
Abstract
Introduction:
Postnatal depression has a serious impact on new mothers and their children and families. Risk factors identified include a history of depression, multiparity, and young age. The study aimed to investigate factors associated with experiencing antenatal depression and developing subsequent postnatal depression.
Methods:
The study utilized survey data from 5332 women about their experience and well-being during pregnancy, in labor, and postnatally up to 3 months. Prespecified sociodemographic and clinical variables were tabulated against the incidence of antenatal depression and postnatal depression. Binary logistic regression was used to estimate the effects of the principal underlying variables.
Results:
Risk factors for antenatal depression were multiparity, black and minority ethnic (BME) status, physical or mental health problems, living in a deprived area, and unplanned pregnancy. Different factors for postnatal depression were evident among women who had experienced antenatal depression: multiparity and BME status were protective, whereas being left alone in labor and experiencing poor postnatal health increased the risk of postnatal depression.
Conclusion:
This study confirms previous research on risk factors for antenatal depression and stresses the importance of continuous support in labor and vigilance in the postnatal period regarding the potential ill effects of continuing postnatal health problems.
Introduction
Antenatal depression is recognized as a major risk factor for postnatal depression. 1 –3 Rates of postnatal depression are reported at between 9% and 15%, 4 and for antenatal depression at between 7% and 22% depending on severity and the timing of data collection. 5 –8 Risk factors for antenatal depression include young maternal age, less than 12 years of education, chronic medical conditions, Asian and African American ethnicity, 8 single parenthood, and having an unwanted pregnancy. 6 Risk factors for postnatal depression appear to be similar, 3 being associated with a history of depression, antenatal depression, antenatal anxiety, stressful life events, negative cognitive attributional style, low self-esteem, low social support, and low income. 9 Other suggested risk factors for postnatal depression include young age, lower levels of education, a history of miscarriage and pregnancy termination, and a history of childhood sexual abuse. 10
Many studies of perinatal depression utilize relatively small numbers of women, often associated with specific hospitals providing obstetric care and community medical practices and in areas that differ in terms of the degree of disadvantage. 8,11 –13 This may account for some of the variation in the proportions of women being identified as experiencing depression in the antenatal and postnatal periods.
Babies of women suffering from postnatal depression have been found to be more likely to experience the consequences of poor attachment and impaired interactions, leading to impaired cognitive outcomes, 14,15 with longer term outcomes being of concern if the postnatal depression is severe or chronic. 10 However, not all studies report similar findings. With a recent large, population-based sample of women, neither maternal history of depressive disorder nor maternal depressive symptoms either during pregnancy or postnatally were found to be related to later mother–infant attachment. 16
While associations have been found between antenatal depression and its occurrence in the postpartum period, 4,13 it is not clear if there are mitigating factors that can influence whether a woman who experiences antenatal depression goes on to have postnatal depression. Thus, the aim of this study was, first, to investigate some of the factors associated with antenatal depression in this population, and second, for those women who had antenatal depression, to determine which factors appear to influence depression being experienced subsequently in the postnatal period.
Methods
This study used analysis of secondary data from a recent survey of new mothers. A random sample of 10,000 women aged 16 years and over who had their baby in a 2-week period in England were selected by the Office for National Statistics (ONS) from birth registrations. Mothers of babies that had died and those less than 16 years at the time of the baby's birth were excluded from the sample. Women were sent a questionnaire, invitation letter, information leaflet, and an information sheet in a range of languages when the babies were 3 months of age in January 2010. All were offered the option of completing the survey online using individual log-ins. Tailored reminders were sent to those who had not responded: initially a letter 2 weeks after the first mailing, a further questionnaire after 4 weeks, and a further letter 4 weeks later. 17
A range of questions about women's health, clinical care, and perception of care during the antenatal, intrapartum, and postnatal periods care were asked, including whether the woman had experienced depression antenatally or postnatally. For the purposes of this analysis, which focused on outcomes at 3 months, “blues” was combined with postnatal depression since blues do not generally continue to 3 months. A list of variables indicated by the literature to be associated with antenatal or postnatal depression was constructed and grouped into sociodemographic and clinical variables (see Appendix 1). Two independent sets of analyses were done, the first relating to antenatal depression, the second relating to postnatal depression. In the first set of analyses, sociodemographic variables were tabulated against reported antenatal depression using chi-square statistics and a significance level set at p<0.01 (due to the size of the dataset and the number of variables). These variables were then entered into a multivariate binary logistic regression model, with a significance level set at p<0.05, to ascertain the key variables at this stage. Antenatal clinical variables were also tabulated against antenatal depression in the same way. The second set of analyses concentrated solely on those women who had experienced antenatal depression. Sociodemographic and clinical care variables were tabulated against postnatal depression in univariate analyses followed by multivariate binary logistic regression of significant variables to explore associations with postnatal depression. In the multivariate models, analyses were adjusted for sociodemographic variables and also those variables that were significant in the univariate analyses. Significance levels for these analyses were set at p<0.05 due to the smaller numbers. Analyses were carried out using SPSSX version 17.
