, which is a cross-sectional analysis of individuals aged 20–29 years living in Toronto. Recruitment occurred from the autumn of 2004 to the autumn of 2011. All recruited individuals gave written informed consent, and the protocol was approved by the Ethics Review Board of the University of Toronto. All study participants gave an overnight fasting blood sample and completed a food frequency questionnaire (FFQ), a general health and lifestyle questionnaire, and a physical activity questionnaire. We excluded individuals who were unable to provide a blood sample, as well as pregnant or breastfeeding women. Individuals who were First Nations Canadian, Afro-Caribbean, or of mixed ancestry were excluded from the analyses reported here because of the insufficient sample size.
The individuals included in this study (n=1,403) were non-smoking men (n=428) and women (n=975), free of diabetes, who had available information on 25(OH)D, CRP, HC use among women, and each additional variable considered for analysis at the time that this study was carried out. Participants were classified as Caucasian (n=702), East Asian (n=536), or South Asian (n=165) based on self-reported ancestry, as described previously. 32 Participants were grouped by season based on the date when they provided blood: winter (December, January, February), spring (March, April, May), summer (June, July, August), and autumn (September, October, November).
Anthropometric and physical activity measures
Anthropometric variables, including height, waist circumference, body mass index, and systolic and diastolic blood pressure, were measured with the participant wearing light clothing and no shoes, as previously described. 32 Participants provided information on physical activity by questionnaire, and level of physical activity was expressed as metabolic equivalent task-hours per week, as described previously. 33
Dietary assessment
Dietary intake was assessed using the Toronto-modified Willett questionnaire, which is a 196-item semiquantitative FFQ that includes questions on dietary supplements, such as multivitamins and vitamin D supplements. 32,34,35 Subject responses to the individual foods were converted to daily number of servings for each item. Estimates of intake were based on the United States Department of Agriculture Nutrient Database for Standard Reference. 36 VitaminD intake is reported as international units (IU) per day.
Hormonal contraceptive use
Women reported use of HC by questionnaire. Women participants were grouped into HC users (n=280) or HC non-users (n=695), based on their responses to the questionnaire. HC users were those who reported current use of any type of HC, regardless of delivery method (oral, transdermal, vaginal, injection, etc.). Based on the type of medication used, HC users were further categorized into those taking HCs with <1 mg or ≥1 mg of total hormone (estrogen + progesterone-derived ingredients) per day.
Biochemical and 25(OH)D measurements
Each participant provided a blood sample after a minimum 12-hour overnight fast. Individuals with temporary inflammatory conditions, including recent piercings or tattoos, acupuncture, medical or dental procedures, vaccinations or immunizations, infections, or a fever, gave blood after a 2-week wait. Samples were collected at LifeLabs Medical Laboratory Services (Toronto). High-sensitivity CRP was measured at LifeLabs using a latex-enhanced immunoturbidimetric method with the Siemens Advia® 2400 analyzer (Siemens Healthcare Diagnostics Inc.). Plasma 25(OH)D was measured by high performance liquid chromatography-tandem mass spectrometry at the University Health Network Specialty Lab (Toronto). The concentration of 25(OH)D is reported as the sum of 25-hydroxycholecalciferol (D3) and 25-hydroxyergocalciferol (D2) for each participant.
Statistical analysis
The software SAS (version 9.2; SAS Institute Inc.) was used to perform all statistical analyses. The α error was set at 0.05, and all reported p-values are two-sided. Continuous variables that were not normally distributed were loge- or square root-transformed prior to analysis, unless otherwise indicated. In each case, the p-values from analyses using the transformed values of these variables are reported, but untransformed means, regression coefficients, and measures of spread (standard deviations or standard errors) are reported to facilitate interpretability.
Subject characteristics between men, women HC non-users, and women HC users were compared using chi-square tests for categorical variables and analysis of variance (ANOVA) for continuous variables. We then compared circulating 25(OH)D and CRP concentrations among men, women HC non-users, and women HC users within each ethnic group using analysis of covariance (ANCOVA) adjusted for age, waist circumference, physical activity, and season of recruitment. We also conducted correlation analyses to explore the association between circulating 25(OH)D and total dietary intake of vitamin D in the population as a whole, independently within each ethnic group, and separately among men, women HC non-users, and women HC users within each ethnic group. Correlations were also conducted between 25(OH)D and CRP in the same manner. Where indicated, correlation coefficients were compared between subgroups using the Fisher's z transformation.
