
Abstract
Background:
Mortality from coronary heart disease (CHD) in women in Japan is one of the lowest in developed countries. In an attempt to shed some light on possible reasons of lower CHD in women in Japan compared with the United States, we extensively reviewed and analyzed existing national data and recent literature.
Methods:
We searched recent epidemiological studies that reported incidence of acute myocardial infarction (AMI) and examined risk factors for CHD in women in Japan. Then, we compared trends in risk factors between women currently aged 50–69 years in Japan and the United States, using national statistics and other available resources.
Results:
Recent epidemiological studies have clearly shown that AMI incidence in women in Japan is lower than that reported from other countries, and that lipids, blood pressure (BP), diabetes, smoking, and early menopause are independent risk factors. Comparing trends in risk factors between women in Japan and the United States, current levels of serum total cholesterol are higher in women in Japan and levels have been similar at least since 1990. Levels of BP have been higher in in Japan for the past 3 decades. Prevalence of type 2 diabetes has been similar in Japanese and white women currently aged 60–69 for the past 2 decades. In contrast, rates of cigarette smoking, although low in women in both countries, have been lower in women in Japan.
Conclusions:
Differences in risk factors and their trends are unlikely to explain the difference in CHD rates in women in Japan and the United States. Determining the currently unknown factors responsible for low CHD mortality in women in Japan may lead to new strategy for CHD prevention.
Introduction
Japanese women in Japan have experienced the greatest longevity for the past 25 years. 1 This is partly due to a constant decline in mortality from coronary heart disease (CHD) since the 1960s, although CHD mortality in women in Japan was one of the lowest in developed countries. 2 Low CHD mortality in Japan in the 1960s was attributed to low dietary intake of saturated fat and cholesterol, resulting in low serum levels of total cholesterol (e.g., 160 mg/dL in Japan and 240 mg/dL in the United States). 3 The hypothesis at that time was that with Western acculturation, CHD rates in Japan would increase. In fact, CHD mortality in Asian countries has increased with concomitant rise in serum total cholesterol except for Japan. 4,5 Between 1960 and 1990, dietary intake of both total fat and animal protein almost tripled, 6,7 and the current dietary intake of cholesterol in women in Japan is higher than in the United States (i.e.,199 vs. 128 mg/1,000 kcal). 8 The current levels of total cholesterol in women aged 50–69 years in Japan are higher than those in the United States. 9 The absence of increase in CHD is unusual, given that during this period, dietary-related diseases (e.g., colon and breast cancer in women and colon and prostate cancer in men increased substantially). 10 It is important to note that low CHD mortality in women in Japan is not a function of high mortality from other causes (e.g., stroke, cancer). 1
Low CHD mortality in Japanese in Japan does not appear to be due primarily to genetics or host susceptibility because CHD incidence and mortality increased substantially in Japanese migrants to the United States within one to two generations. 11 Additionally, we have recently documented that levels of atherosclerosis assessed as calcification of the coronary artery and aorta and intima-media thickness (IMT) of the carotid artery in Japanese American men are not only higher than those in Japanese men in Japan, but are also higher compared with white Americans. 12,13 We have previously reported that low CHD mortality in middle-aged men in Japan compared with the United States is very unlikely due to misclassification of cause of death, 14 difference in risk factors, 15,16 or cohort effect. 16 In an attempt to shed some light on possible reasons of lower CHD in women in Japan compared to the United States, we extensively reviewed and analyzed existing national data and recent literature.
Materials and Methods
Data on CHD mortality were obtained from the World Health Organization (WHO) Statistical Information System (
To compare trends in risk factors between women in Japan and the United States, data were obtained from the National Health and Nutrition Examination Surveys (NHANES) in the United States, 18,19 the National Health and Nutrition Survey and the National Survey of Cardiovascular Diseases in Japan 6,7,20 as well as published articles (Table 1). 21 –23 Prevalence of diabetes in white women in 2007–2010 in the United States was estimated using the NHANES dataset available at a web site of the Centers for Disease Control and Prevention. 19
AMI, acute myocardial infarction; NHANES, National Health and Nutrition Examination Survey; NHNS, National Health and Nutrition Survey; NSCD, National Survey of Cardiovascular Diseases; WHO, World Health Organization.
