
Abstract
Introduction:
Vaginal childbirth may result in vaginal introital laxity, altered genital sensation during sexual intercourse, and reduced sexual satisfaction. We report the long-term effectiveness of a single nonsurgical procedure with radiofrequency (RF) energy for laxity at the vaginal introitus.
Materials and Methods:
Prospective single-arm study of 30 premenopausal women (21–52 year) with one 30-minute office procedure using RF applied to the vaginal introitus; 12-month outcome assessments included the linguistic validated Japanese versions of the Female Sexual Function Index (FSFI) and Female Sexual Distress Scale-Revised (FSDS-R) and the Vaginal Laxity and Sexual Satisfaction Questionnaires.
Results:
Sexual function improved significantly throughout 6 months (30 subjects); mean FSFI total score was 22.4±6.7 before treatment and then improved to mean 26.0±5.8 at month 6 (P=0.002), inclusive of improved scores in five of six FSFI domains except desire (P<0.001 –<0.01). In the 22 of 30 subjects remaining evaluable at 12 months, the mean was 26.0±5.2 (P=0.08). Distress related to sexual activity decreased significantly; baseline FSDS-R mean score of 15.8±11.7 improved to 9.8±8.0 at one month and was sustained throughout 12 months (P<0.001 – 0.002). Subjects reported decreased vaginal laxity within the first month after the procedure (P<0.001); responses peaked, and effectiveness was sustained through 12 months (P<0.001).
Conclusions:
A single nonsurgical office-based RF procedure for vaginal introital laxity achieved significant and sustainable 12-month effectiveness with respect to improved integrity at the vaginal introitus and improved sexual satisfaction. Treatment was well-tolerated with no adverse events.
Introduction
One of the most common physical consequences of vaginal deliveries is laxity of the vaginal introitus, a physical change that is rarely discussed between women and their healthcare professionals (HCP). 1 –3 Pregnancy and vaginal childbirth may result in trauma to the genito-pelvic floor musculature and vagina, with stretching of the vaginal introitus. Vaginal introital laxity is distinguished from prolapse, which involves the “falling” out of vaginal and other genito-pelvic structures. Prolapse can involve the bladder falling out, vaginal tissue bulging into and through the introitus, and/or the rectal tissue prolapsing into the vaginal area. Thus prolapse involves other structures, not just the vaginal introitus. A frequent consequence of this physical stretching is decreased genito-pelvic sensation during sexual intercourse, which may impact sexual quality of life. 4 –7 Other common patient complaints after a normal vaginal delivery are pelvic organ prolapse, stress urinary incontinence, bowel incontinence, altered sexual function, dyspareunia, and chronic pelvic pain. 5,7 –11 Changes in body image also impact sexual function and sexual health in the postpartum period. 6,7 In an international survey of urogynecologists, 83% of the 563 respondents described vaginal laxity as underreported by their patients, and the majority considered it a self-reported bothersome condition that impacts sexual function and relationships. 3 The incidence of this phenomenon remains undetermined, but HCP surveys have indicated that many practitioners do not have enough time to screen for potential sexual concerns in an office visit, are unsure of therapeutic opportunities, or have had unsatisfactory training to deal with female sexual dysfunction (FSD). 3,5
In this study we evaluated treatment with a low-dose, radiofrequency (RF) energy as a nonsurgical outpatient approach to the vaginal introitus tissue in women who experienced vaginal introital laxity after vaginal childbirth. The first human study explored the tolerability and safety of variable RF energy doses to discern the optimal energy level for this study. 12 Treatment with RF has shown long-term safety and effectiveness for stress urinary incontinence. 13,15 Low-dose RF continues to be used in other areas of medicine for the treatment of facial and neck skin laxity 16,17 as well as periorbital rhytides. 18
The primary aim of this study was to test the hypothesis that monopolar RF thermal therapy applied to the mucosal surface of the vaginal introitus can improve the integrity of the vaginal introitus and enhance sexual satisfaction, specifically determined by subject self-reports. Additional aims were to examine the long-term safety profile of the procedure and determine the magnitude of changes in sexual function and distress associated with sexual satisfaction assessed with both validated and patient-reported outcome (PRO) questionnaires.