We examined the association between 25(OH)D and CRP using linear regression. First, an unadjusted linear regression was conducted with CRP as the outcome variable and 25(OH)D as the predictor variable in the entire population to explore trends in the data. Then, linear regressions adjusted for age, waist circumference, physical activity, ethnicity, and season of blood draw were carried out separately in the population as a whole, among men, women HC non-users, and women HC users. In the analysis of the population as a whole, the model was also adjusted for sex. We then conducted additional linear regressions to examine the association between 25(OH)D and CRP among individuals below and above the median 25(OH)D concentration, in order to determine whether the direction of the association differed between those with a lower or a higher vitamin D status. In these analyses, Model 1 was unadjusted. Model 2 was adjusted for age, sex, waist circumference, physical activity, ethnicity, and season. Model 3 was adjusted for all the covariates included in Model 2, plus HC use among women.
Finally, within women HC users, we examined the association between 25(OH)D and CRP among those taking <1 mg (n=170) versus ≥1 mg (n=63) total hormone per day, to determine whether hormone dose played a role in this relationship. The two hormone dose categories were created based on self-reported type of HC medication, including brand, using information on dose available from the specific manufacturer's website. We excluded subjects (n=47) from this analysis if the type of HC medication they reported made it difficult to ascertain daily hormonal exposure (e.g., receiving HC by injection, since the timing of this mode of delivery ranges from weeks to months depending on the brand; reporting “Other”; or reporting HC use but not reporting a type of medication).We first compared circulating 25(OH)D and CRP concentrations between women HC users taking <1 mg/day versus ≥1 mg/day total hormone using ANCOVA adjusted for age, waist circumference, physical activity, and season. We then conducted linear regressions adjusted for age, waist circumference, physical activity, ethnicity, and season separately among women taking <1 mg/day and ≥1 mg/d total hormone.
Results
Subject characteristics
Subject characteristics are shown in Table 1. We observed differences in HC use across ethnic groups, with a greater percentage of Caucasian women reporting use of HC than East or South Asian women (p<0.0001). Circulating 25(OH)D concentrations were approximately 25 nmol/L higher in women HC users than in men and women HC non-users, despite a similar total vitamin D intake across groups (p<0.0001 and p=0.26, respectively). Women HC users had the highest circulating CRP, whereas women HC non-users had the lowest CRP concentrations (p<0.0001).
Shown are crude means±standard deviations for continuous variables, and n (%) for categorical variables.
p-values from analysis of variance (ANOVA) for continuous variables and chi-square for categorical variables. P-values are from tests using loge- or square root-transformed variables as necessary to improve normality, but untransformed means and standard deviations are shown for ease of interpretation.
Different superscript letters indicate significant differences in specific subject characteristics between men, women HC non-users, and women HC users (p<0.05). The Tukey-Kramer procedure was used to adjust for multiple comparisons between groups within each ANOVA.
BMI, body mass index; CRP, C-reactive protein; HC, Hormonal contraceptive; IU, international units; MET, metabolic equivalent task.
Effect of HC use on 25(OH)D and CRP concentration
We first examined differences in 25(OH)D concentrations between women HC users, women HC non-users, and men across ethnic groups (Fig. 1). Across all ethnic groups, women HC users had significantly higher circulating 25(OH)D than men and women HC non-users after adjusting for age, waist circumference, physical activity, and season of recruitment (p<0.0001 for Caucasians and East Asians, and p=0.0079 for South Asians). Concentrations of 25(OH)D were similar between men and women HC non-users across ethnic groups.
