
Abstract
Background:
Efforts to increase mammographic screening for early detection of breast cancer among women of lower socioeconomic class and ethnic minorities have been largely unsuccessful. This study explores the receptivity of hospitalized women to inpatient mammography as a novel approach to enhance breast cancer screening.
Methods:
A cross-sectional study was conducted among 210 hospitalized women, aged 50–75 years, admitted to the medicine services at Johns Hopkins Bayview Medical Center in early 2012. Unpaired t-test and Chi-square tests were used to compare characteristics, barriers, and receptivity to inpatient mammography among women adherent and non-adherent to screening guidelines.
Results:
One-third of women enrolled were African American, and 60% of study participants reported an annual household income of <$20,000. Thirty-nine percent were overdue for screening, of which, 13% never had a mammogram and 28% were at high risk for breast cancer (Gail score ≥1.7%). The commonly reported barriers to screening mammograms were failure to remember appointments and lack of transportation. Most women (91%) believed that it is important for healthcare providers to discuss breast cancer screening while patients are in the hospital. Sixty-eight percent of non-adherent women would agree to have an inpatient screening mammogram if it was due and offered.
Conclusions:
A significant number of hospitalized women from lower socioeconomic class are at high risk of developing breast cancer and non-adherent to mammographic screening. Inpatient hospital stay may be a feasible time for screening and education to ensure adequate breast care and promote screening among these women.
Introduction
Breast cancer is now the most commonly diagnosed cancer globally among women and the leading cause of cancer death. 1 In the United States during 2012, an estimated 226,870 new cases of invasive breast cancer and 39,510 breast cancer deaths are expected among women. 2 Mortality from breast cancer has steadily decreased in women since 1990 as a result of progress in early detection, improved treatment, and recently decreased incidence. 2 Mammography remains the screening test of choice 3 and has reduced breast cancer mortality by 22%–35% among women age 50 years and older. 4 Despite the steady utilization of screening mammography (67.1% in 2008), studies suggest that women older than 50 years, low-income, uninsured, and minorities (especially African Americans) are initiating mammography later than recommended, not having mammography at recommended intervals, and not receiving appropriate follow-up after a positive screen. 5 –7
According to the National Health Interview Survey, women aged 40 years and older reporting a mammogram within the past two years increased from 29% in 1987 to 70% in 2000. 8 Thereafter, the prevalence of mammogram screenings has been gradually trending down. Breen et al. reported that breast cancer screening was on a decline from 2000 to 2005—with the largest drop occurring among women 50–59 years old. 9 The mammography rates remain lowest among the uninsured (35.6 %), and low income women. 8 –10 Studies have also shown that physicians tend to recommend mammography more frequently to well-educated, white women who have annual incomes above $20,000. 11 This unequal emphasis may partially explain the lower screen rates seen among the uninsured, minorities, and low income women. 8,11,12 Daily and colleagues found that women living in disadvantaged areas were less likely to have screening mammography, even after adjusting for individual-level socioeconomics and access to health care. 13 Some of the well documented barriers to an outpatient screening mammogram, including patient preferences, appear to be even greater obstacles in these low socioeconomic areas. 14,15
Breast cancer screening is traditionally offered exclusively in outpatient settings, however for some women having a screening mammography while an inpatient may be a more practical and preferable option that has not been studied. The purpose of this study is to identify characteristics and barriers associated with non-adherence of mammographic screening among an ethnically diverse, predominantly low socioeconomic class of hospitalized population and evaluate their receptivity to screening during their inpatient stay.
Methods
Study design and sample
All women between 50 and 75 years admitted to the general medical service at Johns Hopkins Bayview Medical Center between October 2011 and January 2012 were approached for participation in this cross-sectional study. This age range was selected in accordance with breast cancer screening recommendations from the United States Preventive Services Task Force (USPSTF). 16 Patients with a history of breast cancer, or comorbidities that could either impact survival or make them ineligible to have a mammogram were excluded. This included patients with current hospitalization for dementia, mental status change, acute myocardial infarction, and acute stroke. Fifty-seven percent of the study population was independent, 10% were wheelchair bound, and 33% were on chronic disability. Patients who had multiple admissions during the study period were only enrolled on their first visit. The patients were consented during their hospitalization and survey data was collected via bedside interview taking approximately 15 minutes to complete.
Four hundred and forty one women admitted to the medicine service between October 2011 and January 2012 were eligible for the study based on their age. Of these, 49 (11%) refused to participate, 43 (10%) had a prior history of breast cancer, 83 (19%) were admitted with altered mental status, and 56 (13%) women were discharged from the hospital before the study coordinator could consent them, leaving a study population of 210 women.