Patients and Methods
This prospective, open label study was conducted between January and December 2011 at the Yokohama Motomachi Women's Clinic LUNA in Yokohoma, Japan. The protocol was reviewed and approved by the ethics committee (Medical Corporation LEADING GIRLS Women's Clinic LUNA). This single-site sample recruited women attending the gynecology and female urology clinic. They were given a survey about vaginal introital laxity; those that met the inclusion criteria were invited to receive a single treatment with RF energy to the vaginal introitus.
Subjects were required to be between the ages of 21 and 55 and premenopausal. They were to have had at least one full-term vaginal delivery (>36 weeks completed gestation), the last of which was at least 12 months prior to study enrollment. Participants were eligible if they self-reported a perception of vaginal introital laxity defined as “very loose,” “moderately loose,” or “slightly loose” on a seven-point Likert scale, the Vaginal Laxity Questionnaire (VLQ). Other major inclusion criteria included a normal Papanicolaou smear cytology and negative pregnancy test within 2 months prior to treatment; no breastfeeding for 3 months prior to enrollment; in a stable monogamous heterosexual relationship for at least 3 months prior to screening; willingness to participate in vaginal intercourse at least once per week; and be either surgically sterilized or willing to use an acceptable method of birth control at least one month prior to screening and/or will continue for duration of study. Exclusion criteria included: evidence of a thin recto-vaginal septum as assessed by the experienced clinical operator (approximately 1 cm in length or one finger's breadth); pelvic organ prolapse beyond the hymenal ring; an active sexually transmitted disease; acute or chronic vulvar pain syndrome; vulvar dystrophy; taking over-the-counter or prescription medications known to directly affect sexual function (e.g., antihypertensive, psychotropic, or chemotherapeutic agents); daily use of anti-inflammatory drugs that can affect collagen or healing (e.g., ibuprofen, aspirin, and steroids) or failure to fulfill a 30-day washout prior to treatment; clinically significant anxiety or depression; current treatment for hypoactive sexual desire disorder (HSDD) or orgasmic disorder; a current chronic skin condition involving the vulva; dyspareunia; irritable bowel syndrome; or a medical problem that might interfere with wound healing response as deemed by the investigator. All participants provided written informed consent before treatment. They were paid a nominal fee to cover travel expenses.
Screening evaluations included a detailed medical history, physical and pelvic examination, urine pregnancy test, patient demographics, and an obstetrics and gynecology history. PRO questionnaires were completed to characterize the subjects' sexual health and discern the outcomes following treatment. These instruments were administered before the treatment and at months 1, 3, 6, and 12 (post-treatment). PRO questionnaires were confidentially answered in the clinical setting; responses remained anonymous.
Primary outcome measures were determined with the Viveve System (VS) Questionnaire, with two Likert-type scale questions to assess the participant's perception of vaginal laxity (VLQ) and sexual satisfaction (SSQ) specifically from vaginal intercourse. The VLQ has seven-level ordered responses (very loose, moderately loose, slightly loose, neither loose nor tight, slightly tight, moderately tight, or very tight). The SSQ levels of response were none (no satisfaction), poor, fair, good, very good, or excellent. The questionnaire was administered prior to the RF treatment to assess current status; this is used as the baseline for comparison of therapeutic responses to treatment. The VS Questionnaire was translated into Japanese by a certified professional translation service and approved by the senior author (YS).
