
Abstract
Objectives:
Latina breast cancer patients are 20 percent more likely to die within 5 years after diagnosis compared with white women, even though they have a lower incidence of breast cancer, lower general mortality rates, and some better health behaviors. Existing data only examine disparities in the utilization of breast cancer care; this research expands the study question to which utilization factors drive the shorter survival in Latina women compared with white women.
Methods:
This longitudinal linked Surveillance Epidemiology and End Results (SEER)-Medicare cohort study examined early stage breast cancer patients diagnosed between 1992 and 2000 and followed for 5–11 years after diagnosis (N=44,999). Modifiable utilization factors included consistent visits to primary care providers and to specialists after diagnosis, consistent post-diagnosis mammograms, and receipt of initial care consistent with current standards of care.
Results:
Of the four utilization factors potentially driving this disparity, a lack of consistent post-diagnosis mammograms was the strongest driver of the Latina breast cancer survival disparity. Consistent mammograms attenuated the hazard of death from 23% [hazard ratio, HR, (95% confidence interval, 95%CI)=1.23 (1.1,1.4)] to a nonsignificant 12% [HR (95%CI)=1.12 (0.7,1.3)] and reduced the excess hazard of death in Latina women by 55%. Effect modification identified that visits to primary care providers have a greater protective impact on the survival of Latina compared to white women [HR (95%CI)=0.9 (0.9,0.9)].
Conclusions:
We provide evidence that undetected new or recurrent breast cancers due to less consistent post-diagnosis mammograms contribute substantially to the long-observed Latina survival disadvantage. Interventions involving primary care providers may be especially beneficial to this population.
Introduction
Latina breast cancer patients are 20 percent more likely to die within 5 years when compared with whites of the same age and stage at diagnosis. This survival disparity is noted despite lower incidence rates of breast cancer in Latina women, 1 lower general mortality rates 2 and reports of better health behaviors, such as lower tobacco and alcohol use, among Latino populations. 3 More than 1 in 100 women in the United States are currently enduring the uncertainty of living with a breast cancer diagnosis, and 1.6 million women will be alive with breast cancer in 10 years. 4 The U.S. population is 16.7 percent Latino, representing over 52 million people, making Latino Americans a significant population of concern. 5
Multiple studies have investigated disparities in race and ethnic minorities' utilization of care 6 –9 ; however, to our knowledge, no studies have examined if utilization factors play a role in the shorter survival of Latina breast cancer patients. Many studies report Latina women use less routine physician services and pre-diagnostic screening mammograms. 10 –13 Given that the reasons African Americans have shorter survival than whites includes utilization of post-diagnostic care, controlling for tumor characteristics, and delay in diagnosis, 4,6,14 –16 researchers have hypothesized that reduced utilization of timely high quality follow-up care reduces survivorship from early stage breast cancer in the Latina population. We hypothesize that Latina women have shorter 5-year survival rates than whites due to modifiable behaviors related to the utilization of health care. Utilization factors examined include quality of initial care, yearly follow-up post-diagnosis mammograms, yearly primary care clinician visits, and yearly follow-up specialist visits.
Methods
Study population
We conducted this study using the merged Surveillance Epidemiology and End Results (SEER) Medicare population-based cancer registry sponsored by a collaboration between the National Cancer Institute and the Centers for Medicare and Medicaid Services. 17 The cancer patients represent approximately 28 percent of the U.S. population and 93 percent of the cancer patients are linked to Medicare claims records. 18 These data allowed us to examine patients 1 year before diagnosis (for preexisting comorbid conditions) and examine their utilization of care before diagnosis until up to 11 years after diagnosis or death. The University of Nevada, Reno Office of Human Research Protection approved the study.
Case ascertainment
Eligibility included stage 1 and 2 breast cancer patients diagnosed and reported to the cancer registry between 1992 through 2000, age 66 years and older. We used exclusion criteria to maximize patients whose claims data were complete; excluded women using Medicare due to chronic disability and those diagnosed on a death certificate, at autopsy or in a nursing home. We excluded women who were not enrolled continuously in Medicare fee-for-service plans (both Part A and B) from 1 year prior to diagnosis through the observation period. We only included confirmed paid claims thus excluding managed care enrollees and focused in white and Latina women only. We linked the resulting cohort to Medicare carrier, outpatient, and hospital files. The final sample size was 44,999 women with breast cancer, of whom 1560 (3.3%) were Latina and 43,439 were white (Fig. 1).