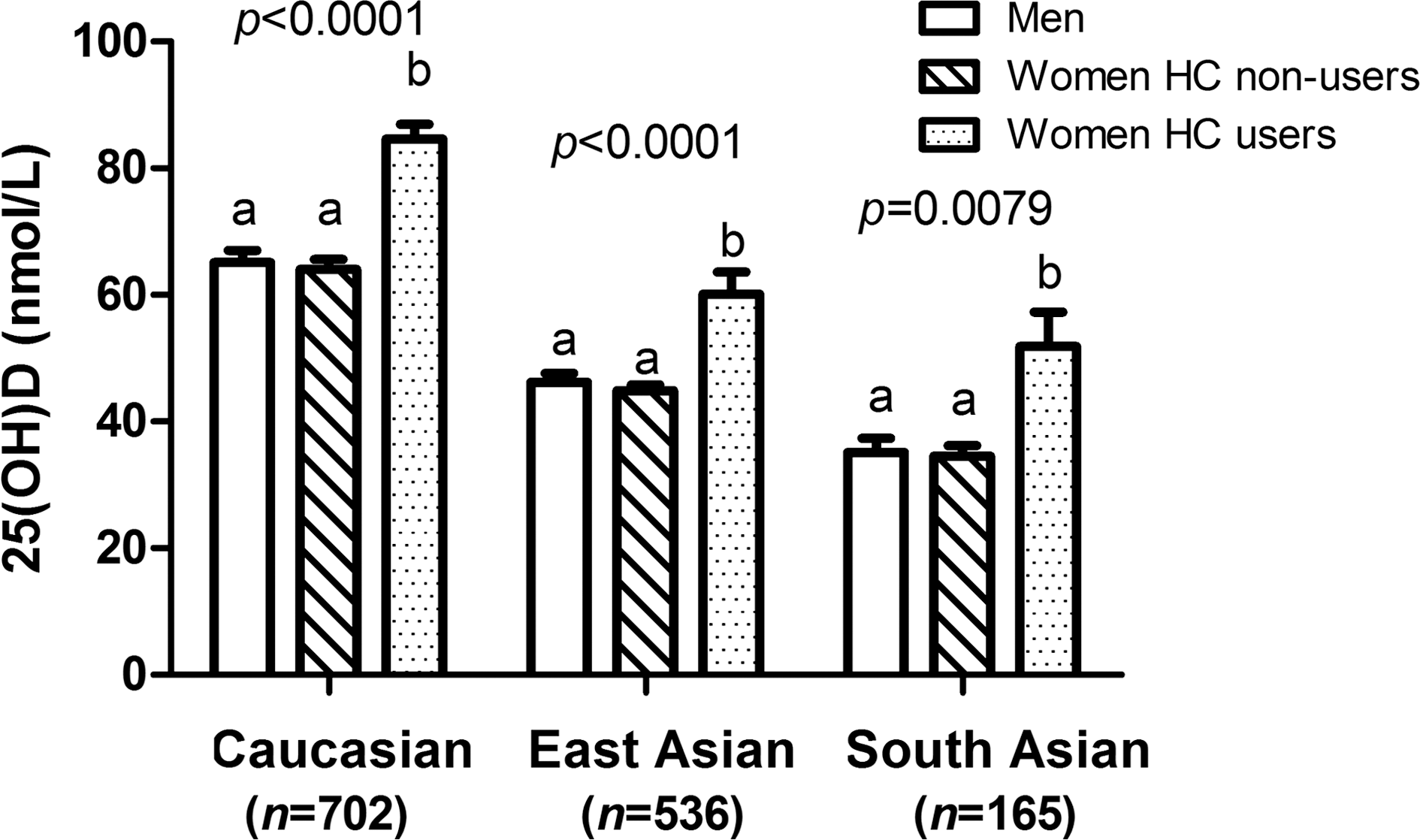
Plasma 25-hydroxyvitamin D [25(OH)D] concentrations among men, women hormonal contraceptive (HC) non-users, and women HC users, by ethnicity. Shown are crude means±standard errors. P-values were obtained with analysis of covariance (ANCOVA). Within each ethnic group, mean 25(OH)D concentrations were compared between men, women HC non-users, and women HC users after adjusting for age, waist circumference, physical activity, and season of recruitment. Plasma 25(OH)D was loge-transformed prior to analysis to improve normality. However, untransformed means and standard errors are shown for ease of interpretation. Within each ethnic group, different superscript letters indicate significant differences between men, women HC non-users, and women HC users (p<0.05). The Tukey-Kramer procedure was used to adjust for multiple comparisons between groups. Across all ethnic groups, women HC users had significantly higher circulating 25(OH)D than men and women HC non-users. Concentrations of 25(OH)D were similar between men and women HC non-users across ethnic groups.
We then examined differences in CRP concentrations among women HC users, women HC non-users, and men across ethnic groups (Fig. 2). After statistical adjustment, women HC users had higher CRP concentrations than men and women HC non-users across ethnic groups (p<0.0001). Among Caucasians and South Asians, men had CRP concentrations that were intermediate between women HC users and non-users. In East Asians, we observed no differences in CRP concentrations between men and women HC non-users.