Additional outcome measures included the Female Sexual Function Index (FSFI) 19 and the Female Sexual Distress Scale Revised (FSDS-R). 20 We used the linguistic validated Japanese translations of the English versions of the FSFI and FSDS-R, both available from the MAPI Institute. 21 The FSFI is a 19-item questionnaire divided into six content domains: desire, arousal, lubrication, orgasm, satisfaction, and pain. The FSFI total score (sum of the six domains) as well as each domain score was analyzed. The FSFI has been found to be sensitive for detecting outcomes after treatment. 22 We defined a clinically significant change for a FSFI post-treatment total score of at least 2 points regardless of the participant's score at study entry. We based this on a similar calculation and methodology previously reported. 23,24 The FSDS measures sexually related personal distress in women. The questionnaire is scored by summing the responses to a list of 12 items asking the respondent to indicate how a problem or feeling caused distress in the last 30 days; responses are scaled from “never” (0) to “always” (4).
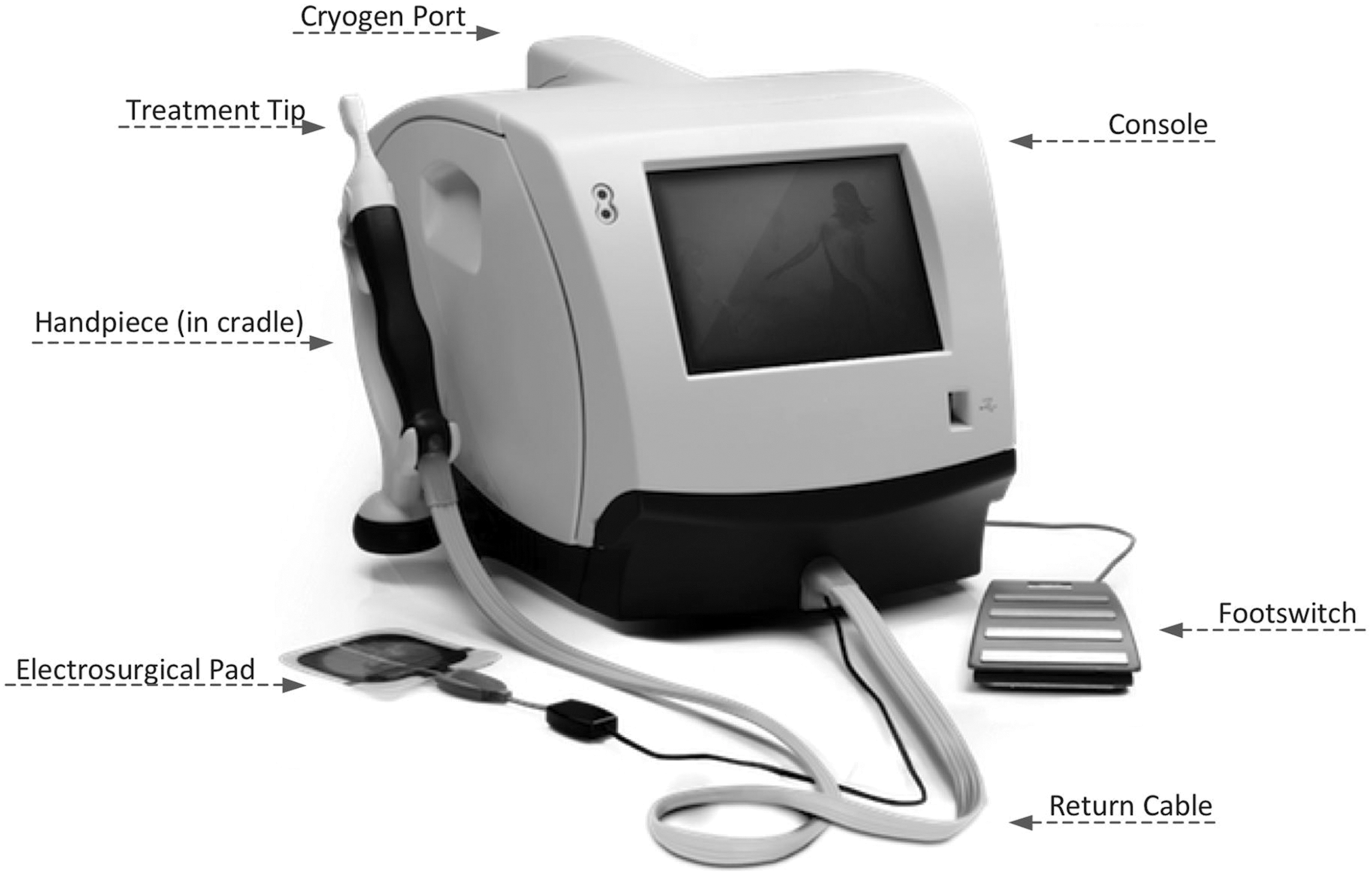
A single RF treatment was performed on each subject as an in-office procedure; no prior sedation or analgesics was required. The RF device (Viveve® Vaginal Laxity RF Therapy System, Viveve, Inc. Sunnyvale, California USA) provides a nonablative approach to creating heat within the submucosal layer of vaginal tissue while keeping the surface cooled. The system consists of a RF console, a cooling module, a horizontal handpiece, and a treatment tip (Fig. 1). It uses reverse thermal gradient RF technology. The monopolar RF pulse is generated to selectively heat a given volume of tissue beneath the surface, while the integrated cryogen is delivered to the inside of the treatment tip to cool and protect the surface tissue—the vaginal mucosa. RF energy pulses delivered at each dose are electronically monitored by the system to operate within the specifications for the RF device within the expected range of total pulses. Each of the three obstetricians/gynecologists operators who performed the procedures was trained by a board-certified U.S. gynecologist who had been involved in the prior U.S. study. They received on-site didactic learning and supervision. The procedure was standardized and performed in the same manner by the HCPs.
The in
