
Abstract
Background:
This study was conducted to evaluate the therapeutic efficacy of a device designed to deliver high-frequency vibratory stimulation through direct intravaginal tampon application (VIPON) compared with a low-dose over-the-counter pharmacologic treatment of dysmenorrhea.
Methods:
A randomized, open-label, prospective study comparing the investigational device to an oral self-administration of the over-the-counter dose of 200–400 mg of ibuprofen with the onset of menstrual discomfort was conducted at two academic medical centers in the Midwest region of the United States. Women age 18 and older with self-reported dysmenorrhea were treated with either VIPON or a single dose of 200–400 mg of ibuprofen, randomized for each of the next four menstrual cycles, and pain reduction from baseline was measured according to the Melzack-McGill pain scale.
Results:
Overall, both ibuprofen and VIPON have significant effects on pain reduction according to the Melzack-McGill pain scale. However, the VIPON group achieved statistically significant greater, and more rapid, pain relief at every time point when compared with the ibuprofen.
Conclusion:
VIPON tampon is a viable, nonpharmacologic option to traditional low-dose over-the-counter pharmacologic therapies for menstrual pain management with more rapid onset of action.
Introduction
Dysmenorrhea, or functional cyclic pain directly related to menstruation, is one of the most common gynecologic complaints. At least 50% of all menstruating women experience appreciable pain some time during their menstruation, and an estimated 600 million work hours are lost annually to this condition, with an average loss of time of two or more workdays per year per female employee. 1 The most widely accepted explanation of the etiology of dysmenorrhea is overproduction of prostaglandins in the endometrium, causing myometrial contractions and vasoconstriction leading to the perception of pain.
Nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to be highly effective in the treatment of dysmenorrhea. 2 Women most often self-treat menstrual pain with over-the-counter (OTC) analgesics such as acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs) or other self-care modalities in the absence of—or prior to—seeking medical advice. 3 Accelerated prescription-strength dosing of NSAIDs and/or oral contraceptives are commonly used by medical professionals when severe symptoms are present. 4
Several nontraditional and nonpharmacologic treatments for dysmenorrhea have also been proposed, but most are not well studied. Massage, topical continuous low-level heat, rest and/or exercise, nutritional supplements (e.g., thiamine, ginger, vitamin E, omega-3 fatty acids, magnesium), acupuncture, acupressure, and transcutaneous electrical nerve stimulation (TENS) units have all been suggested to be beneficial in pain relief. 5,6 The TENS unit has demonstrated equal efficacy and safety compared with NSAIDs in the treatment of dysmenorrhea but requires external placement that may be visible and possibly hinder mobility. 7 –10 Vibratory energy has been favorably compared to TENS technology for rapid and effective relief for other types of pain. 11 Although the exact mechanism of action of vibratory energy in pain relief is not known, it is believed that physical vibration, similar to TENS, relieves pain in a manner consistent with the gate control theory of pain management. 12 This theory postulates that vibratory stimulation excites A-beta nerve fibers, which inhibit A-delta fiber signals, minimizing pain signals relayed to the brain. 13 We hypothesized that vibratory energy delivered through direct intravaginal application within a tampon (VIPON) would be as effective as the standard over-the-counter dosage of ibuprofen in reducing symptoms of dysmenorrhea, providing a discrete and nonpharmacologic pain relief option. Secondarily, we hypothesized that the direct application of this device would produce pain relief more quickly than 200–400 mg oral ibuprofen.
Materials and Methods
VIPON study device
The Food and Drug Administration (FDA)-approved VIPON includes a cotton tampon, an applicator for insertion of the tampon into the vagina, a vibratory stimulation micro-unit, and a battery (see Fig. 1). The micro-unit is embedded within the tampon and is covered by cotton, which prevents contact with vaginal mucosa. The 1.5-V (0.246 W) battery is external to the body and is sealed inside a button housing that turns it on or off.

Photograph of VIPON study device unit.
Methodology
This randomized, open-label, prospective study of over-the-counter methods for relief of the initial symptoms of menstrual pain was conducted at two academic medical centers in the Midwest following approval by the Institutional Review Boards at both study sites. The study was registered with the
SD, standard deviation.