For incidence of acute myocardial infarction (AMI) and the association of risk factors with CHD in women in Japan, we identified epidemiological studies published after 2001 that reported the data in women and men separately, because no previous epidemiological studies in Japan reported the association only in women. We identified these studies using review papers we and others published in 2008, 24,25 articles citing these review papers, a website listing cardiovascular epidemiology studies conducted in Japan with their publications, 26 and PubMed.
Results
Between 1995 and 2004, age-adjusted CHD mortality in women was declining in each country (Fig. 1). During this period, women in France and Japan had the lowest and women in the United Kingdom and the United States had the highest CHD mortality. A five-fold difference existed in aged-adjusted CHD mortality (per 100,000) in 2004 between Japan and the United States: 13.5 in Japan verses 65.6 in the United States.

Recent trend in aged-adjusted mortality from coronary heart disease in women in selected countries. Data were obtained from the World Health Organization Statistical Information System (
AMI incidence in women in Japan, evaluated using the protocol of the WHO MONICA Project (Monitoring of Trends and Determinants in Cardiovascular Disease) 27 was much lower compared to other countries. The Takashima AMI Registry covering about 55,000 individuals reported that age-adjusted incidence of AMI in women aged 25–74 years was 18.0/100,000 28 and that the incidence was the lowest as compared to the incidence in registries from the WHO MONICA Project. 27 Age-adjusted incidence of AMI in women aged 35–64 in Takashima was 9.1/100,000, which was less than a tenth of that in the United Kingdom (256/100,000), the United States (139/100.000), and Finland (86–165/100,000) and even less than a half of that in France (37–77/100,000), and China(37/100,000). 28 AMI incidence in women in other registries in Japan was reported and similarly low. 24,29
Additionally, there is little evidence that AMI incidence in women in Japan has increased recently. The MIYAGI-AMI registry study, which covers more than 2 million individuals, the largest AMI registry in Japan, reported AMI incidence in women between 1979 and 2009. 30 Age-adjusted incidence of AMI in women remained similar or appeared to be slightly decreasing between 1987 and 2008, although it increased between 1979 and 1986. The Circulatory Risk in Communities Study (CIRCS) which covers more than 30,000 individuals reported that age-adjusted incidence of sudden cardiac death in women in Japan significantly decreased from 1981 to 2005. 31 Age-adjusted incidence of sudden cardiac death (per 100,000) was 50.6, 39.5, 27.1, 16.7, and 18.2 during 1981–1985, 1986–1990, 1991–1995, 1996–2000, and 2001–2005 respectively. Although the Takashima AMI registry reported a significant increase in AMI incidence in women from 1990–1992 to 1993–1995, there was no increase since 1993–1995 to 1999–2001. 32 Several other studies reported trends in AMI incidence in women in Japan but the number of cases was too small to examine the trend. 33 –36
Up until 2009, epidemiological studies did not show significant independent associations of lipids with CHD in women in Japan (Table 2). 37 –42 Japan Atherosclerosis Longitudinal Study-Existing Cohorts Combine (JALS-ECC), a project pooling the data from cohort studies in Japan examined the association of total cholesterol and non-high-density lipoprotein cholesterol (non-HDL-C) with AMI incidence in 13,477 women and 8,953 men aged 40–89 years at baseline with an average follow-up of 7.6years. 38 The study reported that among women incidence rate ratio for one standard deviation (SD) increase of cholesterol was 1.54 (95% confidence interval [CI]: 1.14–2.09) after adjusting for body-mass index (BMI), blood pressure (BP), diabetes, high-density lipoprotein cholesterol (HDL-C), and current smoking. Similarly, among women incidence rate ratio for one SD increase of non-HDL-C was 1.65 (95% CI: 1.22–2.24) after adjusting for the same variables. Following JALS-ECC, CIRCS examined the association of low-density lipoprotein cholesterol (LDL-C) with CHD and AMI incidence in 4,897 women and 3,079 men aged 40–69 years at baseline and reported that among women hazard ratio for AMI incidence for one SD increase of LDL-C was 1.42 (95% CI,1.05–1.91) after adjusting for categories of BP, glucose, HDL-C, and triglycerides, medications for BP and lipids, BMI, smoking status and other variables. 37 Likewise, among women hazard ratio for CHD for one SD increase of LDL-C was 1.25 (95% CI, 1.00–1.55) after adjusting for the same variables. Similarly, recent epidemiological studies in women in Japan reported a significant independent association of each of other traditional risk factors (i.e., BP, 40,43 –47 diabetes, 29,40,48 cigarette smoking 49 –51 ) (Table 3) and early menopause. 52
Multivariate adjustments:
CIRCS: age, blood pressure category, antihypertensive medication use, glucose category, body mass index, smoking status, alcohol intake category, lipid lowering medication use, categories of HDL-C, and triglycerides, fasting status, years at entry, and study areas;
JALS-ECC: age, body mass index, HDL-C, blood pressure, diabetes, and current smoking;
The Suita Study: age, body mass index, diabetes, HDL-C, cigarette smoking category, and alcohol intake category;
The JMS cohort study: age, systolic blood pressure, diabetes, and current smoking;
The JACC study: systolic blood pressure, HDL-C, ethanol intake, smoking status, and diabetes;
NIPPON DATA: age, serum albumin, body mass index, hypertension, diabetes, cigarette smoking category, and alcohol intake category.
