
Abstract
Objective:
Bariatric surgery can reduce the risk of obesity-related complications of pregnancy, but may cause essential nutrient deficiencies. To assess adherence to laboratory testing guidelines, we examined frequency of testing for and diagnosis of deficiency during preconception and pregnancy using claims data in women with a delivery and bariatric surgery.
Methods:
Retrospective analysis of claims from seven Blue Cross Blue Shield plans between 2002 and 2008. We included women with a delivery and bariatric surgery within the study period. We used common procedural terminology (CPT) and ICD-9 codes to define laboratory testing and deficiencies for iron, folate, vitamin B12, vitamin D, and thiamine. Using Student's t-test and chi-square testing, we compared frequency of laboratory tests and diagnoses during 12 months preconception and 280 days of pregnancy between women with pregnancy before versus after surgery. We used multivariate logistic regression to evaluate for predictors of laboratory testing.
Results:
We identified 456 women with pregnancy after bariatric surgery and 338 before surgery. The frequency of testing for any deficiency was low (9%–51%), but higher in those with pregnancy after surgery (p<0.003). The most common deficiency was vitamin B12 (12%–13%) with pregnancy after surgery (p<0.006). Anemia and number of health provider visits were independent predictors of laboratory testing.
Conclusion:
Women with pregnancy after bariatric surgery were tested for and diagnosed with micronutrient deficiencies more frequently than those with pregnancy before surgery. However, most laboratory testing occurred in less than half the women and was triggered by anemia. Increased testing may help identify nutrient deficiencies and prevent consequences for maternal and child health.
Introduction
N
Deficiencies of essential micronutrients, such as iron, folate, and vitamin D, can lead to maternal anemia and impaired neural tube development and may be associated with preeclampsia. 12 –15 The monitoring of nutrient deficiencies after bariatric surgery, despite routine multivitamin supplementation, is important. 16 –18 Guidelines suggest screening for micronutrient deficiencies annually beginning the year after bariatric surgery. 19,20 There are no prior investigations of laboratory testing for and diagnosis of micronutrient deficiency in women who become pregnant after bariatric surgery.
Our objective was to assess the frequency of screening for deficiencies of iron, folate, and vitamins B1, B12, and D in women who became pregnant after bariatric surgery compared to those who became pregnant before bariatric surgery. We also assessed the frequency of diagnoses for vitamin deficiencies and determined the predictors of testing for vitamin deficiencies in pregnant women following bariatric surgery. We hypothesized that testing would occur more frequently in women with a pregnancy after bariatric surgery than those with a pregnancy before bariatric surgery.
Methods and Procedures
Study design and data source
We performed a retrospective analysis using insurance claims data from 2002 to 2008. We used claims data from seven Blue Cross Blue Shield health plans, providing coverage in seven areas: Tennessee, western Pennsylvania, Michigan, North Carolina, the city of Philadelphia in Pennsylvania, South Dakota and Iowa (included in the same plan), and Hawaii. The data included insurance claims information (including hospitalizations, clinic visits, and laboratory tests) and variables for age, sex, and geographic area, but not clinical variables such as BMI or demographic information such as race or socioeconomic status. Inclusion in this obesity-related data set required at least one of the following criteria at any point during 2002–2008: completed health risk assessment or other survey; claim for a diagnosis of obesity; claim for bariatric surgery; prescription claim for a weight reduction medication; or diagnosis code of hyperlipidemia, type 2 diabetes, sleep apnea, gallbladder disease, or metabolic syndrome. These diagnoses were identified by common procedural terminology (CPT) codes, ICD-9-CM (International Classification of Disease, ninth revision, clinical modification codes), or diagnosis-related group codes. We acquired data on enrollment files for administrative data; benefits information to determine medical coverage; and inpatient and outpatient claims records containing ICD-9 diagnosis, common procedural terminology codes, and costs and charges.
Selection of study sample
We included women who had claims for both bariatric surgery (see Appendix A) and a delivery, defined as one or more live births or stillbirths (Appendix B) associated with a claim with an inpatient point of service code. We excluded delivery dates either less than 280 days after bariatric surgery or less than 31 days before surgery. If a woman had two or more deliveries, or had a delivery both before and after surgery, we selected the delivery closest to her bariatric surgery, which maximized coverage. For women with more than one claim around the time of their delivery, we identified the delivery date for this analysis as the date of service with the most delivery records/claims.
For each woman, we compared the delivery date(s) with the date of the claim for bariatric surgery. Women were classified into groups that delivered before or after surgery based on date of delivery in relation to surgery such that no woman was included in both before and after surgery groups. The study group of interest was women who had a delivery after bariatric surgery and the comparison group was women who had a delivery prior to bariatric surgery. We chose our comparison group because it likely included women with Class II obesity with comorbid conditions or Class III obesity since these are the indications for bariatric surgery and our claims database does not provide BMI data.