At the onset of dysmenorrhea, subjects were instructed to complete the numerical Pain and Symptom Relief Assessment Form provided in the patient diary based on the modified Melzack-McGill pain response scale. 14 Pain was assessed on a numeric pain intensity scale from 0 to 10 where 0=no pain and 10=worst pain (see Fig. 2). 14, 15 Subjects then completed the pain questionnaire at 15 minutes, 30 minutes, 1 hour, and 2 hours post treatment. Study visits were conducted at enrollment, mid-visit, and at the conclusion of the study. No follow-up assessments were performed upon study completion.
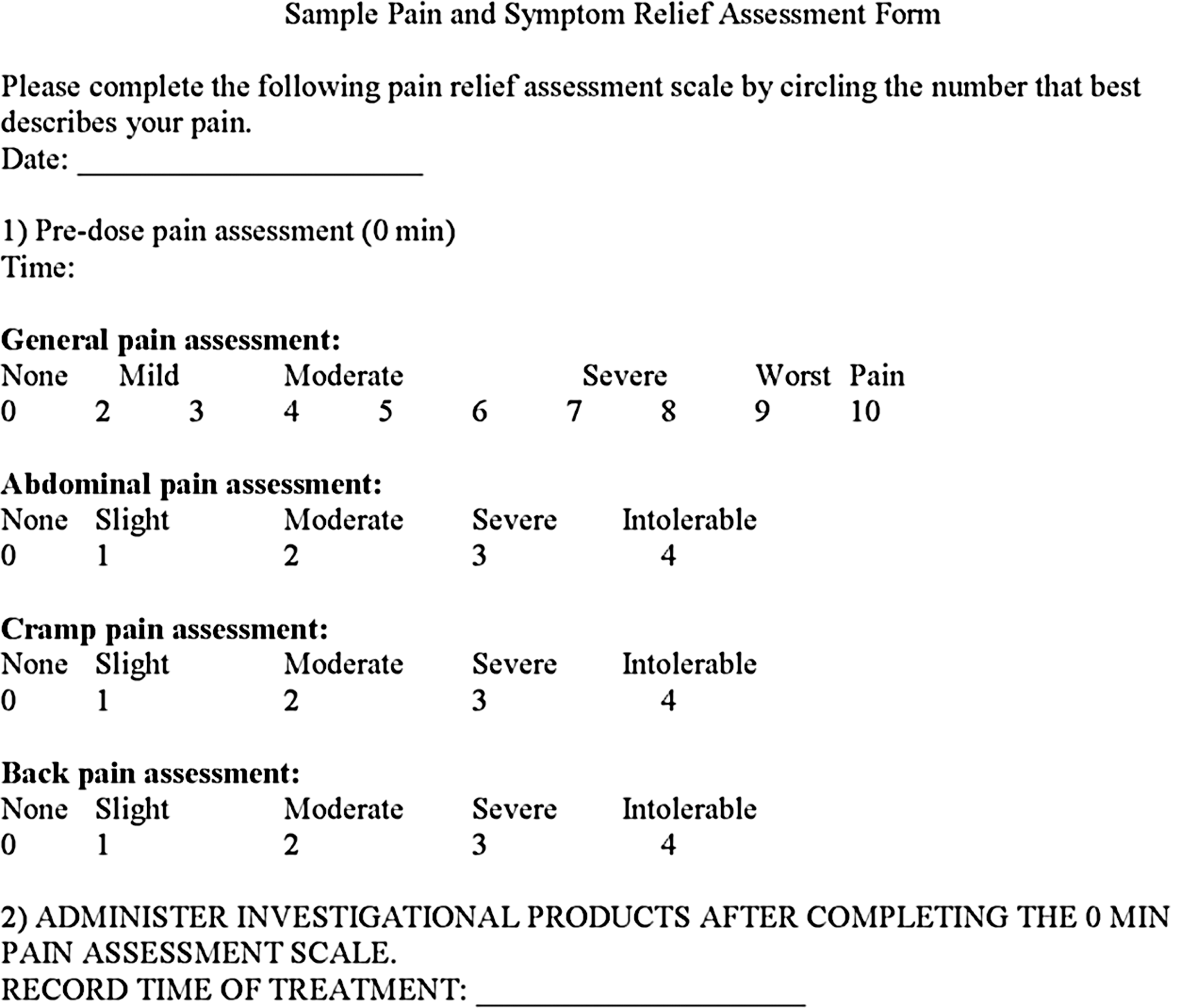
Pain and Symptom Relief Assessment Form.