CHD, coronary heart disease; CIRCS, The Circulatory Risk in Communities Study; HR, hazard ratio; IRR, incidence rate ratio; JACC, Japan collaborative cohort study for evaluation of cancer risk; JALS-ECC, the Japan Arteriosclerosis Longitudinal Study-Existing Cohorts Combine; JMS cohort, Jichi Medical School cohort; LDL-C, low-density-lipoprotein cholesterol; MI, myocardial infarction; NIPPON DATA, the National Integrated Project for Prospective Observation of Noncommunicable Disease and Its Trends in the Aged; non-HDL-C, non-high-density-lipoprotein cholesterol; SD, standard deviation; TC, total cholesterol.
Variables adjusted in multivariate adjustment in blood pressure analysis:
JPHC: age;
The JMS cohort study: age, diabetes, total cholesterol, and current smoking;
JALS: age, body mass index, total cholesterol, and current smoking;
Suita: age, body mass index, diabetes, hyperlipidemia, smoking, and drinking status;
Iso H.: age, community, total cholesterol, smoking, alcohol intake category, time since last meal, and menopausal status;
NIPPON DATA: age, body-mass index, total cholesterol, diabetes, cigarette smoking category, and drinking category.
†Variables adjusted in multivariate adjustment in diabetes analysis:
Suita: age, body-mass index, hypertension, hyperlipidemia, smoking, and drinking status;
JMS: age, systolic blood pressure, total cholesterol, and current smoking;
Hisayama: age, systolic blood pressure, electrocardiogram abnormalities, body-mass index, total cholesterol, and HDL-C smoking, alcohol intake, and regular exercise.
‡Variables adjusted in multivariate adjustment in cigarette smoking analysis:
JPHC, TPCS, JACC: age, cohort, and number of years smoked;
Suita: age, body-mass index, blood pressure, non-HDL-C, glomerular filtration rate, and alcohol drinking;
JPHC: age, alcohol, frequency of fruit, vegetable, fish, history of hypertension, diabetes, and hyperlipidemia as well as public health center.
JPHC, Japan Public Health Center-based Prospective Study; TPCS, Three Prefecture Cohort Study.
Figure 2 shows levels of serum total cholesterol in women in Japan and the United States in the most recent data and data around 1990. 6,18 –20 Comparing the most recent data in women currently aged 50–69 years, levels of serum total cholesterol were higher in women in Japan than in the United States. Moreover, in this birth cohort of women, levels of serum total cholesterol in Japan and the United States were very similar around 1990. Thus, among women currently aged 50–69 years, serum levels of total cholesterol in Japan had been similar or higher as compared wit the United States at least for the past two decades.