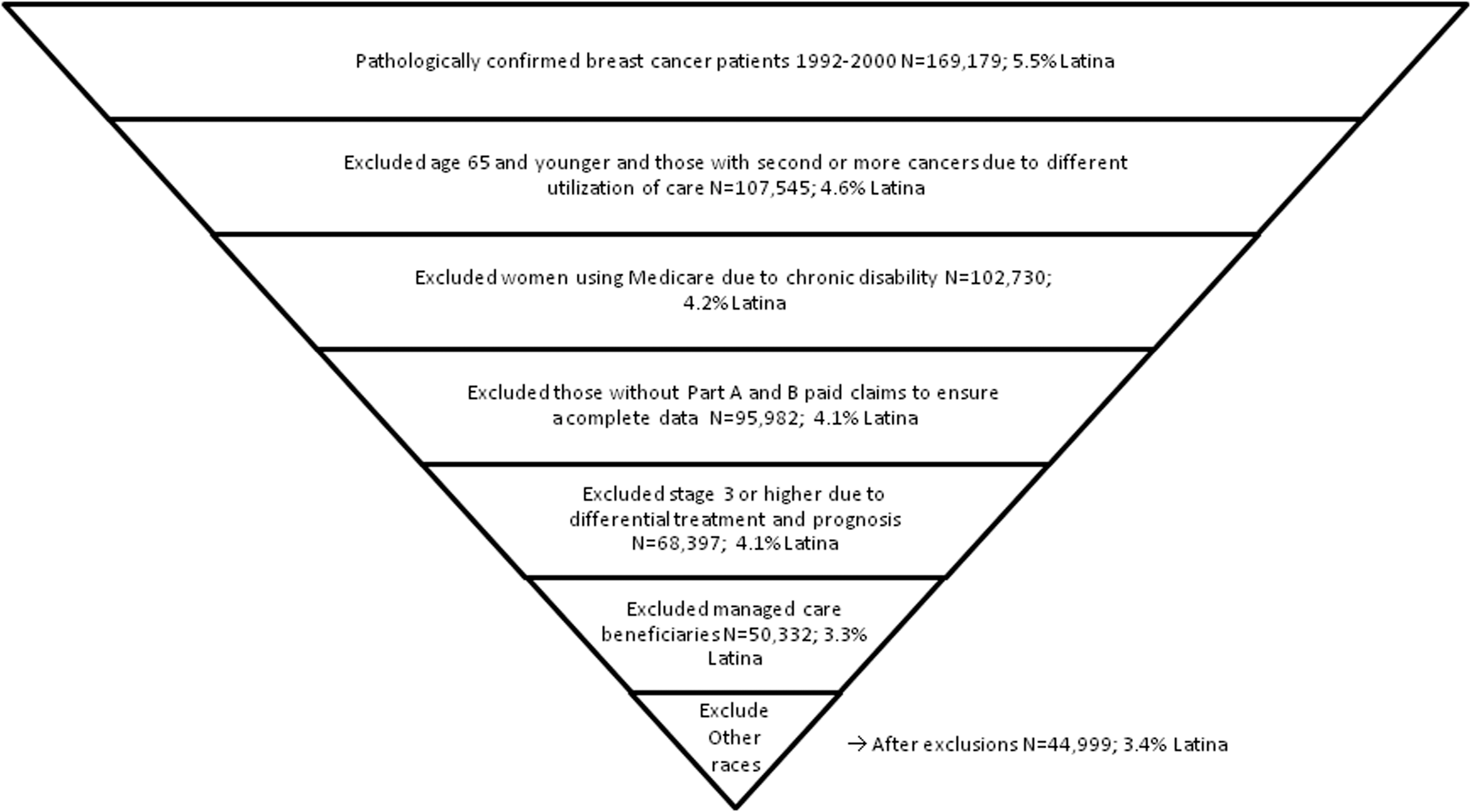
Selection criteria for Surveillance Epidemiology and End Results (SEER)-Medicare patients.