A hierarchical linear mixed model that included both fixed and random effects was conducted to account for the repeated measurements from each individual for each menstrual cycle. Changes in the value of outcome variables from baseline to each post-treatment time point were calculated and treated as dependent variables in the linear mixed model—greater change defined greater pain reduction from the treatment. Estimated pain reduction at each time point for the ibuprofen and VIPON groups were estimated and tested for significance while individual-specific variables were included as random effects. This analytic strategy provided a modeling advantage by accounting for the individual effect in the analysis, resulting in more accurate estimates for the study. All tests were two-sided, and statistical analyses were performed using SAS 9.2 (SAS institute Inc.).
Results
Data from 375 cycles (VIPON, n=183; ibuprofen, n=192) in 102 patients were included in the analysis. An additional 13 patients were enrolled but not included in analysis because of incomplete cycle data. Of the 192 ibuprofen cycles, 95% took the higher 400 mg dose.
For the Melzack-McGill Pain response, pain reduction in the ibuprofen group was not statistically significant at 15 minutes post treatment (a reduction of 0.20) (Fig. 3). The effect of ibuprofen increased with time, and it reached a reduction of 2.55 at 2 hours post treatment. The effect of VIPON was significantly better than ibuprofen by 0.76 at 15 minutes, 0.84 at 30 minutes, and 0.51 at 1 hour (p<0.01, p<0.01, and p<0.01, respectively). There was no significant difference in pain reduction between VIPON and ibuprofen after 2 hours of treatment (reductions of 2.86 and 2.55 respectively; p=0.09). Overall, both ibuprofen and VIPON had clinically significant effects on pain reduction according to the Melzack-McGill pain scale. However, the VIPON group had greater pain relief at every time point up to 2 hours when compared with the ibuprofen group, and the pain relief was statistically significantly faster than ibuprofen.
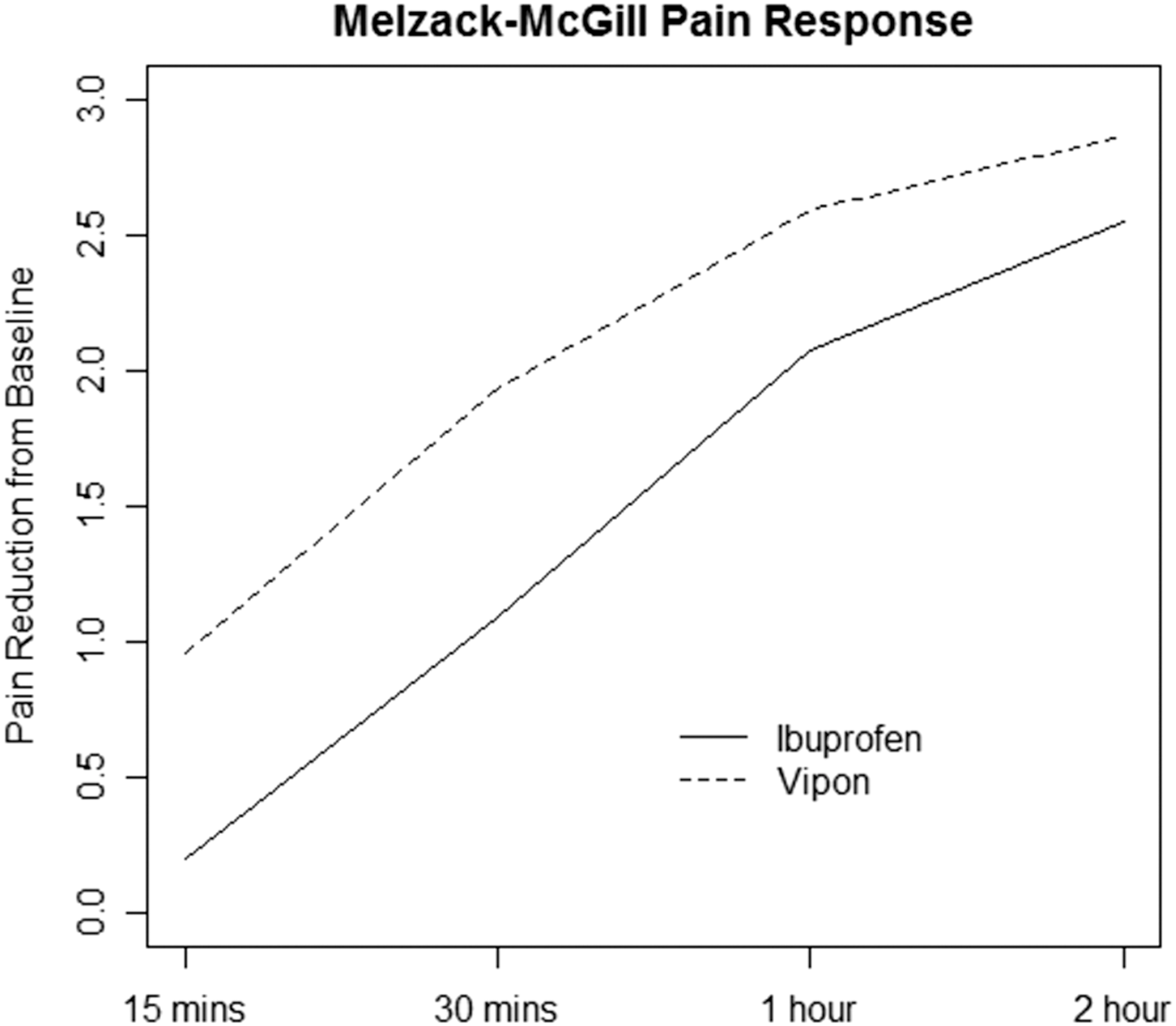
Estimated pain reduction from baseline at 15 minutes, 30 minutes, 1 hour, and 2 hours post treatment in the VIPON and ibuprofen groups.
Discussion
Dysmenorrhea remains a significant problem leading to suffering and functional disability for a large proportion of reproductive age women. While several homeopathic and pharmacologic point-of-pain remedies are recommended to improve functional capacity and decrease pain, many women still desire a discrete, nonpharmacologic, non–medically supervised treatment. This investigation proved that VIPON provided effective relief of dysmenorrhea equal to OTC doses of ibuprofen with a more rapid onset of action. In addition, the delivery method housed within a disposable tampon allows women to avoid the use of a parenteral medication with possible side effects and have an effective, discrete, and well-tolerated novel alternative for over-the-counter treatment of dysmenorrhea.