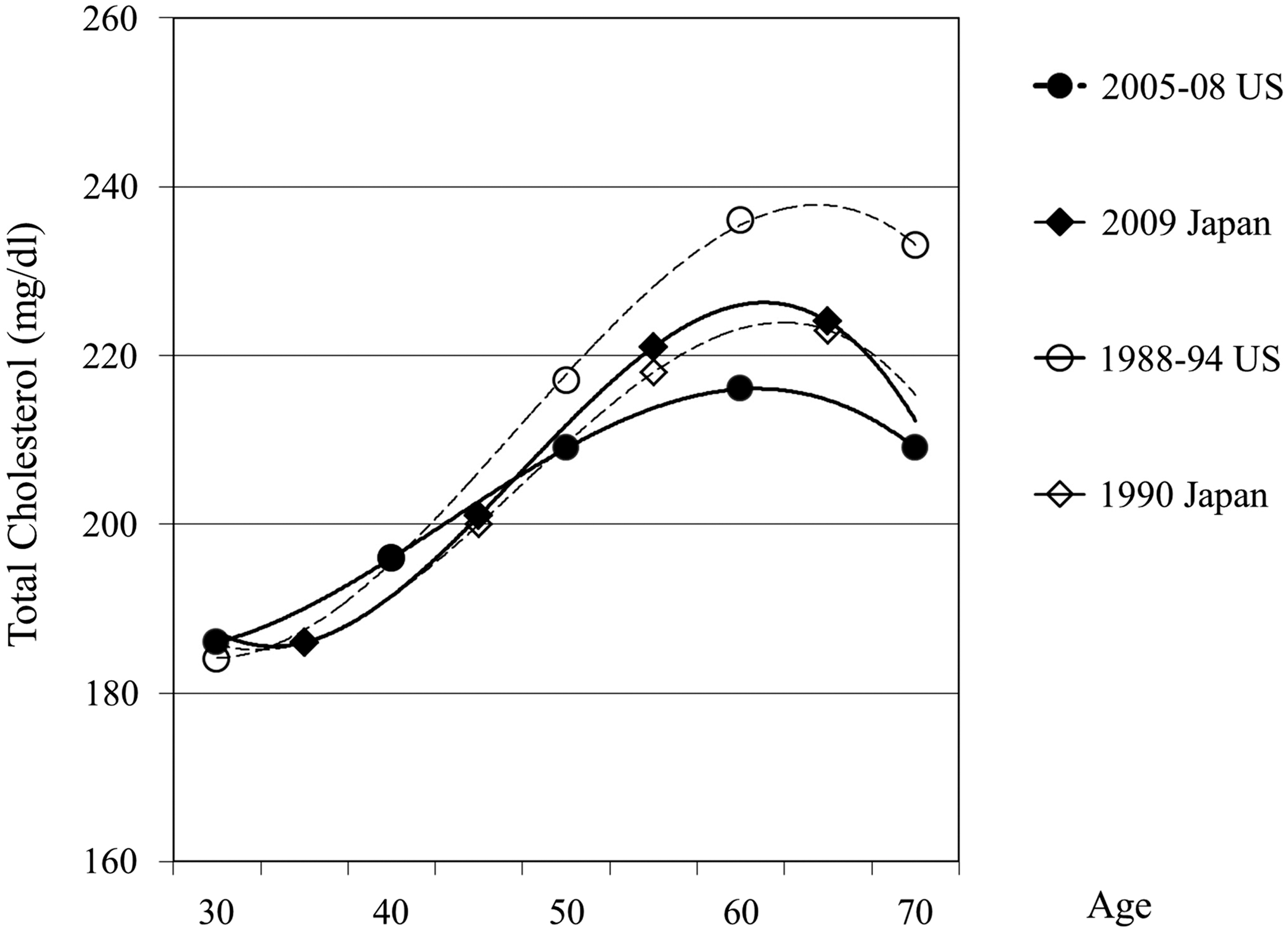
Trend in serum total cholesterol in women in Japan and the United States.
Figure 3 shows levels of systolic BP in women in Japan and white women in the United States in the most recent data and data around 1990. 6,18 –21 Comparing the most recent data in women currently aged 50–69 years, levels of systolic BP were high in women in Japan. Furthermore, in this birth cohort, levels of systolic BP were much higher in Japan than in the United States around 1990. Thus, among women currently aged 50–69 years, levels of systolic BP in Japan had been higher than in the United States at least for the past two decades. Similarly, we observed that among women currently aged 50–69 years, levels of diastolic BP in women in Japan had been higher than the United States at least for the past two decades (Fig. 4).

Trend in systolic blood pressure in women in Japan and the United States.

Trend in diastolic blood pressure in women in Japan and the United States.
