
Abstract
Background:
Examination of maternal experiences of intimate partner violence (IPV) and depression as risk factors for food insecurity can provide a more nuanced understanding of the role that the family environment and women's health plays in the lives of families with young children that experience food insecurity. We investigated the longitudinal association between mothers' experiences of IPV and household food insecurity, and whether maternal depression mediated the relationship.
Methods:
IPV, depression, and food insecurity were assessed among 1,690 socioeconomically disadvantaged mothers of young children who participated in the Fragile Families and Child Wellbeing study. Longitudinal multivariate logistic regression models were used to examine the association between IPV measured 3 years after the child's birth and increase in food insecurity from child's third to fifth birthday, as well as the mediating role of maternal depression, controlling for a number of maternal and household characteristics.
Results:
Mothers who reside in food insecure households and those who experience IPV share similar characteristics of socioeconomic disadvantage and a greater propensity for depression compared to their counterparts. Mothers' experiences of IPV predicted an increased risk of household food insecurity two years later, and the relationship was mediated by maternal depression.
Conclusions:
Food insecure mothers may benefit from widespread assistance. Targeting issues central to women's health must become a priority in combating food insecurity. Having IPV and mental health screenings coincide with food assistance applications may help identify women who would benefit from resources designed to increase physical safety, psychological well-being, and food security.
Introduction
F
Intimate partner violence and maternal depression
A particularly destructive consequence of the stress associated with economic hardship is the experience of IPV. 26,27 In the limited existing examination of this issue, Melchior and colleagues 28 and Wehler and colleagues 29 found higher rates of IPV among female-headed families experiencing food insecurity compared to those not experiencing food insecurity. Similarly, more recent research on female-headed households indicates that childhood trauma and violence are also associated with experiencing very low food security during adulthood. 30 It has been proposed that mothers use several management strategies so that their children avoid or limit hunger. 31,32 For example, it has been observed that low-income mothers reduce their dietary intake or skip a meal in order to provide food for their children. 33 Other research has suggested that the quality and quantity of food purchases among food insecure households are based on the sense financial security. 34 However, Wehler and colleagues 29 propose that the managerial strategies used to avoid hunger (also including providing the necessary time and attention to the task of acquiring food) may be hampered among mothers who experience IPV, placing the entire household at risk for experiencing food insecurity. We propose that the experience of depression among victims of IPV may be a mechanism accounting for their apparent impaired ability to obtain adequate food, resulting in the household to experience food insecurity.
A variety of research suggests that mothers' ability to obtain food in the context of economic hardship and violent relationships may be compromised by the mental health effects of experiencing IPV. IPV results in a wide range of mental health consequences for female victims, most prevalent of which is depression. Across studies, women who experience IPV have been found to be at approximately four times greater risk of developing depression than women who do not experience IPV, such that, on average, 48% of women who experience IPV also experience depression. 13 Further, depression has been found to be highly prevalent among food insecure mothers. 20,28 Therefore, among mothers who have experienced IPV, depressive symptoms may represent the severity of their negative psychological response to the violent experiences. In turn, depression may functionally impact their abilities to obtain food on a regular basis, likely due to factors such motivational and cognitive impairments, 28,35 decreased work productivity, 36 fewer supportive relationships, 37 and potentially including an inability to connect with individuals and institutions who may assist with food hardship.
Present study
In the current study, we focus on IPV and depression as risk factors for food insecurity to gain a more nuanced understanding of the role that women's health plays in the lives of families that experience food insecurity. To this end, we have three goals. Our first goal was to (a) examine IPV and depression across food secure versus food insecure households and (b) examine depression and food insecurity across mothers who have never experienced IPV versus those who have experience IPV. We hypothesized that, compared to their counterparts, a greater proportion of food insecure households and a greater proportion of mothers who experienced IPV would have experienced depression and characteristics of socioeconomic disadvantage. Our second goal was to investigate the longitudinal relationship between IPV and household food insecurity, controlling for risk factors related to these two variables. We hypothesize that mothers' experience of IPV will positively predict household food insecurity. Our third goal was to examine whether maternal depression mediates the relation between IPV and food insecurity. We hypothesized that depression would be a pathway by which IPV influences food insecurity.