This preliminary study focused on initial pain relief with the recommended over-the-counter dosing of ibuprofen. The effect of longer use, reapplication of the device, or its use in combination with other medication was not addressed. Efficacy was only assessed to 2 hours post-treatment and over a limited number of treatment cycles. It is unknown if the treatment effects were sustained over 4 hours of recommended over-the-counter ibuprofen administration or across the known variations in pain severity across menstrual cycles. No readministration of either VIPON or OTC strength ibuprofen was done. It is unknown if replacement of the VIPON tampon would sustain or prolong the desired therapeutic effect. Finally, higher dosing of ibuprofen was not addressed, as this study focused on two over-the-counter dosages that required no medical supervision. It is unknown if common (higher) medical prescription dosing of ibuprofen would yield similar or superior results as compared to over-the-counter medication.
Conclusions
Optimally, clinicians should be able to offer women with dysmenorrhea a range of methods to alleviate discomfort. Our findings indicate that the VIPON tampon is a viable, effective, nonpharmacologic option for initial menstrual pain management with rapid onset of action. Further studies should be conducted to address higher doses of ibuprofen, the device reapplication efficacy beyond 2 hours, and the effect of the VIPON used in conjunction with other modalities including pharmacotherapies. It is hypothesized that because VIPON's mechanism of action is distinct from pharmacologic treatments, it should be able to be safely combined with any of the other treatments for dysmenorrhea. The additive effects of this treatment combined with pharmacologic therapy is unknown but may provide additional beneficial effects. The findings of this study do suggest that providers should incorporate a discussion of this new device into the broader discussion of a wide variety of over-the-counter treatment options available for dysmenorrhea.
Footnotes
Acknowledgments
Funding for this study was provided by Another Way Products LLC. (Note: The production version of the VIPON is presently being marketed and sold OTC in Europe under the trademarked name Tamia.)
Disclosure Statement
No competing financial interests exist.