Participants were treated in the dorsal lithotomy position; a return pad was attached on the subject's upper thigh. In brief, the procedures included a confirmatory pelvic examination to assess an adequate thickness of the recto-vaginal septum (approximately 1 cm or 1 finger's breadth, as measured by the operating clinician) and cleansing of the vagina, perineum, and perianal area using a nonalcohol-based cleanser. RF treatments were delivered at 90 J/cm2 , a dose previously determined to be safe and tolerable in a RF energy dose escalation study, as documented elsewhere. 12 A coupling fluid was used to ensure full contact. The active RF treatment tip was applied to the mucosal surface of the vaginal introitus behind the hymenal ring. Starting at the 1 o'clock position and moving circumferentially around the introitus, the treatment tip is passed over the entire area of 1 to 11 o'clock while avoiding the urethra. The area is treated with RF energy pulses at 0.5 cm overlapping intervals by moving the tip in a clockwise direction. The duration of each pulse is 7.5 seconds. The process is repeated until the entire area is treated five times each with 21 overlapping pulses or up to a maximum total of 105 pulses. The duration of the treatment averaged 26 minutes (range 20–30 minutes).
Subjects' experiences of discomfort or pain were documented during and after the procedure. Telephone interviews were conducted within 72 hours of the procedure. Follow-up clinic visits occurred at 10 days 1, 3, and 6 months post-procedure and included a pelvic examination, collection of adverse events if any, concomitant medication use and completion of the FSFI, FSDS-R, VLQ/SSQ, and the Global Response Assessment (GRA), responding to the question of “How are you now compared to before treatment?” Only questionnaires were provided to the participants for the 12-month post-procedure assessment.
Descriptive statistics were applied to obtain the means and frequencies of patient demographics. The Kolmogorov-Smirnov test was used to check for normality of distribution of data on the sexual function questionnaires (FSFI and FSDS-R) and the vaginal laxity and sexual satisfaction questionnaires (VLQ and SSQ). It was found that most of the data was not normally distributed. Thus the nonparametric test, the Wilcoxon signed rank test for paired samples, was used for comparative statistics of each time point evaluation score relative to pretreatment score. P<0.05 was designated as significant. Statistical analysis of data was performed using Microsoft Excel 2010 programs.