This study extends previous research in important ways. As noted, a dearth of literature exists focused on the important association between IPV and hunger. Wehler and colleagues 29 provided limited evidence that IPV is more prevalent among households experiencing food insecurity, and the study was confined to a discrete geographic area and cross-sectional data. Melchior and colleagues 28 used longitudinal data; however, the sample was based on British families, a culture that has different methods of accessing social services. Further, the study performed by Melchior and colleagues 28 only included one sociodemographic risk factor in the multivariate regression models. In the present study, we focus on a multicity, socioeconomically disadvantaged sample of mothers with young children in the United States. This sample is ideal for studying the association between IPV and food insecurity because characteristics of socioeconomic disadvantage are highly correlated with IPV 38 –40,41 and food insecurity. 2 In addition, IPV occurs most frequently among young couples and families with young children. 42
The current study also focuses on a highly vulnerable population. As described, the occurrence of food insecurity among families with young children has particularly serious developmental consequences for children. 14 –20,23 –25 Additionally, exposure to parental IPV is a risk factor for children's poor physical, emotional, behavioral, social, and cognitive functioning. 43,44 It is also a concern that the different sources of stress that children experience residing in violent households could lead to the intergenerational cycle of violence and food insecurity. 30 Further, young children who reside with depressed mothers are more likely to demonstrate externalizing and internalizing behavior problems, 20,45 as well as adverse impacts on executive functioning, 46 physical growth, 47 and health. 48 Thus, studying the longitudinal relationship between maternal health problems and food insecurity among households with young children may inform the development of broader social services to provide food and maternal health assistance that can improve children's futures in a variety of ways.
Materials and Methods
Data are drawn from the main survey of Fragile Families and Child Well-being (FFCW) study, as well as the In-Home Longitudinal Study of Preschool Age Children, which comprises a subsample of families who participated in the main survey of the FFCW study. The FFCW is a longitudinal study of the conditions and capabilities of a disadvantaged urban cohort of 4,898 primarily unmarried parents of newborn children born between 1998 and 2000 in 20 U.S. cities where the population exceeds 200,000. Mothers and fathers in the main survey were interviewed separately soon after birth of their child (i.e., year 0), then interviewed again by telephone at 1, 3, and 5 years from the child's birth. We extracted data received from mothers in the main survey. The In-Home survey was administered when children were 3 and 5 years of age and included questions regarding household food security that were not available in the main survey. In most cases (96%) the In-Home survey was completed by the child's mother. 49,50 Information on sampling and design of the study has been previously reported. 49 –52 The study was approved by the Institutional Review Board.
Analytic sample
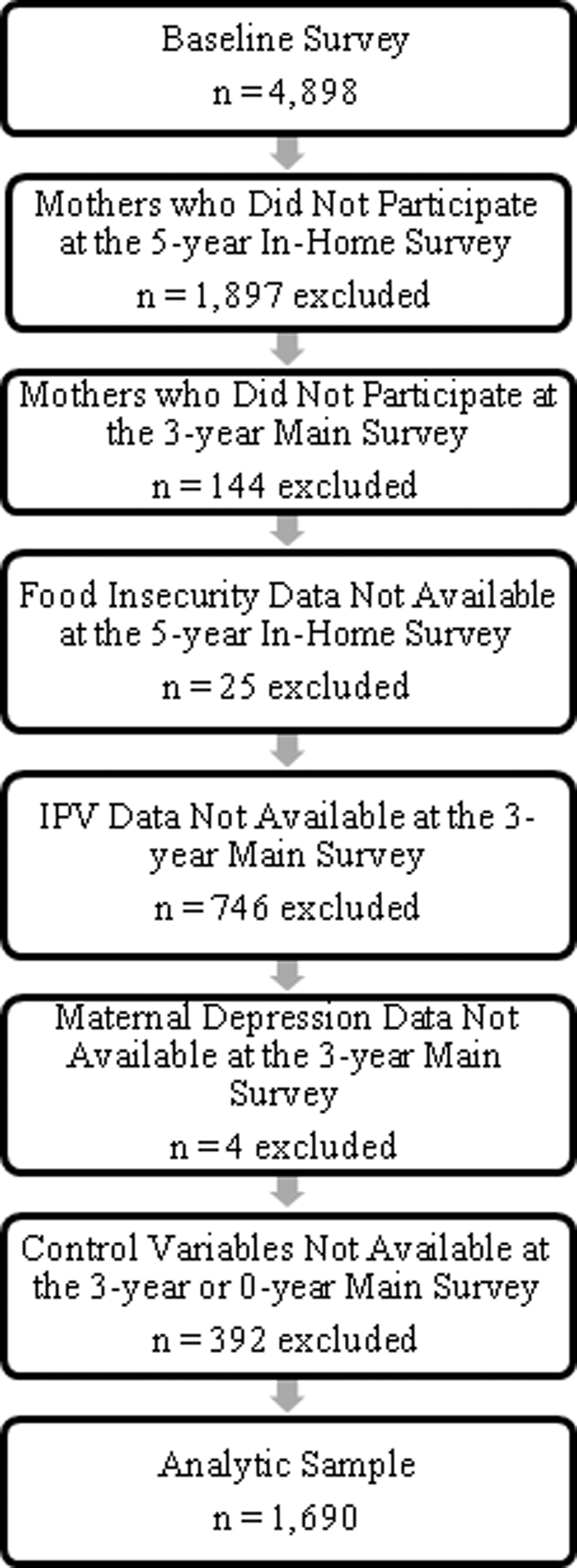
A total of 4,898 mothers were interviewed in year 0. As shown in Fig. 1, the analytic sample was restricted to mothers who participated in the 5-year In-Home survey (1,897 mothers excluded) and the 3-year main survey (144 mothers excluded). In addition, the sample was restricted to mothers who had complete data on household food insecurity at the year 5-year In-Home survey (25 mothers excluded), as well as IPV (746 mothers excluded) and depression (4 mothers excluded) data at the 3-year main survey, and the covariates (392 mothers excluded). The final analytic sample consisted of 1,690 mothers who were either romantically involved with the biological father of the child or another man.