Results
The response rate to the survey was 55.1%, with 5332 women providing usable responses, 8% of which were on-line returns. Summary demographic data on respondents and nonrespondents were provided by ONS. The respondents were largely representative of the whole population; however, as with most surveys of this kind, younger women, those living in more disadvantaged areas, women who were not married, those from BME groups, and those born outside the United Kingdom were less likely to respond. 17 –19 Nevertheless 22% of respondents were born outside the United Kingdom, 14% came from BME groups, and 12% were single parents.
A total of 475 women (9.6%) responded positively to the question in the antenatal section about depression during their pregnancy: “Did you experience depression or seek help for depression from a midwife or a doctor?” Of these women only half (4.5%) reported seeking help for depression at this time. Of those women reporting depression during pregnancy, just over a third (35%) went on to report having postnatal depression at 10 days, 25% at 1 month, and 21% at 3 months (Fig. 1). This is compared to 5% at each time point in women who were not depressed antenatally. Outcomes were also poorer in women with antenatal depression in terms of general health and well-being. When asked how they felt physically in the first few days after the birth and, again, at 3 months after the birth, women who had experienced antenatal depression rated their health as significantly worse than those who were not depressed antenatally. For example, 10% of women in the antenatally depressed group reporting feeling “very well” in the first few days, compared to 18% among other respondents. At 3 months the difference was greater with the comparable proportions being 10% and 28%, respectively.
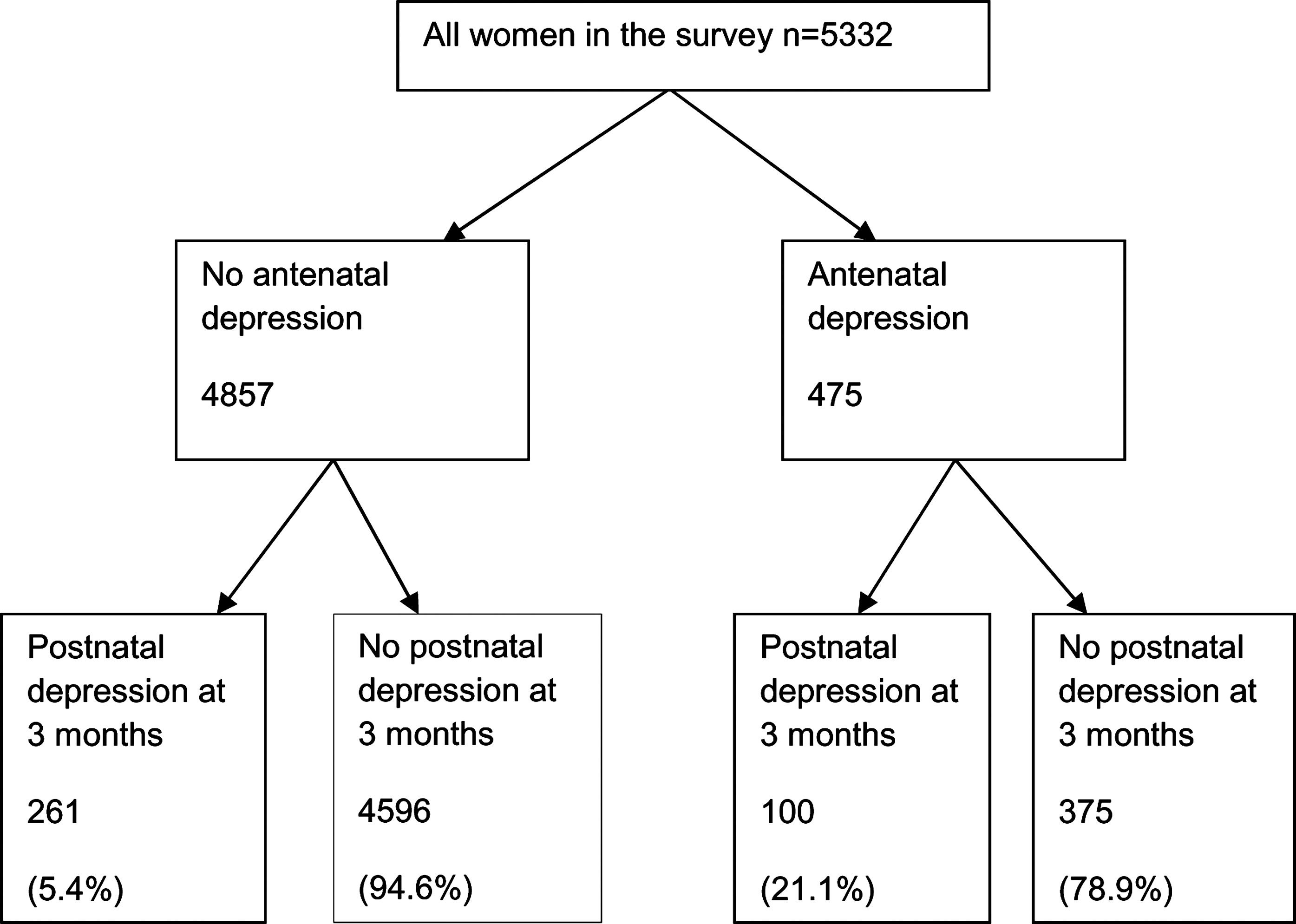
Rates of antenatal and postnatal depression at 3 months in survey respondents.