Results
Thirty premenopausal Japanese subjects each received one RF treatment. The mean age was 42.9 years (range 30–52 years). All had at least one full-term spontaneous vaginal delivery, and the average was 2.2 per patient; 40% had two and 30% had three or four vaginal deliveries. In the total of 65 full-term vaginal deliveries, only one delivery was forceps-assisted and 25 (38%) involved an episiotomy or laceration intervention. No subject had urinary or rectal symptoms or coexisting pelvic floor defects. Participants associated their laxity with a feeling of “vaginal emptiness,” as if water could flow in and out of the vaginal vault when bathing or swimming; they also described a loss of physical/sexual sensation during vaginal intercourse and decreased satisfaction with intercourse. The participants' descriptions of vaginal laxity and its consequences are similar to opinions collected from 421 women in an online survey. 2 At screening, 17 of 30 subjects reported a decrease in sexual satisfaction (on the SSQ survey); 13 of 30 reported no change or decrease in sexual satisfaction since their last vaginal delivery.
The RF procedure was well tolerated at 90 J/cm2; a total of 105 pulses were delivered to each participant. No treatment-related adverse events occurred during or after the treatment. All subjects reported a sensation of slight or moderate warmth during delivery of the RF pulses. The pain visual analog (VAS) scores averaged 1.5 out of a maximum of 10 during treatment, and seven subjects (23%) reported sporadic discomfort/pain with a VAS range of 3 to 5. One subject reported excessive but sporadic pain (VAS 7.7) but completed the treatment procedure without incident or requiring a topical anesthetic. When subjects were questioned at the 72-hour post-procedure evaluation, all reported a return to their normal routine activities of daily living. One case each of vaginal leukorrhea and lower abdominal pain occurred; both were reported as mild, and both resolved spontaneously within 10 days. Subjects resumed vaginal intercourse 10 days after treatment, and there were no reports of vaginal, vulvar, or abdominal pain. Pelvic examinations at day 10 and throughout the 6 months of follow-up were unremarkable.
Beginning at the first month after treatment and throughout 12 months, subjects reported improvements in vaginal laxity integrity (P<0.001) as reported on the VLQ (Fig. 2). The pretreatment mean score (±SEM) of 2.43±0.16 increased to 4.2±0.18 at 6 months; the 23 evaluable patients at month 12 scored 4.0±0.45. Regardless of the number of vaginal deliveries (ranging from 1 to 4), the RF procedure resulted in decreased vaginal laxity scores in most patients (Table 1).

Vaginal Laxity Questionnaire (VLQ) scores throughout 12 months of follow-up after a single RF procedure. The recall of vaginal tightness prior to vaginal deliveries is for point of reference of subjects' perceptions. P values, Wilcoxon signed rank test.
RF, radiofrequency.
Significant improvements in sexual satisfaction as reported on the SSQ were perceived at each follow-up assessment relative to pretreatment in 13 of the 17 (76.5%) subjects who expressed decreased satisfaction at study entry (Fig. 3A). The pretreatment mean score (±SEM) of 1.29±0.17 improved to 2.71±0.66 at month 6 (P<0.01). At 12 months, only 12 of the original 17 subjects remained evaluable for assessment of sexual satisfaction. The SSQ outcomes for 13 of 30 subjects who reported no change or decrease in sexual satisfaction since vaginal deliveries are reported separately in Fig. 3B. The pretreatment mean score of 2.42±0.18 remained similar and without any significant changes throughout the study.