We further excluded women with pre-existing disorders that could impact micronutrient absorption and consequently affect frequency of testing and deficiency: pernicious anemia (ICD-9 281.10), alcoholism (ICD-9 303), pancreatic diseases (577.xx), and Crohn's disease (555.xx). We restricted our analyses to women aged 12–45 years at the time of delivery, who had continuous insurance coverage during pregnancy (280 days prior to delivery) and during the year prior to the estimated date of conception.
Definitions of outcomes: micronutrient testing and deficiencies
We assessed primary outcomes during the 12 months prior to conception and 280 days of pregnancy. Primary outcomes were laboratory testing for the following micronutrients: iron, folate, vitamin B12, thiamine, and vitamin D. We chose these nutrients to reflect the deficiencies that occur following bariatric surgery, for which expert recommendations suggest screening 19,20 and which may impact both maternal and fetal outcomes. 13,15,21 We defined laboratory testing using CPT codes for both basic and optimal laboratory tests (Table 1) for the micronutrients of interest. “Basic” was defined as a laboratory test for the micronutrient of interest, and “optimal” included laboratory testing according to recent guidelines for postbariatric surgery management. 20
CPT, common procedural terminology code.
ICD-9, International Classification of Diseases, Ninth Revision.
PTH, parathyroid hormone; MMA, methylmalonic acid; RBC, red blood cell; TIBC, total iron binding capacity.
The secondary outcomes were the diagnoses of nutrient deficiencies during the preconception and pregnancy periods, including iron, folate, vitamin B12, thiamine, and vitamin D deficiencies. We used both ICD-9 and procedure codes to define both the deficiency and the conditions (e.g., anemia) resulting from deficiency (Table 1). A diagnosis of any anemia due to nutritional deficiency was identified through ICD-9 codes (281.1, 281.2, 281.3, 280, 280.1, 280.9). As a control for universally recommended pregnancy-specific testing, we assessed syphilis screening (RPR) during pregnancy (defined by CPT codes 80055, 86592, 86593, 86781, 87166, 87164, 87285).
Definitions for other covariates
In the multivariate logistic regression analyses, our covariates included maternal age, number of visits to a health care professional (categorized into tertiles) as a proxy for contact with a health care provider and medical complexity, and Blue Cross Blue Shield insurance plan. Maternal age was categorized into two groups, ≤33 years or ≥34 years, to include approximately 50% of the sample in each group. We categorized number of visits into “low” (0–7 visits), “medium” (8–15 visits), and “high” (>16 visits) groups.
Statistical methods
We compared the clinical characteristics of women who delivered before and after surgery using Student's t tests for continuous variables and χ2 tests for categorical variables. We calculated the proportion of women with the desired testing for nutrient deficiency outcomes in the before and after bariatric surgery groups. We tested for the differences between groups using Fisher's exact test.
In the second part of our analysis, we used logistic regression to calculate the odds ratio and confidence intervals for the primary outcomes of laboratory testing. We created a composite laboratory testing outcome, combining basic and optimal laboratory testing outcomes, and controlled for insurance plan and the time between surgery and delivery as covariates in the model. We then used a stepwise analysis to identify predictors for laboratory testing, including visit frequency, maternal age at delivery, and diagnosis of anemia.