Characteristics of the analytic sample.
Mothers who were excluded from the analytic sample were more likely than mothers included in the analytic sample to have experienced IPV as well as food insecurity at the 3- and 5-year In-Home Survey. Mothers excluded from the analytic sample were less likely white, more likely black, less likely to have a high school diploma, less likely to reside with her romantic partner, and more likely to be poor. There were no differences in the proportion of mothers who experienced depression between mothers excluded from the analytic sample and mothers included in the analytic sample.
Measures
Food insecurity
Mothers reported on household-level food security at the 3- and 5-year In-Home survey. The measure of food security is based on an 18-item scale developed by the U.S. Department of Agriculture (USDA) that assesses both the quality and quantity of food over the past 12 months. The scale captures food hardship due to financial constraints such as running out of food, perceptions that food in a household is of inadequate quality or quantity, and reduced food intake by adults or children. The USDA considers households food insecure if mothers respond affirmatively to 3 or more of the 18 items. 53
Intimate partner violence
Mothers reported whether, in the past year, they experienced physical abuse, sexual abuse, or restrictive and controlling behaviors from either the child's father or their current partner during the 3-year main survey. Physical abuse consisted of two items in which each mother reported (1) whether or not her partner “hit or slapped when he was angry” and (2) whether she was ever “cut/bruised or seriously hurt in a fight” with her partner. Sexual abuse consisted of one item assessing whether or not her partner “tried to make her have sex or do sexual things she did not want to.” Restrictive and controlling behaviors consisted of three items assessing whether her partner had (1) “isolated her from friends or family,” (2) “prevented her from going to work or school,” or (3) “withheld or controlled her money.” Affirmative responses were summed, with higher scores indicating greater exposure to violence (α=0.60). This scale has the same items used by Boyton-Jarrett, Fargnoli, Suglia, Zuckerman, and Wright. 54
Maternal depression
Maternal depression was measured using the Composite International Diagnostic Interview Short Form (CIDI-SF), Version 1.0, 55 at the 3-year main survey. The CIDI-SF questions originated from the Diagnostic Interview Schedule 56,57 and were designed to roughly correspond to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) 58 diagnostic criteria. Mothers were asked whether, at some time during the previous year, they had feelings of depression or were unable to enjoy things that they normally found pleasurable. Those who experienced at least one of these two conditions most of the day, every day, for a 2-week period were asked additional questions (e.g., having trouble concentrating, experiencing a change in weight of at least 10 pounds, having trouble sleeping, feeling worthless). Mothers who answered affirmatively to three or more questions were considered depressed. 55
Covariates