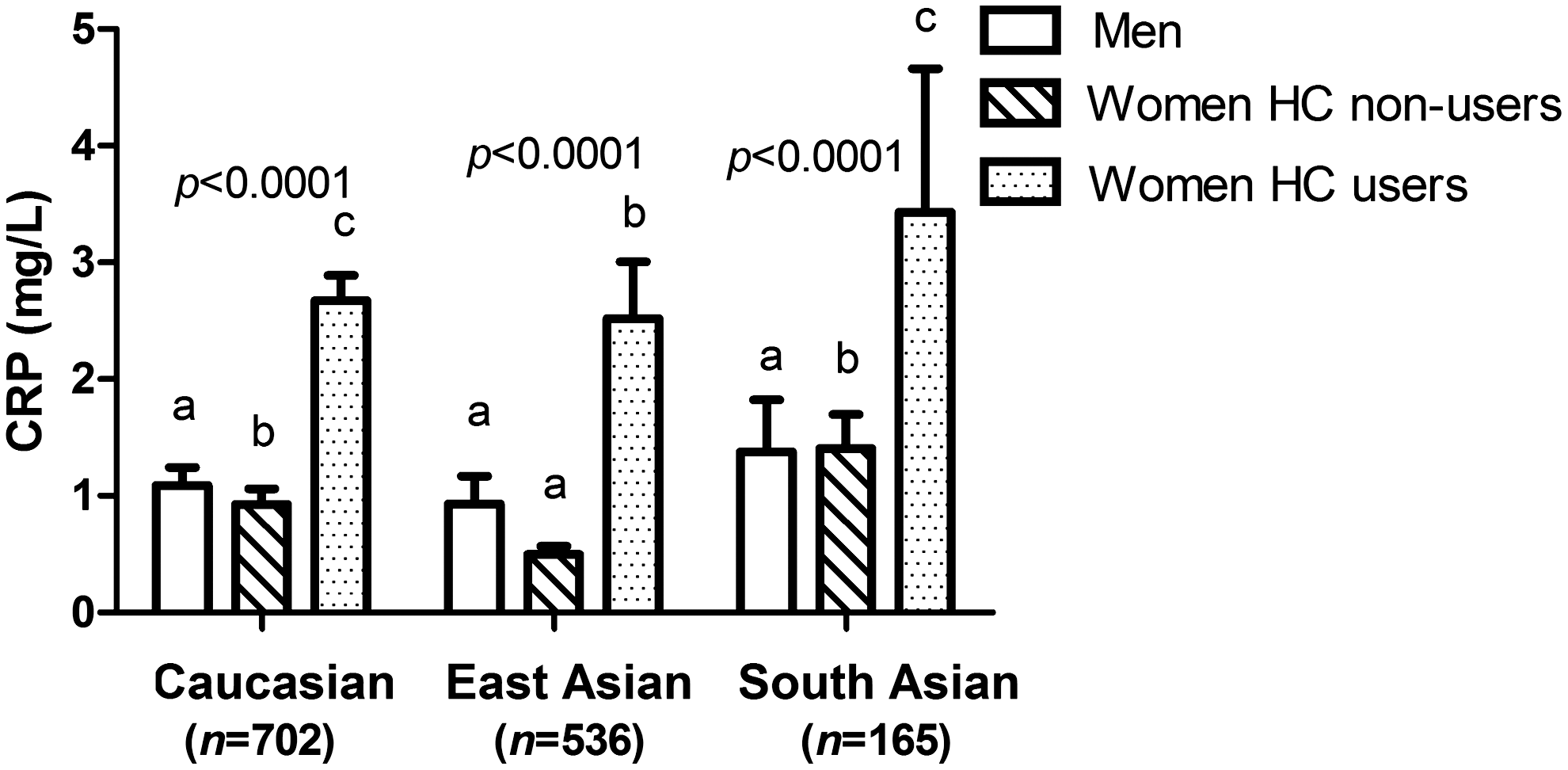
C-reactive protein (CRP) concentrations among men, women hormonal contraceptive (HC) non-users, and women HC users, by ethnicity. Shown are crude means±standard errors. P-values were obtained with ANCOVA. Within each ethnic group, mean CRP concentrations were compared between men, women HC non-users, and women HC users after adjusting for age, waist circumference, physical activity, and season of recruitment. Circulating CRP was loge-transformed prior to analysis to improve normality. However, untransformed means and standard errors are shown for ease of interpretation. Within each ethnic group, different superscript letters indicate significant differences between men, women HC non-users, and women HC users (p<0.05). The Tukey-Kramer procedure was used to adjust for multiple comparisons between groups. Women HC users had higher CRP concentrations than men and women HC non-users across ethnic groups. Among Caucasians and South Asians, men had CRP concentrations that were intermediate between women HC users and non-users. In East Asians, we observed no differences in CRP concentrations between men and women HC non-users.