Protocol and measures
The survey consisted of questions regarding sociodemographic information, breast cancer risk factors including reproductive history, history of mammographic screening, breast biopsies, and receptivity or preferences related to inpatient screening mammography. Women age 52 or above who reported having a mammogram within the last 2 years or 24 months were classified as being adherent, and women reporting a screening mammogram more than 2 years or 24 months from the study survey were classified as being non-adherent. In our sample, there were 15 women aged 50–51 years. Ten had a screening mammography within the last 24 months; these women were characterized as being adherent. The remaining 5 who had not been screened within the prior 24 months were also considered to be adherent with the USPSTF guidelines because they had 12 more months during which they can be screened. We evaluated access to health care with the variables health insurance status and having a primary care physician. Disease burden was characterized by assessing medical comorbidities. Several questions inquired about breast care during their current hospital stay, including whether any hospital provider had examined their breasts or talked to them about breast cancer screening. A few questions were also used to evaluate the women's knowledge about breast cancer screening, perceived susceptibility, and the barriers to screening. Most of the knowledge, susceptibility, and barrier-related questions were adapted from Champion's Health Belief Model Scale for breast cancer screening.
17
The participants were then asked if they thought it was important for the hospital providers to discuss breast cancer screening with them during the hospital stay and if they would agree to have an inpatient screening mammogram if it was due and offered. At the end of the interview, these women were educated about breast cancer and educational material was provided for breast cancer screening. The risk for developing breast cancer within the next 5 years was estimated using the National Cancer Institute Breast Cancer Risk Tool (the Gail model,
Pilot testing of the survey was conducted on fifteen patients to ensure that questions were clear and not ambiguous. This study was approved by Institutional Review Board at Johns Hopkins Bayview Medical Center.
Statistical methods
Respondent characteristics are presented as proportions and means. Unpaired t-test and Chi-square tests were used to compare demographic and socioeconomic characteristics, barriers to screening mammography, and receptivity to inpatient mammography among women adherent and non-adherent to screening guidelines.
Results
The mean age for the total study population was 60 years; 32% of the women were African American, 60% of women reported annual household income less than $20,000, and 5% were uninsured (Table 1). Average 5-year Gail risk of breast cancer was 1.6%. One-third of the study population (32%) was at high risk for breast cancer based on a 5-year-risk prediction of ≥1.7% using the Gail model. Thirty-nine percent of the hospitalized women in our study were overdue for a screening mammogram (non-adherent), including 13% who had never had a mammogram; 28% of the non-adherent women were also at high risk for breast cancer (Gail score ≥1.7%).
Chi-Square test (Yates corrected p value where at least 20% of frequencies were <5).
Unpaired t test statistic.
Comorbidities included: diabetes, hypertension, heart disease, chronic kidney disease, stroke, congestive heart failure, chronic obstructive pulmonary disease, and cancers other than skin or breast.
Family history of breast cancer was defined as breast cancer in first-degree relatives like mother, sisters, or daughters.
Gail score estimated using the National Cancer Institute Breast Cancer Risk Tool (
BMI, body mass index; SD, standard deviation.
Characteristics for adherent and non-adherent women are shown in Table 1. More non-adherent women had annual incomes of less than $20,000 and a history of a prior stroke. Ninety-four percent of adherent group had a primary care provider versus 85% of the non-adherent group (p=0.04). Non-adherence rates were not statistically different across the age groups (36%, 43%, and 39% in the 50–59, 60–69, and 70–75 years age groups respectively [p=0.69], as shown in Fig 1).