The following variables were included as covariates in the models because they reflect selection factors that could lead households to be food insecure as well as experience intimate partner violence: mothers' age, race/ethnicity, education level, employment status, relationship status, household income, and number of children in the household. All covariates were measured at the 3-year main survey, with the exception of race/ethnicity, which was measured at year 0 (i.e., at the time of the child's birth). Mothers reported on their age (years), race/ethnicity [white (reference), black, Hispanic, other], education [1=high school diploma, General Education Development (GED) test, or more; 0=less than high school education], employment (number of hours employed in the past year), relationship status (1=married/cohabiting; 0=romantically involved but not living with a partner), household income categorized into three levels with respect to federal poverty line (FPL) [poor (<100% FPL; reference), near poor (100%–199% FPL), not poor (≥200% FPL)], and number of children in the household. In addition, all models included food insecurity at year 3 in order to examine the change in food insecurity from year 3 to year 5.
Statistical analyses
Descriptive analyses and multivariate logistic regression analyses were conducted using STATA version 10.0 statistical software (StataCorp LP). Bivariate analyses were conducted on the food security subgroups and IPV subgroups based on one-way analysis of variance tests for continuous measures or chi-square tests for dichotomous measures. Multivariate logistic regression models were conducted and the odds ratio coefficients and 95% confidence intervals are presented. To assess whether depression mediated the relationship between intimate partner violence and food insecurity, methods outlined by Baron and Kenny 59 and Sobel and Leinhardt 60 were followed. In all regression models, we included covariates in the models and a baseline measure of food insecurity (from 3-year In-Home survey). This method accounts for potentially unobserved family characteristics that may be related to IPV and food insecurity.
Results
Sample characteristics
Table 1 presents descriptive statistics for all study variables for the full analytic sample and separated according to the presence of food security and IPV. Fourteen percent of the households experienced food insecurity, 16 percent of mothers experienced IPV, and 19 percent of mothers experienced depression.
p<0.001; ** p<0.01; * p<0.05.
Mean differences between the two sub-groups (e.g., food secure vs. food insecure) are based on one-way analysis of variance tests for continuous measures or chi-square tests for dichotomous measures.
Range is from 0 to 5.
Range is from 1 to 5.
FPL, federal poverty line; GED, General Education Development test; IPV, intimate partner violence.
Relative to food secure households, a greater proportion of mothers in food insecure households experienced IPV and depression. Food insecure mothers were less likely to be white, have completed their high school education, be in a married or cohabiting union, and more likely to be poor (i.e., <100% FPL). There were more children residing in food insecure households and greater proportion of these had experienced food insecurity in the previous 2 years.
When comparing IPV subgroups, a greater proportion of mothers who experienced IPV also experienced food insecurity and depression. Mothers who experienced IPV were less likely to be black and more likely to be Hispanic or other race, less likely to have received their high school diploma, employed fewer hours, and more likely to be poor (i.e.<100% FPL). There were more children residing in IPV households and greater proportion of these had experienced food insecurity in the previous 2 years prior.
Table 2 describes the proportion of mothers who experienced the prevalence of various forms of IPV. The majority of mothers experienced psychological IPV (i.e., restrictive and controlling behaviors from their partner). A smaller proportion of mothers experienced physical or sexual violence.
n=264.