Correlations between 25(OH)D and dietary vitamin D intake, and between 25(OH)D and CRP
Table 2 shows the results of correlation analyses exploring the relationship between 25(OH)D and total dietary vitamin D intake. Overall, circulating 25(OH)D and dietary vitamin D were more strongly correlated among South Asians than Caucasians and East Asians (Pearson's r=0.55 [p<0.0001], 0.24 [p<0.0001], and 0.27 [p<0.0001], respectively; Fisher's z transformation p<0.0001). Within Caucasians, circulating 25(OH)D and dietary vitamin D appeared to be more strongly correlated among men and women HC non-users than among women HC users (r=0.28 [p<0.0001], 0.26 [p<0.0001], and 0.19 [p<0.006]). However, these correlation coefficients were not significantly different from each other (Fisher's z transformation p=0.15). Within East Asians, circulating 25(OH)D and dietary vitamin D were correlated only among men and women HC non-users, with coefficients of approximately 0.30 (p<0.0001). In South Asians, correlation coefficients between 25(OH)D and dietary vitamin D were different between men, women HC non-users, and women HC users (Fisher's z transformation p=0.03), ranging from 0.48 (p<0.0001) among women HC non-users to nearly 0.70 among women HC users (p=0.0025).
Pearson's (r) correlation coefficients are shown. Within Caucasians, circulating 25-hydroxyvitamin D [25(OH)D] and dietary vitamin D were more strongly correlated among men and women HC non-users than women HC users. Within East Asians, 25(OH)D and dietary vitamin D were correlated among men and women HC non-users only. In South Asians, 25(OH)D and dietary vitamin D more strongly correlated than in the other ethnic groups, and were correlated across men, women HC non-users, and women HC users. In the population as a whole, 25(OH)D and CRP were positively correlated. When examined within each ethnic group, 25(OH)D and CRP were positively correlated among Caucasians and East Asians, but not South Asians. When men, women HC non-users, and women HC users were examined separately, the two metabolites were not significantly correlated in any ethnic group.
Variables were loge- or square root-transformed as needed prior to analysis.
Table 2 also shows the results of correlation analyses between 25(OH)D and CRP. In the population as a whole, 25(OH)D and CRP were positively correlated (r=0.19, p<0.0001). When examined within each ethnic group, 25(OH)D and CRP were positively correlated among Caucasians (r=0.14, p=0.0001) and East Asians (r=0.17, p=0.0001), but not among South Asians. When men, women HC non-users, and women HC users were examined separately, the two metabolites were weakly correlated in East Asian women HC non-users (r=0.13, p=0.0131), and not correlated in any other subgroup.
Effect of HC on the association between 25(OH)D and CRP
The association between 25(OH)D and CRP was first explored using linear regression (Fig. 3). The two metabolites were positively associated in an unadjusted model in the population as a whole (p<0.0001). The positive association was retained in the adjusted model. However, when men, women HC non-users, and women HC users were examined separately, we observed no association between 25(OH)D and CRP among men and women HC non-users. Among women HC users, 25(OH)D and CRP were positively associated in an adjusted model (p=0.002).