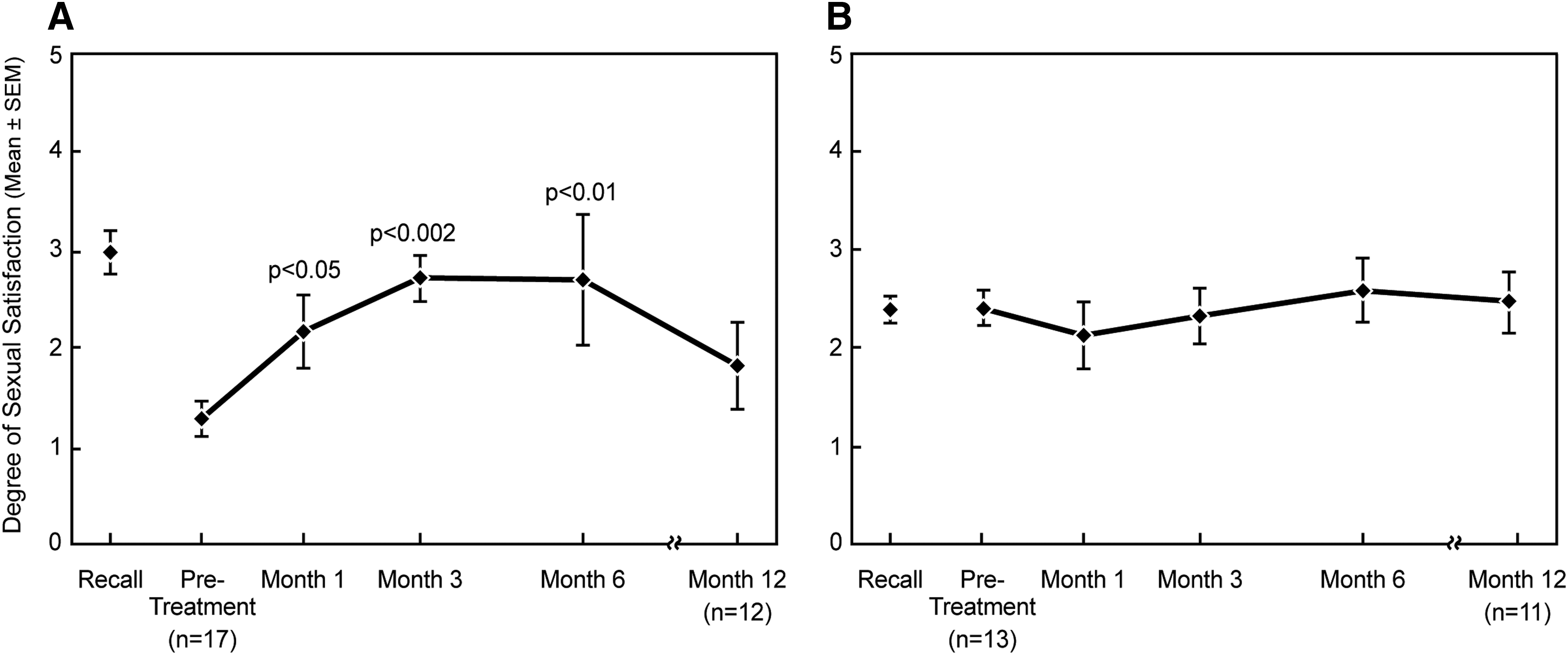
Sexual Satisfaction Questionnaire (SSQ) scores throughout 12 months of follow-up after a single RF procedure.
The FSFI and FSDS-R revealed no detrimental effects on any domains of sexual function related to the RF procedure. At screening, the individual subjects' FSFI total scores ranged from 3.6 to 31.2, mean (±SD) 22.4±6.7. After treatment, the total FSFI scores ranged from 19.0 to 33.4, mean 26.0±5.8 at month 6 (P=0.002) (Table 2); 19 of 30 (63%) subjects met the definition of experiencing a clinically significant change (≥2 point increase in total score) with a median increase of 3.6 points (range 2–22.7) compared with pretreatment. In 22 of 30 subjects evaluable at 12 months, the mean FSFI total score was 26.0±5.2 (P=0.08). Eleven of 22 (50%) were considered to have a clinically significant change, a median increase of 4.7 points (range 2.3–12.4). Distress related to sexual activity reported on the FSDS-R significantly decreased from a mean score of 15.8±11.7 at baseline to a mean of 9.0±8.0 at one month (P<0.001) and was sustained through 12 months (P<0.001–0.002).