Rates sum to greater than 100% as mothers could have been exposed to more than one form of IPV.
Longitudinal multivariate logistic regression models
The association between IPV and household food insecurity, as well as direct and indirect effects of depression, was assessed using longitudinal multivariate logistic regression models (Table 3). In Model 1, the association between IPV and food insecurity, accounting for all maternal and household characteristics was examined. Households in which mothers experienced IPV were at 22% greater odds of experiencing food insecurity. In Model 2, controlling for all maternal and household characteristics, the association between IPV and depression was assessed. Mothers who experienced IPV were at 44% greater odds of experiencing depression. The association between depression and food insecurity was assessed in Model 3, accounting for all maternal and household characteristics. Households in which mothers experienced depression were twice as likely to experience food insecurity. Last, in Model 4, both IPV and depression are included in the model, along with maternal and household characteristics. Similar to Model 3, households in which mothers experienced depression were approximately twice as likely to experience food insecurity. In regards to IPV, the odds ratio was no longer significant and decreased in magnitude from Model 1. The Sobel test indicated that depression fully mediated the relationship between IPV and food insecurity (z=2.89, p<0.01).
N=1,690.
p<0.001; * p<0.05.
The reduction in OR for intimate partner violence can be explained by the significant mediation effects of depression on intimate partner violence and food insecurity. The significant Sobel test mediation value was: 2.89 (p<0.01).
CI, confidence interval; OR, odds ratio.
Sensitivity models
To further assess the robustness of the mediating effects of depression on the IPV-food insecurity relationship, additional models were tested. We conducted models designed to test whether different types of IPV (i.e., physical, sexual, and restrictive/controlling behaviors) may be differentially influencing the key findings. In separate regression models, we included each individual type of IPV as the main predictor variable. Each type of IPV functioned in the same direction as the measure of total IPV; however, no individual type of IPV alone reached statistical significance (results available upon request). Thus, it appears that the measure of total IPV may better represent women's experiences and no individual form of IPV is independently driving the results. Additionally, because IPV and depression were measured concurrently, it might be argued that depression could differentially influence reporting of specific types of IPV; however, this does not appear to be the case.
Discussion
We focused on IPV and depression to increase the understanding of the roles that the family environment and women's health plays in the lives of families with young children that experience of food insecurity. Our first goal was to compare the characteristics of food insecure households and mothers who experienced IPV. Similar to previous research, our findings indicate that food insecure households are characterized by mothers experiencing depression and greater socioeconomic disadvantage than households that are food secure. 2 –4,20 For instance, mothers in food insecure households were more likely to be characterized by an incomplete high school education, poverty, a greater number of children, and a history of food insecurity during the past two years. Similarly, mothers who experienced IPV were more likely to be characterized as having experienced depression, an incomplete high school education, poverty, fewer weeks of employment, greater number of children, and a history of food insecurity compared to mothers who did not experience IPV in the past year. Thus, mothers who reside in food insecure households and those who experience IPV share similar mental health problems and characteristics of socioeconomic disadvantage, which may amplify their vulnerability and the vulnerability of their children.
Our second goal was to examine the longitudinal relationship between IPV and household food insecurity. Similar to previous research that has documented a link between IPV and food insecurity, 28,29 we found a small, but positive association, between IPV and food insecurity. Our third goal was to assess whether maternal depression plays a role in the relation between IPV and food insecurity. Indeed, the relation between IPV and food insecurity was mediated by mothers' symptoms of depression, suggesting that the experience of IPV leads to depressive symptoms that further impede mothers' ability to ensure food security in their homes. Mothers' depressive symptoms may further compromise the organizational and planning skills that encompass the managerial capacity needed to provide food for one's household. For example, depression may impact mothers' motivation to obtain and prepare food due to decreased appetite, physical and cognitive fatigue, and feelings of being overwhelmed by the task. 35,61 Depression may also increase feelings of helplessness when being psychologically controlled by a partner, 61 leading mothers to be especially challenged in terms of finding, accessing, and asking for the support they need. Thus, the managerial capacity of the mothers may have been greatly challenged by experiencing their partners' psychological and physical control, exacerbating depressive symptoms, and placing the entire household at risk for experiencing food insecurity.