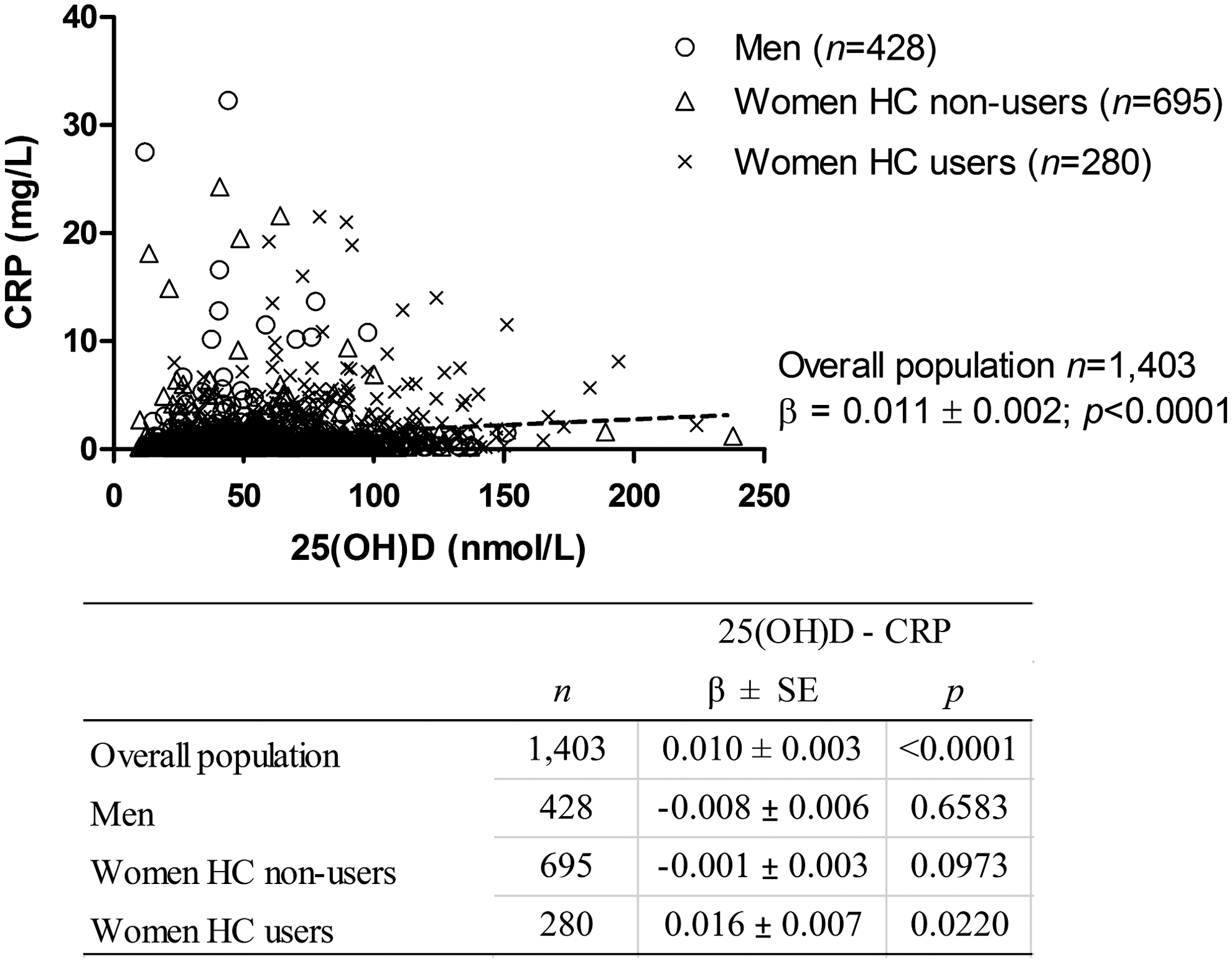
Association between 25(OH)D and CRP. First, unadjusted, untransformed 25(OH)D and CRP values were plotted on a single graph with open circles representing men, open triangles representing women hormonal contraceptive (HC) non-users, and crosses representing women HC users. An unadjusted linear regression was conducted on the untransformed values for the entire population to explore the association between 25(OH)D and CRP (linear regression shown as dotted line). Then, linear regressions adjusted for age, waist circumference, physical activity, ethnicity, and season, using loge-transformed CRP, were carried out separately among men, women HC non-users and women HC users, as well as in the population as a whole (in this case, the model was also adjusted for sex). The table insert shows regression coefficients (β)±standard errors and p-values for these adjusted linear regressions. Untransformed β coefficients and standard errors (SE) are shown for ease of interpretation. In the unadjusted model of the population as a whole, the two metabolites were positively associated. The positive association was retained in an adjusted model. However, when men, women HC non-users, and women HC users were examined separately, we observed no association between 25(OH)D and CRP among men and women HC non-users. Among women HC users, 25(OH)D and CRP were positively associated in an adjusted model.
The population was then divided into two groups: those with 25(OH)D below or above the median (51.9 nmol/L). Linear regressions were conducted separately within each group to examine the association between 25(OH)D and CRP. These results are shown in Table 3. Among those below the median 25(OH)D concentration, we observed no association between 25(OH)D and CRP. In the group above the median, we observed a positive association (p<0.0001) between the two metabolites in both unadjusted and adjusted models (Model 1 and 2, respectively). However, the association was no longer significant after further adjusting for HC use among women (Model 3).