Primary outcome
Survival time was defined as months between diagnosis and death date. We considered three types of death: all causes, breast-cancer-specific, and other causes of death. The minimum follow-up was 5 years and stopped after 2005 or after 11 years due to sparse data.
Variables influencing survival
A priori variables
We defined three a priori variables (ethnicity, age, and stage) because they are intrinsic to our primary study question: Why do Latina women have shorter survival than whites, controlling for age and stage at diagnosis? We categorized patients according to known ethnicity in SEER as abstracted from the medical record and by the Hispanic Identification Algorithm based on surname developed, validated, and described by the North American Association of Central Cancer Registries. 19 SEER defines stage at diagnosis using the American Joint Committee on Cancer criteria. 20 We defined age as a yearly increasing time-dependent variable. In the descriptive analysis, we categorized age in three groups for comparison with other research.
Health care utilization
Variables include adequate care, mammography, and physician specialty and were identified from SEER and Medicare using diagnosis and procedure billing codes: Internal Classification of Diseases, Ninth Revision, Clinical Modification, Current Procedural Terminology codes and the Healthcare Common Procedure Coding System (HCPCS). 21 –23
Adequate care
This was defined as receiving breast conserving surgery plus radiation or mastectomy, and estrogen receptor (ER) status documentation (all criteria=1; some or none of the criteria=0) based on previously used methodology. 7 Data of receipt of surgery and radiation therapy were obtained from both SEER and Medicare. ER status documentation (yes/no) was collected from SEER and is necessary to determine appropriate chemotherapy. 7
Mammography
We examined if women received at least a yearly mammogram (consistent mammograms) after diagnosis as a time-dependent variable, since intervals shorter than 12 months are not more effective than are 1-year intervals. 24 Since many women did not have mammograms in the year of death, partially because women do not survive the entire year, we censored mammograms done in the year of death. Mammogram identification in Medicare datasets was reported 94% accurate. 25
Physician specialty
We examined if women received at least a yearly clinician visit (consistent visits) as a time-dependent variable. We defined specialists using these specialty codes from the Healthcare Provider Taxonomy Code (HPTC) used by the Center for Medicare and Medicaid Services: 83 or 90, oncology; 92, radiation; 49 and 91, general; and surgical oncologists, 91. We defined primary care clinicians using HPTC with the following specialty codes: 01, generalist; 11, general practice; 08, internal medicine; 16, family practice; 38, obstetrics/gynecology; and 70, geriatric and multispecialty practices. 6 Since much of the healthcare utilization is captured longitudinally (i.e., women see their physicians multiple times per year and undergo multiple mammograms after diagnosis), we allowed health care utilization variables to change yearly (time-dependent variables). The variable was coded 1 or 0 depending on if the patient used the health care in a particular year; thus, consistency of utilization (at least one use per year) was measured using time-dependent variables. Two functional forms for the time-dependent variables were considered: (1) a yearly step function, where provider visits and mammograms that occurred during the year were attributed to that year and (2) a time-lagged covariate where provider visits and mammograms were attributed to the preceding year. Many women dying of breast cancer did not use screening or preventative health care the year they died; therefore, more information would be available from the previous year. 26
Adjustment variables
The Klabunde comorbidity index, specifically for use in claims data during the 11 months prior to a cancer diagnosis, was used to assess comorbid conditions (excluding cancer). 27 This index includes 19 comorbid conditions, accounts for number and the seriousness of these conditions and has been validated against mortality rates, complication rates and length of stay in hospitals. 27 Census demographic variables are used because this information is not available from the cancer registry nor claims records. We included, at the census tract level, estimates for percent married, mean income, urban or rural residence, and proportions from census tracts (CTs) where more than 50% of all households reported having at least one non English-speaking member age 65 or older, defined as limited English proficiency (LEP).