Figure 5 shows trends in prevalence of current smokers in women in Japan and in the United States. 6,18 –20 Prevalence of current smokers had been consistently lower in women in Japan than in the United States for the past three decades. For example, prevalence of current smokers in women in Japan aged 50–59 years in 2008 was 14.8%. In this birth cohort, the prevalence was 6.8% in 2000, 17.2% in 1990, and 16.2% in 1980. The prevalence of current smokers in women aged 45–64 years in the United States in 2005 was 18.8%. In this birth cohort, the prevalence was 32% in 1985. Thus, among women currently aged 50–69 years, prevalence of current smokers in Japan had been lower than in the United States for the past three decades.
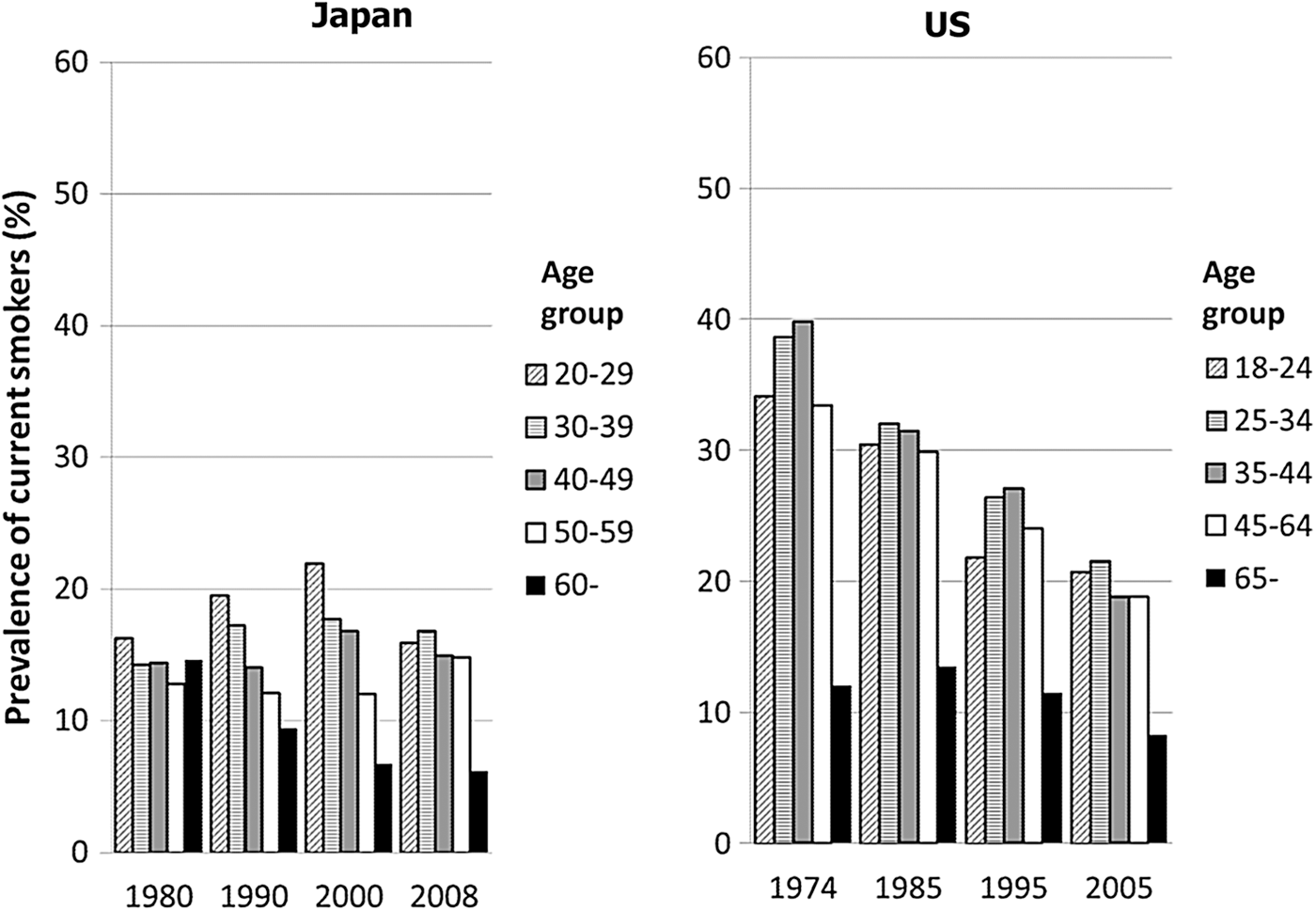
Trend in rates of cigarette smoking in women in Japan and the United States.