Shown are regression coefficients (β)±standard errors (SE).
p-values from linear regression. CRP was loge-transformed prior to analysis to improve normality. However, untransformed β coefficients and standard errors are shown for ease of interpretation. Model 1 was unadjusted. Model 2 was adjusted for age, sex, waist circumference, physical activity, ethnicity, and season. Model 3 was adjusted for the variables included in Model 2, plus hormonal contraceptive use among women. No association between 25(OH)D and CRP was seen among individuals below the median 25(OH)D concentration. Among individuals above the median, we observed a positive association between 25(OH)D and CRP in Models 1 and 2, but the association was no longer significant after adjusting for hormonal contraceptive use among women (Model 3).
Effect of HC dose on the association between 25(OH)D and CRP
Because we observed a positive association between 25(OH)D and CRP among women HC users (Fig. 3), we assessed whether total HC dose affected this association. After adjusting for age, waist circumference, physical activity, ethnicity, and season, women who took <1 mg/day total hormone had lower 25(OH)D concentrations than those who took ≥1 mg/day (mean±standard error: <1 mg/day=76.4±2.7 nmol/L; ≥1 mg/day=85.1±4.5 nmol/L; p=0.0475), but circulating CRP concentrations were similar across women HC users regardless of daily hormone dose (<1 mg/day: 2.8±0.3 mg/L, ≥1 mg/day: 2.8±0.4 mg/L; p=0.8544). In separate adjusted linear regression models of women taking <1 mg/day and women taking ≥1mg/day, we observed no association between 25(OH)D and CRP in either group.
Discussion
The present study assessed the effect of HC use on circulating 25(OH)D across ethnic groups and examined whether HC use modifies the association between 25(OH)D and the inflammatory biomarker CRP in an ethnically diverse population of young adults. Consistent with some previous research, 13 we observed a positive association between 25(OH)D and CRP. Women HC users had the highest plasma concentrations of 25(OH)D, as well as CRP, suggesting that HC use might have confounded these associations. Indeed, there was no longer an association between 25(OH)D and CRP when they were examined separately in men and women HC non-users. Within women HC users, a positive association between 25(OH)D and CRP was no longer significant once we examined those who took <1 mg/day and ≥1 mg/day total hormone separately, suggesting that hormone dose may have confounded the initial association.
Other studies have examined the effect of HRT on the association between vitamin D and various cancers among post-menopausal women. 22,30 However, to our knowledge, the present study is the first to examine whether HC use confounds the association between 25(OH)D and inflammation. In the present study, a confounding effect of HC use was observed in a mixed, ethnically diverse population consisting of both men and women. Women HC non-users and men had similar 25(OH)D and CRP concentrations, whereas women HC users had higher concentrations of both. These results highlight the importance of accounting for HC use in studies of the relationship between vitamin D and inflammation-related health outcomes, if these studies include subjects taking these medications.
Despite a wealth of evidence from in vitro and animal studies suggesting an important role for vitamin D in modulating inflammation, epidemiologic and clinical studies assessing the effects of vitamin D on inflammation have yielded inconsistent results. 7 –13 Vitamin D is thought to exert its anti-inflammatory actions by binding to the vitamin D receptor (VDR) in target tissues. Indeed, most immune cell types express the VDR, 37 which is a transcription factor that, upon binding to 1,25-dihydroxyvitamin D [1,25(OH)2D], the biologically active vitamin D metabolite, regulates the transcription of hundreds of genes, including many that are involved in innate immunity. 38 While a number of biological, demographic, and lifestyle factors may help explain the unexpected positive association between 25(OH)D and inflammation in some human studies, HC use has often been overlooked as a potentially important confounder. Use of HC, which most often consists of a combination of synthetic estrogen and progestins, 39 has been associated with elevated 25(OH)D. 20 The potential effects of progesterone-derived HC ingredients on vitamin D metabolism are not well understood. However, estrogen may upregulate 1α-hydroxylase, the enzyme that converts 25(OH)D to 1,25(OH)2D, as well as the VDR and vitamin D binding protein, which is the main vitamin D metabolite carrier in the circulation. 22,40,41 Estrogen also appears to downregulate vitamin D 24-hydroxylase, the main catabolic enzyme in the vitamin D pathway. 22,42 Together, these actions may result in elevated circulating vitamin D metabolites, although the clinical significance of this effect remains unknown. HC use has also been associated with changes in numerous physiologic pathways, increased inflammation, and a poorer metabolic profile. 23,24,28,29,31 Our finding that adjustment for HC use attenuates a positive association between 25(OH)D and CRP might partly account for some of the unexpected results of previous studies.