Analysis
Descriptive statistics
We assessed ethnic differences in patient characteristics using Student's t-test and chi-square tests. For time-dependent utilization of care variables, we used logistic regression for repeated measures via generalized estimating equations. 28 We constructed Kaplan-Meier survival curves with Greenwood variance estimation and the Log-rank test statistic to investigate survival differences between race/ethnic groups.
Multivariable statistics
Nonproportional Cox hazards regression models with robust sandwich variance estimation were constructed. 29 The counting process style of input was used to analyze time-dependent covariates (PROC PHREG Multipass, SAS version 9.2, SAS Institute). 30 Censoring was assumed noninformative based on SEER-Medicare data accrual mechanisms. For non-time-dependent variables, the proportionality assumption was assessed using graphical methods.
Inferential analyses
To assess the most important variables associated with Latina breast cancer survival, we compared multiple models. First, a priori variables were included in the model (ethnicity, age, and stage), then adjustment variables derived from census tract linkage (marital status, language spoken at home, median income) and the comorbidity index. Finally, healthcare utilization variables (mammography, physician and specialists visits, and adequacy of initial treatment) were included. Clinically collinear variables (i.e., mammograms and visits to physicians) were assessed in hierarchal and separate models. Two-sided p-values were used in all analyses.
This study compares a series of statistical models to answer the primary study question of identifying the most important health care utilization variables associated with shorter survival in Latina relative to white women. We assessed this three different ways. First, by comparing the crude and adjusted hazard ratios (HR) for Latina women and reported the percent of decrease (attenuation) in the Latina HR. A 10% or greater reduction in the Latina HR suggests that the utilization variable explains shorter survival better than ethnicity does (i.e., it is a confounder).
31
Second, we calculated the excess risk of death attributable to each utilization variable. The excess risk (ER) is calculated using the formula
Finally, we assessed if there was residual confounding in the Latina HR indicating that other variables explaining the relationship are missing or that the existing variables do not provide complete control of the association.
It seems reasonable that women who consistently interact with the healthcare system for one type of health service may also consistently interact with the health care system for other types of services. For example, women who visit primary care clinicians (PCCs) consistently might also have regular mammograms ordered, as there are more opportunities. So as a secondary question, we wanted to see if this observation was noted in Latinas and whites alike or if there were differences in utilization patterns by ethnicity. To answer this question, we identified statistically significant three-way interactions between two different utilization variables and ethnicity. To present results, we stratified the data by ethnicity and calculated the interaction. Thus, interpretation of synergistic relationships between utilization variables (the interaction) should be within ethnicity (white or Latina) and not between ethnicities. We assessed effect modification after adjusting for confounding. 32–33
Since Medicare expenditures, physician assignment rate, and health system characteristics may vary by state, we did a sensitivity analysis by adding state of residence to see if this changed the HRs. We also conducted a sensitivity analysis between the different functional forms of the time-dependent variables.
Results
Patient characteristics
The study population consisted of 1,560 Latinas and 43,439 whites. Latinas were significantly younger when diagnosed when compared with other ethnic groups and had greater proportions of LEP CT's (81.5%; Table 1). Latinas were more likely to be diagnosed at stage 2, had greater number of comorbidities, had lower average income, and lived in areas where more households had residents with limited English proficiency (Table 1).
Percentages are shown in parentheses.
Numbers may not add up to total due to missing data.
Statistically significant differences via Students t-test.
N=44,999 women with stage 1a, 1b, 2a, or 2b breast cancer.
CT, census tract; ER, estrogen receptor; LEP, limited English proficiency; SD, standard deviation; SEER, Surveillance Epidemiology and End Results.