Prevalence of type 2 diabetes and impaired glucose tolerance (IGT) diagnosed by the 1985 WHO criteria 53 was similar in women in Japan and white women in the United States in 1990. Prevalence of type 2 diabetes and IGT in women in Japan was 3∼4% and 12∼13% in their 40's, respectively and 7%∼9% and 12∼19% in their 50's, respectively. 23 NHANES III (1988–1994) reported that prevalence of type 2 diabetes and IGT in white women was 5% and 11% in their 40's, respectively and 10% and 15% in their 50s, respectively. 54 Recent data on prevalence of type 2 diabetes based on hemoglobin Ac1 (HbA1c) show that prevalence of type 2 diabetes was similar between women aged 60–69 years (i.e., 14.1% in Japanese 7 and 15.7% in whites), although prevalence was lower in women in Japan than in white women aged 50–59 (i.e., 5.6% in women in Japan 7 and 11.9% in white women). Thus, in women currently aged 60–69 years, prevalence of glucose intolerance had been similar for the past 2 decades, whereas in women currently aged 50–59 years, prevalence of type 2 diabetes was much lower in women in Japan than white women in the United States.
Discussion
This review of recent cardiovascular epidemiological studies in Japan has shown that traditional risk factors are independently associated with CHD in women in Japan. Additionally, traditional risk factors among women currently aged 50–69 between Japan and the United States: total cholesterol, BP, rates of cigarette smoking and prevalence of diabetes, have generally been similar for the past few decades.
CHD mortality in women in Japan is one of the lowest among developed countries. The fact that much lower incidence of AMI in women in Japan from multiple registries than in all registries of the WHO MONICA project strongly indicates that low CHD mortality in women in Japan is not due to misclassification of cause of death, but rather, is real. Although CHD mortality in women in Japan is very similar to that in France, AMI incidence in women in Japan is less than a half of that in France. This is, to some extent, due to misclassification of cause of death in women in France. In fact, the WHO MONICA project shows that official CHD death in women in registries in France underestimated actual CHD death by 100%. 55
Epidemiological studies have shown that each of traditional risk factors, i.e., BP, 40,43 –47 lipids, 37,38 diabetes, 27,35,40 cigarette smoking, 49 –51 and age at menopause, 52 is independently associated with CHD in women in Japan. It is noted, however, that all these epidemiological studies were reported after 2003. This is partly because CHD incidence in women in Japan is too low to detect an independent association of each risk factor without a very large sample size. On the other hand, these independent associations are expected based on observations from autopsy studies. The first nationwide autopsy study in Japan among 2,856 subjects aged 0–39 years conducted around 1980 shows that age, BP, and total cholesterol are risk factors for atherosclerosis of the coronary artery and the aorta for both women and men. 56 This study employed the same method to evaluate atherosclerosis with the Pathobiological Determinants of Atherosclerosis in Youth study, which also shows that age, hypertension, LDL-C, and smoking are risk factors for atherosclerosis and that the extent of atherosclerosis is lower in women than in men. 57
We observed that current levels of total cholesterol in women aged 50–69 years are higher in women in Japan than in the United States. Although it is possible that the difference in rates of statin users contributes to the difference in the levels of total cholesterol, available data show that current rates of statin users in middle-aged women are similar: 14% in Japan 58 versus 16% in the United States. 18 It is also possible that levels of HDL-C or LDL-C have been different between women in Japan and the United States, even though the levels of total cholesterol have been very similar. Although we do not have trend data of LDL-C or HDL-C, these levels were comparable in middle-aged women between Japan and the United States around 1990. Data from the Suita Study, the only population-based study in urban area in Japan where >70% of Japanese live, show that in 1990–1994 mean levels of LDL-C and HDL-C (mg/dL) were 126 and 57 in women aged 40–49 years, respectively and 146 and 57 in women aged 50–59 years, respectively. NHANES III (1988–1994) reported that corresponding numbers were 131 and 56 in women aged 45–54 years, respectively and 144 and 56 in women aged 55–64 years, respectively. 59
We observed that levels of BP in currently aged 50–69 years have been higher in Japan than in the United States at least for the past two decades. The difference in clinical guidelines for hypertension in the past accounts to some extent for the differences in levels of BP. For example, the 1990 National Survey of Circulatory Disorders in Japan used the criteria of hypertension as systolic BP ≥ 160 mmHg, or diastolic BP ≥ 95 mmHg, or on hypertension medication, based on the WHO criteria, 60 whereas the Fifth Report of the Joint National Committee on Detection, Education, and Treatment of High Blood Pressure in the United States in 1993 defined hypertension as systolic BP ≥ 140 mmHg or diastolic BP ≥ 90 mmHg. 61
Rates of cigarette smoking have been lower in women in Japan than in the United States, which could partly contribute to lower CHD rates in women in Japan. Meanwhile rates of cigarette smoking in men in Japan have been much higher than in the United States for the past 3 decades (e.g., 70 to 50% in Japan 6,20 versus 40 to 30% in the United States). 15 Passive smoking is an independent risk factor for CHD both in Japan 62 and the US, 63 about 30% higher risk for CHD in passive smokers compared to never smokers. Thus, it is unlikely that the difference in rates of cigarette smoking largely accounts for the difference in CHD rates between women in Japan and the United States.