Recently, a cross-sectional analysis of data from the United States National Health and Nutrition Examination Survey reported a positive association between 25(OH)D and CRP among those with 25(OH)D ≥52.5 nmol/L. Conversely, the relationship between 25(OH)D and CRP was inverse among those with lower vitamin D status. 13 In the present study, we found no association between 25(OH)D and CRP in those below the median 25(OH)D concentration, and an initially positive association between 25(OH)D and CRP in those above the median was no longer significant after adjustment for HC use. It is possible that the previously observed 13 positive association between 25(OH)D and CRP among individuals with a higher vitamin D status may be due to unaccounted-for HC use among women.
The present study also aimed to assess the effect of HC use on 25(OH)D concentrations across several ethnic groups. To our knowledge, few studies have examined the effect of HC use on vitamin D status in non-Caucasian individuals, and those that did focused on individuals of African ancestry only. 16,21 In the present study, we observed that, across all ethnic groups, women HC users had significantly higher circulating 25(OH)D than women HC non-users and men, even after adjusting for factors known to influence vitamin D concentrations. These observations corroborate previous findings that HC use elevates circulating 25(OH)D. 16,20,43 Furthermore, our results suggest that the effect is consistent across ethnic groups. The magnitude of the effect of HC use on 25(OH)D concentrations across ethnic groups was similar to that observed in previous studies in Caucasians, with women HC users having values over 20 nmol/L higher than women HC non-users, who had 25(OH)D concentrations similar to men. Our observation that 25(OH)D concentrations were higher in women taking ≥1 mg/day total hormone than those taking <1 mg/day suggests that the effect of HC on 25(OH)D may be dose-dependent.
We observed that the association between 25(OH)D and dietary vitamin D differed across ethnic groups. Vitamin D can be obtained exogenously from the diet and supplements or produced endogenously in the skin after exposure to sunlight. 14 Dark-skinned individuals are less able to produce vitamin D endogenously because of a higher skin melanin content, and exogenous sources may contribute more to vitamin D status in these individuals. 18 In the present study, while dietary vitamin D contributed to 25(OH)D concentrations in all ethnic groups, the correlation was weaker among Caucasians and East Asians than among South Asians. The stronger correlation between 25(OH)D and dietary vitamin D observed among South Asians may partly reflect a decreased ability to produce vitamin D endogenously because of generally darker skin, so that dietary vitamin D intake becomes a more important source of 25(OH)D. However, no information was available on lifestyle variables that may affect sun exposure, such as use of long-sleeved clothing or sunscreen. Therefore, we cannot determine whether other lifestyle factors specific to these individuals also contributed to decreased endogenous vitamin D production.
We noted an initial positive association between 25(OH)D and CRP among women HC users. However, this association was no longer significant after we examined HC users who took <1 mg/day and ≥1 mg/day total hormone separately. As noted earlier, we observed a dose-dependent association between HC dose and 25(OH)D among women HC users, which might partly explain the initial positive association between 25(OH)D and CRP observed in this group. However, CRP concentrations were equally elevated in women taking<1 mg/day versus ≥1 mg/day total hormone. It is possible that the initial positive association observed between 25(OH)D and CRP among women HC users as a whole was due to residual confounding.
One limitation of the present study is the smaller sample size of women HC users across ethnic groups, particularly South Asians. Another limitation is the lack of information on menstrual cycle stage and circulating sex hormone concentrations, which prevented us from investigating the potential role of natural fluctuations in estrogen and progesterone in modulating the association between 25(OH)D and CRP. We were also unable to explore whether estrogen or progestin-derived HC components have a greater effect on the observed associations.
Conclusions
In the present study we identified a confounding effect of HC use on the association between 25(OH)D and CRP in an ethnically diverse population of young adults. An apparent positive association between 25(OH)D and CRP was no longer significant after adjusting for HC use. In addition, we noted that HC use increased 25(OH)D concentrations significantly across ethnic groups. Overall, our results bring to light the importance of considering lifestyle variables, particularly HC use, as significant confounders in the relationship between vitamin D and inflammation, as well as, potentially, other health outcomes.
Footnotes
Acknowledgment
This work was supported by a grant from the Advanced Foods and Materials Network (305352 to AE-S).
Disclosure Statement
No competing financial interests exist.