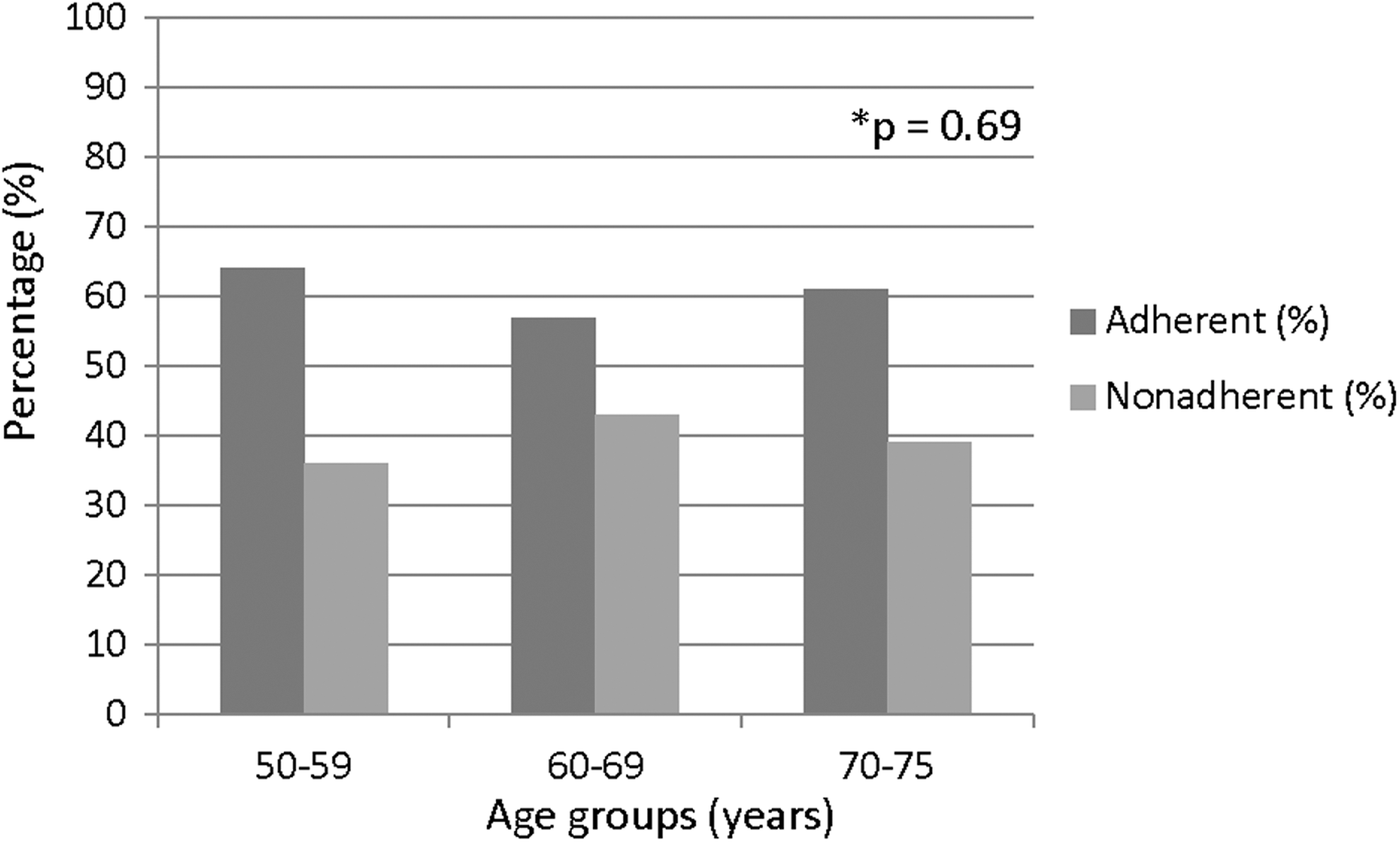
Percentage of adherence and non-adherence for screening mammography by age group. *Chi-Square test–p value for difference in percentage of non-adherent women between age groups.
As shown in Table 2, the most commonly cited barrier to breast cancer screening was “I have other problems more important than getting a mammogram.” Several barriers to breast cancer screening were perceived differently between the two groups, including “I cannot remember to schedule a mammogram” (27% among adherent and 16% in non-adherent, p=0.05) and “No transportation to get to the test” (17% among adherent and 29% in non-adherent, p=0.04). There were no statistical differences between the two groups about knowledge or perceived susceptibility. The two groups were also equally aware of the benefits of screening mammography (Table 2).
Chi-Square test.
Chi-Square with Yates corrected p value where at least 20% of frequencies were <5.
In evaluation of preference for inpatient screening among hospitalized women (Table 3), only 5% (n=11) of women reported that someone had talked to them about breast cancer screening during their inpatient stay, and 3% (n=7) of women reported having a clinical breast examination during that time. Almost all women (91%) believed that it is important for healthcare providers to discuss breast cancer screening while patients are in the hospital. Three-quarters of the women studied (n=159, 76%) indicated that they would agree to have an inpatient screening mammogram if it was due and it was offered. Eighty percent of the adherent women and sixty-eight percent of the non-adherent women (p=0.04), including 27% of women who had never had a mammogram, confirmed that they would be willing to have a screening mammogram during the hospital admission.