Based on the literature on maternal mental health and well-being during pregnancy and postnatally, 1 –8 a range of variables was selected for analysis (see Appendix 1 for list). Univariate analysis indicated that some sociodemographic, possibly predictive, factors associated with antenatal depression were multiparity; young age; young age on completing full-time education or still being in full-time education; being from a BME group (especially black or black British); being a single parent; living in a very deprived area; having long-term physical or, more particularly, mental health problems, especially if these limited day-to-day activities; and having an unplanned, unwanted pregnancy (Table 1). Women with antenatal depression were also more likely to experience other antenatal health problems; for example, repeated vomiting (42% compared with 20%), carpel tunnel syndrome (21% compared with 11%), and stress incontinence (26% compared with 9%; data not shown).
AN, antenatal; IMD, index of multiple deprivation.
There is a degree of overlap between the factors listed as associated with reporting antenatal depression, and therefore binary logistic regression was used to determine the principal underlying variables. The results (Table 2) suggest that women from BME groups and more deprived areas are at increased risk of antenatal depression, as are multiparous women, those with long-term mental health problems or learning disabilities, and women with unplanned, unwanted pregnancies.
p<0.05. Adjusted for age, age on leaving full-time education, single parenthood, and long-term physical problem/disability.
BME, Black and Minority Ethnic.
In terms of clinical factors and service use, women who experienced antenatal depression were generally seen significantly later in pregnancy, were less likely to have a dating or anomaly scan, were less likely to be offered or attend National Health Service (NHS) antenatal classes; screening for Down's syndrome was more likely to be by nuchal scan or nuchal scan plus a blood test, but the women were also less likely to recall being offered the test. Women reporting antenatal depression were nearly twice as likely to have experienced an overnight stay in hospital during the pregnancy and were also more than twice as likely to have long-term health problems affecting this or previous pregnancies (Table 3).