Data are mean±SD.
P value determined by Wilcoxon signed rank test for paired samples, months 1, 3, 6, and 12 compared to pretreatment.
N, number of subjects.
Participants' impressions of changes in their decreased vaginal laxity/improved tautness as recorded on the GRA were characterized as “moderately or markedly improved” by 9 of 29 (33%) subjects at month 3, 12 of 29 (41%) at month 6, and 7 of 22 (32%) at month 12, compared to pretreatment and considered clinically significant. These GRA scores were associated with a median 2-point improvement (range 1–5) in level of vaginal laxity scores on the VLQ. The GRA for sexual satisfaction showed a similar pattern: “moderately or markedly improved” in 24% of subjects at month 3, 38% at month 6, and 27% at month 12. This level of improvement was associated with a median 2-point improvement (range 1–4) in level of sexual satisfaction on the SSQ. No participant reported a decrease in sexual satisfaction on the GRA or excessive changes in vaginal tightness to uncomfortable levels.
Discussion
This proof-of-concept study is the second report of nonablative RF thermal therapy for amelioration of vaginal laxity after vaginal childbirth. It reaffirms the tolerability and 12-month safety profile of this nonsurgical, minimally invasive RF treatment delivered at 90 J/cm2, when limited to the vaginal introitus. The treatment relies on the concept that carefully controlled RF energy can be used to heat deeper submucosal tissue in conjunction with concomitant cryogen cooling to prevent superficial heat injury. The therapeutic goal is to stimulate connective tissue activation with subsequent tissue revitalization. This process is similar to other medical procedures that are approved for the treatment of lax human skin 16,17 in which increased collagen formation appears to contribute to the mechanism of action. 25,26 It is hypothesized that a similar process of fibroblastic activation with new collagen formation after exposure to RF energy might occur in the vaginal introitus. Support for this putative mechanism of action of RF thermal therapy has been explored in a sheep vagina model (with histological similarity to the human vagina) evaluated with the same device and procedure to emulate treatment in human clinical studies. 27 Histological examination of sheep vaginal introitus biopsies after a single RF procedure supports an acceptable safety profile for continued clinical study and mechanism of action of the RF energy involving thermal fibroblast activation leading to collagen regeneration. This is consistent with a reparative pathway of changes to produce improved overall integrity of the genito-pelvic matrix tissues, which may subsequently enhance sexual responsiveness and satisfaction. Heating of the deeper fibro-connective tissue and epithelial protection with cryogen cooling appears safe and produced no mucosal ulceration, regional necrosis, or reparative scarring. A subsequent sheep histology study utilizing a sham treatment or cryogen cooling only without RF energy has provided confirmation of the effectiveness of RF energy (90 J/cm2). 35
The subjective improvements in vaginal integrity as well as increased sexual satisfaction were similar temporally and in magnitude in the Japanese participants in this study compared to non-Asians in a previous U.S. study. 12 This confirmatory data further supports the effectiveness of this procedure. 28
Female sexual dysfunction is common in otherwise healthy Japanese women. 29 –32 Noteworthy in this study is that 22 of 30 (63%) subjects had total FSFI scores ≤26.55 before the RF treatment; the mean was 20 (range 3.6–25.5). A score ≤26.55 is the suggested cut-off for designating women at risk for FSD as established in U.S. subjects. 33 However, the scores of 8 of these 22 subjects improved to levels without FSD after treatment; screening mean total score of 24 (range 19.9– 25.5) increased to a mean of 29.3 (range 27.7–32.3) at 6 months post-treatment. Also of interest are 21 of 30 (70%) subjects (not necessarily the same with lower FSFI scores) with FSDS-R scores ≥11 (mean of 21.6, range 11–43) at screening, a score reported to effectively discriminate between women with FSD and no FSD. 20 In contrast, the percentage of subjects with distress scores ≥11 fell from 70% to around 40% by months 1 and 3 after the RF procedure. Favorable sexual function is essential for a woman's satisfactory sexual life.