Chi-Square test.
Chi-Square with Yates corrected p value where at least 20% of frequencies were <5.
Discussion
More than one-third of the hospitalized women surveyed in our study were non-adherent and therefore overdue for a screening mammogram despite being aware of the potential benefit. The majority of these women responded that they would be agreeable to breast cancer screening performed during the hospitalization. While this study did not delve deeper into this willingness to be screened during the current hospital admission, time in the hospital is known to promote reflection and deeper consideration of health and behaviors. 24 Notwithstanding the recent change in the breast cancer screening interval recommendations from annual to biennial by USPSTF, 16 significant barriers to the screening still exist. Access to mammography during a hospital admission, which eliminates barriers like transportation and convenience, makes the offering of inpatient mammogram germane for increasing screening rates. 25,27 This study confirms prior reports that have shown decreased breast cancer screening among women from low socioeconomic status and those lacking primary care providers. 27 –31 For hospitalized women, particularly those at high risk of developing breast cancer, seizing the moment and performing inpatient mammography at a time when potential barriers are negated seems like a judicious strategy.
Some of the barriers that women cited in our study need to be further explored, like “I have other problems more important than getting a mammogram.” While “other problems” may have been interpreted widely by patients, medical comorbidities must have been among those at the forefront of their minds given the context of the hospitalization for acute illness. Further, while it is likely that multiple comorbidities may deter women from having screening tests, we did not detect significant differences in comorbidities between adherent and non-adherent groups. With the evolution of hospital medicine over the last decade, hospitalists have affirmed their expertise in providing comprehensive medical care to their patients and partnering with outpatient provider to deliver quality. Huth et al. retrospectively reviewed breast cancer screening practices among hospitalized women and concluded that hospital providers failed to seize the opportunity to initiate breast cancer screening during the hospitalization. 32 In Huth's study, women were hospitalized for a median of 6 days, breast cancer screening history was documented in 25% of cases, breast examination was performed on 37% of women, and mammography history was recorded in only 7.5% of hospital admissions. 32 No prior study of which we are aware has assessed breast cancer risk or preferences related to breast cancer screening among the hospitalized women. Consistent with the data above, we found that breast examination and breast cancer screening education during the hospital stay occurred infrequently. This is likely because breast issues were not tied to the reason for the acute hospitalization. However, because 91% of the women studied believed that it was important for hospital-based providers to discuss breast cancer screening during the hospitalization, the failure to do this could result in a missed opportunity for early detection of breast cancer.
A significant proportion of the non-adherent women (28%) carried a high 5-year-risk for breast cancer (using Gail model ≥1.7%). Thus, mammography needs to be a high priority whenever and wherever these patients interface with the healthcare system. Ethicists might suggest that inpatient providers who are not ordering mammograms for women known to be at very high risk for developing breast cancer and who are overdue for the test might be failing to abide by the physician charter's principle of the primacy of patient welfare.
33
One feature of accountable care will be to offer patients recommended testing when they interface with our systems of care.
34
It is interesting to note that some states mandate hospitals to offer all inpatient women over the age of 18 a Papanicolaou (Pap) test to screen for cervical cancer unless the patient refuses, there is documentation of a Pap within the past 12 months, or the physician orders otherwise.
35
However, no such legislation exist
Physician recommendations for screening have consistently been shown to strongly influence patient behaviors.
36
Over the course of several days as hospitalists forge trusting relationships with patients, these physicians can prompt and inspire patients to consider, if not undergo, cancer screening that is overdue. This time together may result in partnerships that can result in shared decision-making between patients and healthcare providers around critical decisions, related both to health maintenance and the presenting illness.
15
Several limitation
Conclusion
Since early detection translates into reduced mortality, there is a need to optimize cancer prevention for breast cancer. It appears that women admitted to the hospital would value the opportunity to have breast cancer screening addressed during their stay. Because hospitalization is a unique time during which patients are a captive audience who are reflecting upon their health, there is tremendous potential for hospitalists to provide comprehensive care for the whole patient. This could in turn have a major impact on public health, particularly if these patients share their new knowledge and perspectives with those in their sphere of influence—friends and family. Future studies are required to evaluate the practical aspects such as the feasibility and financing of prevention and screening for breast cancer while patients are hospitalized.
Footnotes
Acknowledgments
Dr. Wright is a Miller-Coulson Family Scholar, and this support comes from the Hopkins Center for Innovative Medicine.
Disclosure Statement
No competing financial interests exist.