Our results showed that prevalence of diabetes in women currently aged 60–69 years has been similar between Japan and the United States for the past two decades, whereas that in women currently aged 50–59 years in the United States was almost twice as high as in Japan. Because CHD rates in women aged 50–59 years is lower than that in women aged 60–69 years, the difference in prevalence of diabetes in women aged 50–59 years is unlikely to largely contribute to the difference in CHD rates between Japan and the United States. It is speculated that the difference in the prevalence of diabetes in younger generation is due to the difference in recent trend in BMI between Japan and the United States. 64 Between 1980 and 2010, BMI in women in Japan remained similar whereas that in women in the United States much increased.
It is possible that the difference in BMI contributes to the difference in CHD in women between Japan and the United States. Major plausible intermediary factors linking obesity and CHD are BP, total cholesterol, and type 2 diabetes. 65,66 The current study has shown that it is very unlikely that the difference in these factors contributes to the difference in CHD in women between Japan and the United States. Although we have investigated other possible intermediary factors including C-reactive protein, 12 fibrinogen, 12 adiponectin, 67 D-dimer, 68 von Willebrand factor, 68 and lipoprotein-associated phospholipase A2 69 in our study in men, none of these factors significantly contributed to the difference in atherosclerosis. These observations need to be confirmed in the future study in women.
Early menopause is significantly associated with increased risk of CHD both in Japan 52 and the United States. 70 Meanwhile, associations of age at menarche with CHD are equivocal. 52,71,72 Available data show that the age at natural menopause in women in Japan is earlier whereas the age at menarche is similar between the two countries: 49.3 in Japan versus 51.3 in the United States for menopause and 12.5 in Japan and 12.8 in the United States for menarche. 73 Thus, the difference in age at menopause is unlikely to contribute to the lower rate of CHD in women in Japan. Although a rate of oral contraceptive use in women in Japan is very low as compared with other developed countries 74 because it was introduced in 1999, 75 recent epidemiological studies show that use of oral contraceptives including past use is not associated with increased risk of CHD. 76
Lower prevalence of hysterectomy in Japan than in the United States 77 is unlikely to be a significant factor responsible for lower CHD rates in Japan. This is because hysterectomy is not the major determinant of CHD over traditional risk factors. We have recently reported from the Women's Health Initiative Observational Study 78 that the hazard ratio of hysterectomy for incident cardiovascular disease was 1.26 (95% CI: 1.16–1.36, p<0.001), which was attenuated after adjusting traditional CHD risk and other factors to 1.10 (95% CI: 1.00–1.21, p=0.042). The results suggest that a more adverse profile of CHD risk factors in women who had undergone hysterectomy compared with those who had not, rather than hysterectomy itself, is associated with CHD. Moreover, given the hazard ratio of 1.10 after adjusting for CHD and other risk factors, population-attributable risk 79 of hysterectomy for CHD is very low.