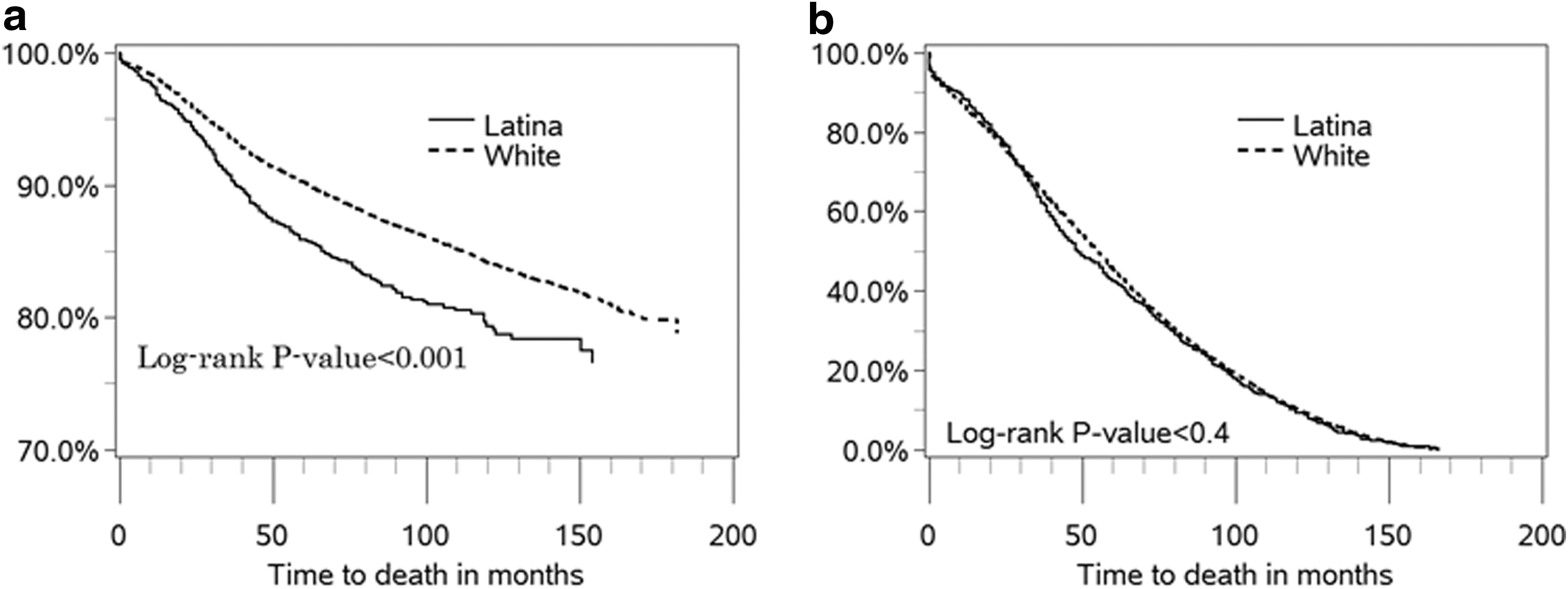
For breast cancer-specific deaths, Latina women have statistically shorter survival compared with whites (p<0.0001; Fig. 2a). There were no significant differences between white and Latina women for other causes of death (Fig. 2b). We confined all further analyses to breast cancer-specific causes of death.
Lower proportions of Latina women received yearly mammograms compared with whites nearly each year of follow-up; p=0.01 (Fig. 3a). Utilization of primary care clinicians by ethnicity was similar to mammography, with lower proportions of Latina women than white women visiting a primary care clinician; p=0.01 (Fig. 3b). Conversely, higher proportions of Latina women visited a specialist, compared with white women; p=0.009 (Fig. 3c).