Our results indicated that households were at greater risk of being food insecure when mothers experienced IPV strengthens the findings of previous research. 28,29 Not only does the current study add to the literature base by using different research methods among a different study sample, but it also addresses some limitations of prior research. For example, Wehler and colleagues 29 used cross-sectional data and Melchior and colleagues 28 based their sample on British families, a culture that has different methods of accessing public assistance. In contrast, we used longitudinal data that focuses on an urban, socioeconomically disadvantaged U.S. sample of mothers with young children and controlled for the degree of food insecurity at the time that IPV was assessed. In addition, we control for a number of confounding factors related to IPV and food insecurity. Thus, we can more confidently suggest that IPV leads to an increase in food insecurity over time.
Limitations of the current study bear note. First, the generalizability of the findings may be limited due to non-random sample attrition and a relatively large proportion of mothers having incomplete data on the measure of IPV. Although the FFCW study is based on socioeconomically disadvantaged young families in urban areas, the analysis sample may differ from the population of young families it was designed to represent, largely due to victims of IPV tending to be more difficult to recruit and retain in research studies. The importance of this limitation cannot be understated. At the same time, our sample size is comparable or greater than sample size in other studies that have examined relations among IPV, depression, and food insecurity; 28,29 thus our results may actually be more generalizable than many studies with significantly smaller sample sizes. Second, the proportion of mothers who experienced IPV in the current study is low compared to other samples of young mothers. 42 IPV prevalence rates vary substantially based on the measurement devices used. Although our measure of IPV utilizes the same items as Boyton-Jarrett et al., 54 and attempts to capture the multidimensionality of IPV, a wide range of IPV behaviors was not directly assessed, which could result in IPV to be underestimated. Third, the majority of mothers in the current sample largely experienced restrictive and controlling behaviors, as opposed to physical forms of IPV. However, sensitivity analyses suggested that these behaviors were not solely affecting the results, and it is important to note that the three forms of IPV are highly intercorrelated. 62 The low numbers of women reporting physical forms of IPV may be related, again, to the difficulty of recruiting and retaining vulnerable populations in research studies and the underreporting that is assumed to occur in self-reported measures of IPV. Unfortunately, the use of self-reported measures is a possible source of bias present in most IPV research and other research conducted on vulnerable populations when an alternative to self-report does not exist. Finally, IPV and depression were concurrently measured and, although we have no reason to suggest that depression might cause IPV, depression could arguably influence reporting of some forms of IPV (e.g., restrictive/controlling behaviors) over others. Our sensitivity analyses, which indicate that no individual form of IPV solely affected the results, lessen this concern.
The current study highlights the need for more widespread assistance for families at risk of being food insecure. Having IPV and mental health screenings coincide with food assistance applications would help identify and provide services to women in need as a means of benefitting their physical safety, psychological well-being, and food security of their household. Advertisement of IPV and mental health resources in locations such as Women, Infants, Children (WIC) Nutrition Program offices and on the back of electronic benefit transfer cards (i.e., the method in which food stamps are delivered to recipients) may prove beneficial. Addressing the IPV and mental health needs of low-income mothers may also indirectly assist with their children's development. Previous research indicates that young children who reside with depressed mothers and in households marked by IPV and/or food insecurity experience a variety of negative developmental consequences. 14 –20,23 –25,45 –48 Thus, improving the health of low-income mothers may also indirectly improve the developmental needs of their children. Although specific methods of intervention and prevention will need to be developed and tested, it is important that those who are invested in decreasing food insecurity begin to consider targeting women's health problems as a risk factor for food insecurity.
Footnotes
Acknowledgments
This project described was supported by award number K12 HD055882 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development to D.C.H. and A.M. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institute of Child Health and Human Development or the National Institutes of Health.
Disclosure Statement
No competing financial interests exist.