Although this study intentionally did not evaluate male sexual partner aspects of the sexual relationship with regard to partners' functionality, sexual interest and involvement in the women's participation in the study, the patients were required to have and be assessed for relationship stability. The importance of the woman herself complaining of changes at the vaginal introitus was paramount. The woman's willingness to come forward without coercion from an intimate partner or without relationship pressure was an important concept when assessing inclusion into the study.
The Global Study of Sexual Attitudes and Behaviors, a large multicountry survey of 27,500 participants aged 40 to 80 years, reported that only 9% of both women and men were asked about their sexual health during a routine office visit with a HCP. 31 The frequency of help-seeking for sexual problems in Asian countries is noted to be exceptionally low. 29 As vaginal introital laxity is a neglected topic of discussion especially after vaginal childbirth, this medical concern should be added to the list of biopsychosocial factors that affect sexual function. Healthcare professionals should question their patients concerning vaginal introital laxity. In addition, the impact or perception of laxity in Japanese women may be different than in U.S. women due to differences in socioculture-specific attitudes, family and partner relationships, and other ethnicity concerns or Japanese values.
The present study design has limitations that might impact the conclusions. The major limitation is the lack of a sham treatment arm for comparison of patient outcomes attributable to the effects of the RF energy. A clinical study with a sham treatment control arm will be important to examine a potential placebo response after RF treatment of vaginal introital laxity. Evidence from animal model studies indicates that controls could include a sham procedure without heating or with cryogen cooling alone.
A linguistically validated Japanese translation of the U.S. version of the FSFI was utilized in this study, which preceded the recent publication of a validated FSFI for Japan. 34 The Japanese version evaluates the previous three months of sexual function rather than one month as in the U.S. version and may result in different outcomes. It is not possible to determine the duration of effectiveness of the improvements at the vaginal introitus.
Several potential methods to objectively quantify vaginal introital laxity, including caliper measurements, a balloon device (such as a barostat for measuring esophageal strictures), and comparative photos, have been evaluated, but all have been found to be unreliable for a variety of medical and anatomical reasons. There are no validated instruments currently available for reliably measuring the vaginal introitus with a high index of reproducibility. Therefore, at the present time the assessment of laxity cannot be objectively defined. Subjective determinations of outcomes may be biased; however, PROs are rapidly becoming the gold standard for primary endpoints for clinical studies evaluating treatments for female sexual problems. Subjective evaluation has been the standard for determining the success of RF-induced facial skin laxity. 17,18
This single-arm study involved a small sample size as is appropriate for a proof-of-concept study. A larger randomized, controlled, multicenter study will be important to examine a potential placebo effect after RF treatment of vaginal introital laxity.
Conclusions
This study confirms that a nonsurgical, nonablative RF treatment is a well-tolerated and safe procedure shown to produce subjective improvements in vaginal introital laxity and improved sexual satisfaction in women after vaginal deliveries. The profile of effectiveness in subjects from Japan is in agreement with earlier observations in a cohort of U.S. patients with vaginal laxity; this is indicative of a cross-cultural similarity of perceptions of this medical concern and impact on sexual health after vaginal childbirth.
Footnotes
Acknowledgments
This clinical study was supported by Viveve, Inc., Sunnyvale, California, USA.
Technical writing support was provided by Elaine K. Orenberg, PhD.
Author Disclosure Statement
Drs. Kingsberg and Krychman are members of the Scientific Advisory Board, Viveve Inc. The other authors have no existing competing financial interests.