NHS, National Health Service.
In terms of communication with staff in the antenatal period, women having antenatal depression were significantly more likely to feel that during pregnancy one or more midwives did not talk to them so they could understand and did not treat them with respect or kindness. The same was true in terms of communication with medical staff. These results are also summarized in Table 3.
In the subgroup of women who had experienced antenatal depression, specific sociodemographic, clinical, and care factors were significantly associated with also experiencing postnatal depression three months after the birth. The results of these univariate analyses are shown in Tables 4 and 5. In contrast to the previous results, multiparous women and those from BME groups were at reduced risk of postnatal depression. However, those with long-term mental health problems or learning disabilities, poor physical health postnatally, or dissatisfaction with postnatal care generally and those who experienced poor interactions with some midwifery and medical staff reported higher rates of depression at 3 months. Mode of delivery was not associated with postnatal depression.
PN, postnatal.
GP, general practitioner/family doctor.
The factors that were significant in the univariate analyses were then used as independent variables in a binary logistic regression with depression at 3 months postpartum as the dependent variable. This analysis was also limited to women who had experienced antenatal depression. As shown in Table 6, the most important factors influencing whether women who reported depression during the antenatal period also had postnatal depression at 3 months after giving birth appeared to be related to having long-term mental health problems or learning disabilities, being left alone and worried in labor or shortly after the birth, having postnatal health problems at 1 month (but not at 10 days), and women feeling physically unwell at the time of the survey. Surprisingly, those women who were depressed in both the antenatal and postnatal periods, reported greater satisfaction with postnatal care overall.
*p<0.05. Adjusted for maternal age, parity, IMD, single parenthood, BME, and other variables significant in the univariate analysis: antenatal anxiety, antenatal and intrapartum staff interaction, perception of length of stay, antenatal classes including partner attendance, availability of baby cafe and baby clinic at GP, help at 6 weeks in settling baby, with baby's crying, feeding baby, and infant feeding at 3 months.
Discussion
The risk factors for antenatal depression found in this study are consistent with those reported in other studies of antenatal depression: ethnicity, social disadvantage, multiparity, long-term mental health problems or learning disabilities, and an unwanted pregnancy. 2,6,8,10,20 The rate based on self-report is within the range of what has been variously reported, including data from recent large population-based studies 21,22 in which rates of antenatal depression of 9% and 10% were described.
Service use for women with antenatal depression was significantly less than for other women: they booked later and consequently had fewer antenatal checks, were less likely to have ultrasound scans, and they were less likely to recall being offered screening for Down's syndrome. Depressed women suffered more antenatal morbidity having more overnight hospital admissions during pregnancy and more long-term health problems. This is consistent with other studies in this area, emphasizing the value of screening for and monitoring maternal health at this time. 8,23,24 Quality of staff interaction was also significant. Women who felt they were spoken to so that they could understand and treated with respect and kindness antenatally by both midwives and doctors were less likely to report suffering from antenatal depression. It may also be that women who were also depressed postnatally have more negative perceptions of staff interactions than nondepressed women. However, that this group were in fact, more likely to report being satisfied or very satisfied with their postnatal care would argue against this interpretation. As has been pointed out, 7 depression may contribute to slower recovery after childbirth, but it is also likely that physical health problems contribute to depression at both time points.