Evidence from migrant studies of Japanese and multiethnic studies in the United States does not support the hypothesis that the Japanese are genetically protected against CHD. Migrant studies of Japanese to the United States clearly show an increase in CHD and atherosclerotic burden in Japanese Americans as compared to Japanese in Japan. The NI-HON-SAN study, a cross-sectional study of cardiovascular disease and its risk factors in middle-aged Japanese men living in Japan, Hawaii, and California in the 1960s, has shown that CHD mortality is significantly higher in Japanese Americans than in Japan. 80 We have reported from a population-based study of Japanese and Japanese and white American men aged 40–49 years that levels of atherosclerosis assessed as coronary artery calcification and carotid IMT in Japanese Americans are higher or similar compared with U.S. whites. 12 Although CHD mortality in Japanese Americans is reported to be lower compared with white Americans, 81 –83 a more recent study has shown that CHD mortality is similar between young Japanese and white American women. Using U.S. Census data and California mortality data in 1990 and 2000, Palaniappan et al. reported age-, sex-, and ethnic-specific CHD mortality for six ethnic groups in California. 84 Although standardized mortality ratios (SMR) of CHD in women aged 45–64 years and 65–84 years are much lower in Japanese Americans than in white Americans, SMR of CHD in women aged 24–44 years is very similar between the two groups.
Given that the lower rates of CHD and atherosclerosis in Japan than in the United States are unlikely to be primarily due to differences in traditional risk or genetic factors, the most likely hypothesis is that there are common source exposures in the diet among Japanese in Japan, which accounts for their low CHD rates and atherosclerosis. The international collaborative study of macro- and micro-nutrients and blood pressure, which provides the most comprehensive dietary data in the United States and Japan 85 and other dietary studies 86 show that Japanese have markedly high intake of marine n-3 fatty acids (1,000 mg/day in Japan vs. 100 mg/day in the U.S.) 87 and isoflavones (25∼50 mg/day in Japan vs. <2 mg/day in the U.S.). 86
A large prospective cohort study in Japan supports the hypothesis that dietary intake of marine n-3 fatty acids and isoflavones are protective against CHD in Japan. The Japan Public Health Center-Based Study, a population-based cohort of individuals aged 40–59 years in Japan, following more than 40,000 individuals for about 10 years, reported that dietary intake of marine n-3 fatty acids had a significant inverse association with myocardial infarction after adjusting for history of hypertension and diabetes, medication for hyperlipidemia and other potential confounders. 88 This study also reported that that dietary intake of soy isoflavones had a significant inverse association with incidence of myocardial infarction in women even after adjusting for the above-mentioned factors. 89 Additionally, we have recently reported that high serum percentage of marine n-3 fatty acids significantly contributed to the difference in levels of atherosclerosis assessed as coronary artery calcification and carotid IMT between Japanese and whites. 12 It is unlikely that marine n-3 fatty acids or soy isoflavones exert their potential protective effects against CHD through total cholesterol, HDL-C, BP, or glucose homeostasis because recent systematic reviews show that effects of marine n-3 fatty acids or soy isoflavones on these factors are clinically insignificant. 90 –92 A large-scale randomized clinical trial (RCT) of marine n-3 fatty acids recently conducted in Japan demonstrated their clear benefit on CHD events, 93 although several recent RCTs failed to show their benefits. 94 –96 The discrepancy is at least due to the difference in dosage of marine n-3 fatty acids in RCT and background dietary intake of marine n-3 fatty acids as described above. No RCT of isoflavones on CHD has been reported, although many RCTs of isoflavones on CHD risk factors have been reported. 90,97,98
Limitations of this study warrant discussion. Mortality statistics are subject to misclassification without validation study. However, the fact that validated AMI incidence is much lower in Japan than in all the registries in other countries strongly indicate that low CHD mortality in Japan is not due to misclassification. Although we compared the trend in risk factors between Japan and the United States using primarily national survey data, these data may not be directly compared, because measurements are not strictly standardized between the countries. Factors other than those described in this paper that may be independently associated with CHD risk in each population, such as physical inactivity, psychosocial factors, and medical practice 55,99,100 could contribute to the difference in CHD rates in women between Japan and the Unites States.
In conclusion, we have shown that CHD mortality in women in Japan is much lower than in women in the United States. Differences in risk factors and their trends are unlikely to explain the difference in CHD rates in women in Japan and the United States. The results from migrant studies of the Japanese to the United States and international studies do not support the notion that Japanese are genetically protected against atherosclerosis and CHD. Investigating factors responsible for low CHD rates in women in Japan is important and may lead to new strategy for CHD prevention.
Footnotes
Disclosure Statement
No competing financial interests exist.