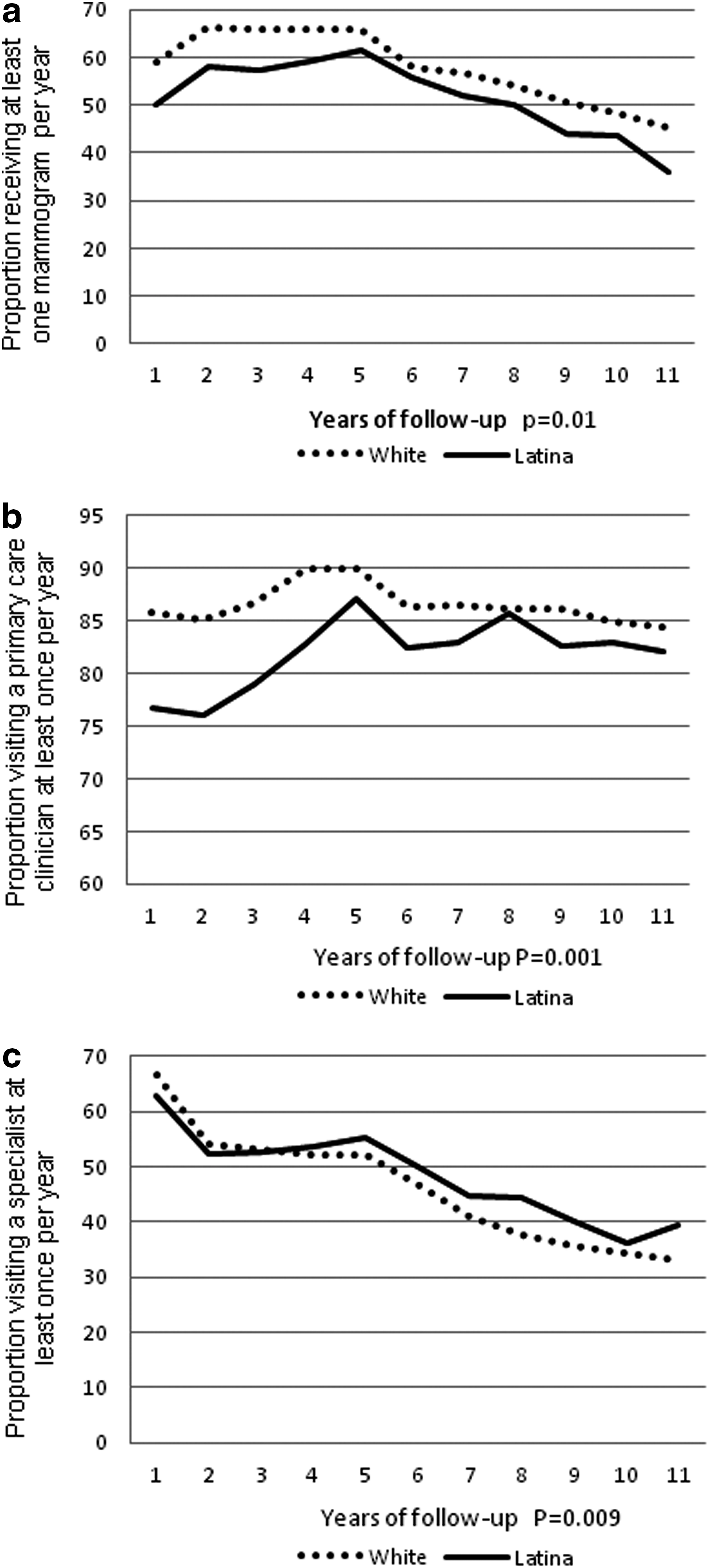
Receipt of yearly post-diagnosis
Contributors to Latina survival disadvantage
To answer our primary study question, we created several models and compared the reduction in the hazard of death in Latina women by healthcare utilization variables of interest. The left-hand column of Table 2 identifies the separate models with different utilization variables. We ran the models with and without adjustment variables (comorbidities, income, proportion LEP CTs, percent married at CT level), and these variables in total did not meet any of the definitions of confounding; they only attenuated the Latina HR by 3%. The HR of all health care utilization variables were significant, however; by comparing separate models, only follow-up mammograms (at least one per year) met all three definitions of confounding: it attenuated the Latina survival disadvantage by the greatest amount (13%), explained the greatest amount of the excess risk (55%), and eliminated residual confounding. Differences were insignificant between the two functional forms of the time-dependent variables (data not shown).
Cox hazard regression analysis with non-proportional hazards (time-dependent variables). The reference group is white women.
Age and stage controlled for in all models (1).
Additional confounders: comorbidities, income, LEP CTs, marital status, urban/rural residence. All were statistically significant, although some were marginally clinically significant; that is, the point estimates of the hazard ratio were very close to 1.
Less consistent mammograms is defined as less frequent than annual.
Consistent mammograms is the only variable that attenuated the Latina survival disadvantage so that it was not statistically different from whites.
Consistent primary care clinician (PCC) and specialist visit refers to at least one annual visit.