In a relatively small-scale study of couples during the transition to parenthood, the proportion of women with antenatal depression, who then at 3 months after the birth reported postnatal depression was 21%. 25 However, studies that have followed women further, to the end of the first year and beyond, have described something of a U-shaped pattern over time, with some women initially adapting to their early parenting role but then experiencing distress later, perhaps when combining parenting with return to work and coping with greater pressures in the couple relationship. 21
For those women who were depressed antenatally, risk factors for postnatal depression were different: being multiparous and from a BME group appeared to be protective. However, being left alone and worried in labor or shortly after the birth, and poor physical health postnatally were associated with higher rates of postnatal depression. Mode of delivery was not associated with postnatal depression in this group of women, which is consistent with some studies in this area 26 but not others. 27 That women at higher risk of postnatal depression, having been depressed antenatally, were more satisfied with postnatal care may indicate that staff perceived their vulnerability and acted accordingly. The only variable that was significantly associated with both antenatal and postnatal depression was long-term mental health problems or learning disabilities. This is not surprising because depression constitutes a significant component of mental health problems generally, and a history of depression is a significant risk factor for perinatal depression. 28
A strength of this study is that it was based on a large population-based national survey with more than 5000 respondents. Some studies have shown that women may be reluctant to discuss their own health at postnatal or later checks during the early months after childbirth, 29 and poor disclosure of emotional problems means that medical or hospital-based records may well underrepresent the extent of maternal morbidity. Thus survey responses, which women make anonymously, may better reflect their health and well-being. 30
A limitation of this study is that the response rate to the survey was 55%. However, this is similar to that found with other national or state surveys, 31 and respondents and nonrespondents were similar except that younger, single women, those born outside the United Kingdom, and women living in the most deprived areas were underrepresented. Despite being underrepresented, significant numbers of these women responded to the survey. A further limitation was that the occurrence of antenatal and postnatal depression was based on women's report without independent verification, and only some women reported seeking help for this. The survey responses may have also been affected by recall bias if women suffering from postnatal depression at the time of completing the questionnaire were more likely to recall problems than women who were feeling well. However, the reported rates are similar to those in the literature and the responses, reflecting perceptions of services and care by this group, were not uniform or universally critical.
This study illustrates different possible associations and influences on women with antenatal depression, and factors associated with subsequent postnatal depression. Long-term mental health problems, high-risk pregnancy, and not recovering well after childbirth are clearly important factors, 32 but the quality of postnatal care may also be an important mitigating influence. Further research could focus on anxiety and depression and the factors associated with comorbidity both before and following childbirth. Clinical implications of the study largely center around health care professionals working with women being aware that depression in the antenatal period may signal the possibility of postnatal depression occurring after the birth. The National Institute for Health and Clinical Excellence (NICE) clinical management and service guidance for women with mental health problems in pregnancy and postnatally recommends the development of a trusting relationship with the woman and, if appropriate, her family, and being sensitive to shame and stigma that can occur in relation to mental illness. 33 Midwives and health visitors helping women in the postnatal period should be aware of the higher rates of depression in women with significant and continuing postnatal health problems. Sensitivity to vulnerable women's support needs and health during pregnancy, in labor and in the months after birth is also likely to contribute to the kind of individualized care which women themselves recognize and value.
Current knowledge on this subject: - Antenatal depression is a major risk factor for postnatal depression - Babies of women suffering from postnatal depression are at risk of poor attachment - Risk factors for antenatal and postnatal depression include socioeconomic and clinical factors
What this study adds: - Risk factors for postnatal depression among women who have experienced antenatal depression differ from risk factors for postnatal depression generally - The only factor common to both antenatal and postnatal depression was long-term mental health problems or learning disability - Interactions with staff, particularly in the postnatal period, may be an important ameliorating factor
Footnotes
Acknowledgments
This article reports on an independent study. The views expressed are not necessarily those of the Department of Health. This study was funded by the Policy Research Program in the Department of Health. The original survey was funded by the Department of Health in 2009-10 (London, United Kingdom).
Author Disclosure Statement
Neither of the authors has any conflict of interest.
Appendix 1. Variables Considered in the Analysis
Sociodemographic variables: Parity, age, ethnicity, age on completing full-time education, index of multiple deprivation (IMD), pregnancy planned, reaction to pregnancy, single parent, father and partner engagement, multiple birth, gestation at birth, birthweight
Clinical care variables: Gestation at booking, number, location and health professional seen for antenatal checks, tests and scans, overnight hospital stays, having midwife contact details, antenatal problems, long term health problems, attending antenatal classes, worries about labor and birth, induction of labor, pain relief in labor, place of birth, type of birth, left alone during or after the birth, infant feeding, admission to neonatal care, care at home after the birth, postnatal health and well-being and communication with staff in the antenatal, intrapartum and postnatal periods.