HR, hazard ratio.
We found statistically significant differences between whites' and Latina's use of (a)PCC visits and mammograms, and (b) PCC and specialists visits (Table 3).The significant interaction between PCC visits, mammograms, and ethnicity was driven by statistically significant differences in white women but not Latina women, meaning their risk of inconsistent mammograms did not depend on whether they saw a PCC consistently or not, consistent with the results in Table 2. The sensitivity analysis by state of residence of breast cancer cases revealed that the mortality HRs for Latinas were not significantly different from models without the state data.
N=4796
Interpretation of the interaction should be within ethnicity (white or Latina) and not between ethnicities.
Discussion
In a large cohort of fee-for-service Medicare recipients, we found that consistent utilization of annual post-diagnosis mammograms could largely explain the survival disparity between Latina and white women diagnosed with early breast cancer Our results provide an explanation for the observed shorter survival in Latina compared with white women and explicitly supports the hypothesis that utilization of primary care clinical services could eliminate this disparity. These results have major implications for clinicians, healthcare organizations, and public health systems and should be used to implement policy and systems change to enhance access to mammography for Latina women after diagnosis of early breast cancer.
Although this survival disadvantage is frequently noted in the literature, studies have not specifically examined possible reasons for this observation. The standard of care is yearly post-diagnosis mammograms for life. 34 –36 Recent studies indicate post-diagnosis surveillance mammograms reduce breast cancer mortality by 25%–47%. 37–38 The rate of recurring breast cancers or development of a new primary breast cancer is constant for at least 14 years after diagnosis, 11 clarifying the importance of long-term follow-up in cancer survivors. In this analysis, ethnicity confuses the relationship between mammography and shorter survival; it met all three definitions of confounding: it attenuated the survival disadvantage by 13%, reduced the excess hazard of death in Latina women by 55%, and left no residual confounding.
Latino populations have lower mortality, lower cancer rates, and longer life expectancy despite paradoxically unfavorable demographic factors such as lower socioeconomic status and rates of health insurance. 39 Some researchers hypothesize adherence to preventative health behaviors as the reason. 40–41 Our effect modification results indicate a synergism between visiting clinicians and having mammograms in whites only. The interactions between PCC and specialists visits concur with the observation that Latina women see specialists more often than do whites (Fig. 2c) and that specialist visits do not contribute to the Latina survival disadvantage (Table 2). One may expect to see women that have consistent specialists visits might be at a higher risk of death due to a more complicated clinical course, but this does not appear to be the case for this population-based assessment of Latina women. This suggests some Latina women without adverse prognostic factors may be using specialists as their primary care although this is a question that deserves further study.
This study provides important information for developing interventions in the Latina population, since access to health care and utilization factors are modifiable and can incorporate culturally appropriate components. Clinicians serving Latina women should find this study particularly relevant, as it identifies their potential influence on the behavior of Latina women. Additionally, transfer of care between specialists and primary care physicians might also be especially important in Latina women. Since recurrences diagnosed through mammography results in significantly longer survival compared with clinically detected recurrences, 42 routine annual follow-up mammograms need to be emphasized to Latina women.
Multiple studies report the barriers experienced by Latina women in obtaining breast healthcare. 43 –46 For example, difficulties Latina women have obtaining adequate treatment at the patient level could be addressed through culturally sensitive navigation programs to improve familiarity with Medicare 4,10 or with health systems in general. Family members may be especially important to Latina women seeking treatment for breast cancer 47,48 and should be included in discussions of treatment and follow-up plans. Obstacles for patient's referral for follow-up care at the institutional level could be addressed by institutional quality improvement efforts in multidisciplinary coordination and culturally and linguistically appropriate outreach to Latinas.
This study has several limitations. We investigated ethnic disparities in the follow-up care of women with breast cancer in a Medicare-insured population using fee-for-service healthcare and thus provides timely insight with the prospect of expanding healthcare coverage. The breadth of the SEER-Medicare dataset gave us adequate statistical power but also limited our analysis to patients older than 65 and those using fee-for-service providers. Latinas may be more likely to enroll in Medicare managed care, but claims data for managed care users are currently unavailable. If managed care claims become available on a population basis, this could be an area of future research. Furthermore, this research excludes the population of Latina women who are not eligible for Medicare due to their employment. We excluded women with documented recurrence or second breast cancers, which could also be a focus of further research. Even though we relied on multiple linked datasets, mobile mammography clinics and the difficulty differentiating between diagnostic and screening utilization codes could have underestimated mammogram utilization. Missing data would bias our results towards the null and our detected association between utilization of mammograms might underestimate long-term survival. So if Latina women have a greater amount of missing mammography data compared with white women, the impact of the importance of mammography could be greater than we reported. Since this analysis focused on an insured population—women using Medicare—it should be interpreted as a “best-case scenario.” Disparities may be more marked in younger Latina women who are more likely to be uninsured and have poor access to mammography.
Other studies have identified the role of language as factors affecting health outcomes. 49–50 However, individual language variables were unavailable in this dataset, and the use of census-derived proxy variables may be insufficient to detect the potential role of language. Analysis of specific Latina national origin groups and by language proficiency could be an area for future research. Other factors that were unavailable to us such as diet and exercise could attenuate our results, but given the magnitude of effect of mammography, that a lack of a mammogram increases the hazard of death five-fold (HR=5.68), it is unlikely that such data would attenuate our results to any significant degree.
The administration of adjuvant non-hormonal chemotherapy to women with stage 1 or 2 breast cancer diagnosis is uncommon, especially in women over age 65, and is probably not an important contributor to survival. However, this study lacks data on the use of estrogen receptor modifiers (SERMs) such as tamoxifen or more recently aromatase inhibitors (AIs), and this is a potentially important limitation. Use of SERMs and AIs for 5 years decrease new breast cancer and/or recurrence by 50% among women with an initial diagnosis and is the standard of care in women with positive hormonal receptors. 51 Given the age range of these women, one would expect about 75% to have a positive estrogen receptor. Thus, differential uptake in the use of SERMs and AIs may in part explain some of the survival differences observed. However, a recent study found no ethnic differences in Medicaid patients for whom it was indicated. 52 However, from a quality of care perspective, the use of SERMs/AIs in women with positive estrogen receptors is an indicator that future researchers should incorporate in the definition of adequate care among women with breast cancer.
In conclusion, as cancer survivors live longer, follow-up health care is essential to reduce future morbidity through surveillance for new malignancies and monitoring for the delayed effects of treatment. Key elements for a cancer survivorship agenda are developing evidence-based approaches to high-quality health care including risk tailored screening and improved interaction between patients and health care services. 24 The U.S. Centers for Disease Control and Prevention recommends establishing clinical practice guidelines for each survivorship stage and developing and disseminating public education programs capable of empowering cancer survivors to make informed decisions. 53 This study identifies a vulnerable target group who could benefit from information regarding the influence of post-diagnosis yearly mammograms on the survival disparity in the Latina population. Primary care clinicians and specialists can implement risk tailored preventative health education and empower Latina breast cancer survivor's decision-making process. Thus, the results of this research are directed not only at researchers and clinicians but also to health policy makers, health and screening managers, and hospital specialists.
Footnotes
Acknowledgments
This project was supported by the Network for Multicultural Research on Health and Healthcare, Department of Family Medicine, David Geffen School of Medicine, University of California, Los Angeles; funded by the Robert Wood Johnson Foundation, and by grants 1R03CA153098-01 and U01-CA86117 and U54-CA153511 (Redes En Acción) from the National Cancer Institute at the National Institutes of Health. The authors would like to thank the anonymous reviewers for their valuable comments and suggestions to improve the manuscript.
This study used the linked SEER-Medicare database. The interpretation and reporting of these data are the sole responsibility of the authors. The authors acknowledge the efforts of the Applied Research Program, National Cancer Institute; the Office of Research, Development and Information, Centers for Medicare & Medicaid Services; Information Management Services, Inc.; and the Surveillance, Epidemiology, and End Results Program tumor registries in the creation of the SEER-Medicare database.
Disclosure Statement
No competing financial interests exist.