P values less than 0.05 were considered significant. Statistical analyses were performed with SAS statistical software, version 9.1 (SAS, Cary, NC).
Results
Figure 1 displays the flow of the selection of subjects for the study. We identified 456 women with a pregnancy after bariatric surgery and 338 women with a pregnancy before bariatric surgery.
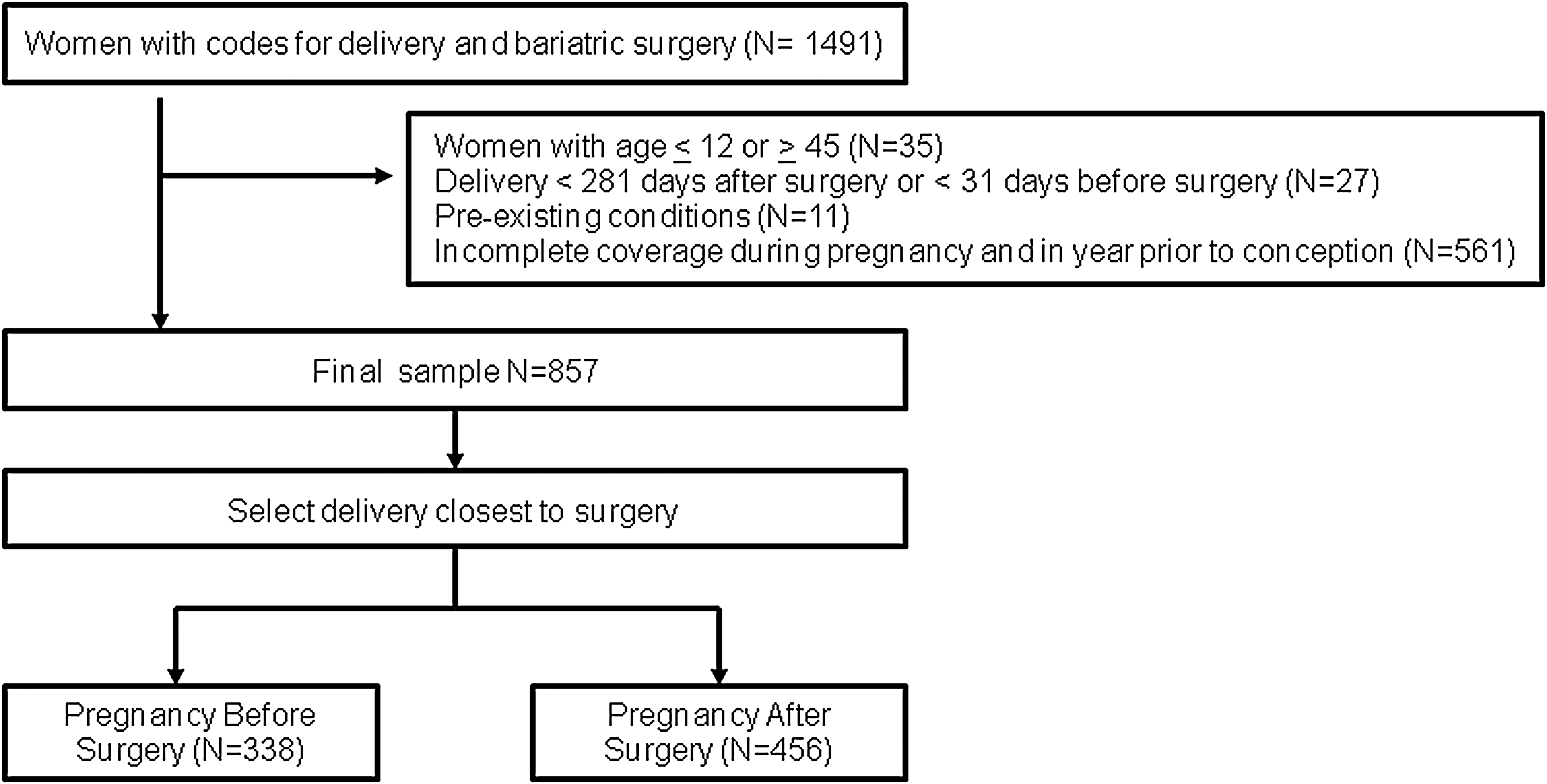
Enrollment flow for selection of study sample.
The characteristics of the women with deliveries before or after bariatric surgery are presented in Table 2. The majority of surgical procedures performed were laparoscopic or open Roux-en-Y gastric bypass surgeries (80%). Women who had a pregnancy after bariatric surgery were, on average, older at delivery (32.3 vs. 31.3 years, p<0.0001) and younger at time of surgery (30.7 vs. 32.9 years, p<0.0001) and had a higher number of outpatient visits in the year prior to conception (13.7 vs. 7.7 visits, p<0.0001) and during pregnancy (14.8 vs. 11.4 visits, p=0.0006). Women who had a pregnancy after bariatric surgery were more frequently diagnosed with anemia in the preconception period (19% vs. 2%, p<0.0001) and had a lower frequency of hypertensive disorders in pregnancy, gestational diabetes, and cesarean section (p<0.02) compared with women who had a pregnancy before surgery. The mean time between surgery and delivery was about 2.25 years for those with a pregnancy after surgery, and 1.66 years for those with pregnancy before bariatric surgery. There was no difference in incidence of multifetal pregnancy between the two groups, an outcome that should not be affected by bariatric surgery. Screening for syphilis in pregnancy occurred with high frequency in both groups, slightly more (92% vs. 85%) in those with pregnancy after bariatric surgery.
Table 3 presents the frequency of testing for micronutrient deficiencies during preconception and pregnancy. The overall rates of testing were low, and the highest (51%) were for vitamin B12 in the preconception period for women with pregnancy after bariatric surgery, as compared to 2% in women with pregnancy before bariatric surgery (p<0.001). There were no major differences in testing frequency if analyses were restricted to Roux-en-Y procedures alone.
“Basic” and “optimal” testing defined in Table 1. χ2 tests used to determine p-values.
Figure 2 shows that laboratory testing occurred more frequently during both the preconception period and pregnancy after surgery than before surgery (p<0.003). The only exception was optimal lab testing for vitamin B12 during pregnancy, which did not differ, and was very low in both groups (0%–1%, p=0.14). Table 4 shows the multivariate analysis. Predictors of laboratory testing for nutrient deficiency included a diagnosis of nutritional anemia for iron (OR 1.772; 95% CI 1.084, 2.898), folate (2.021; 1.240, 3.295), vitamin B12 (1.955; 1.199, 3.189) and a high number of visits for iron (2.023; 1.208, 3.386), folate (1.838; 1.086, 3.110), and vitamin B12 (1.938; 1.168, 3.215). With vitamin B12 as the outcome, a moderate number of outpatient visits was associated with increased laboratory testing (OR 1.681; 95% CI 1.028, 2.749). Maternal age had no effect on any micronutrient laboratory test.
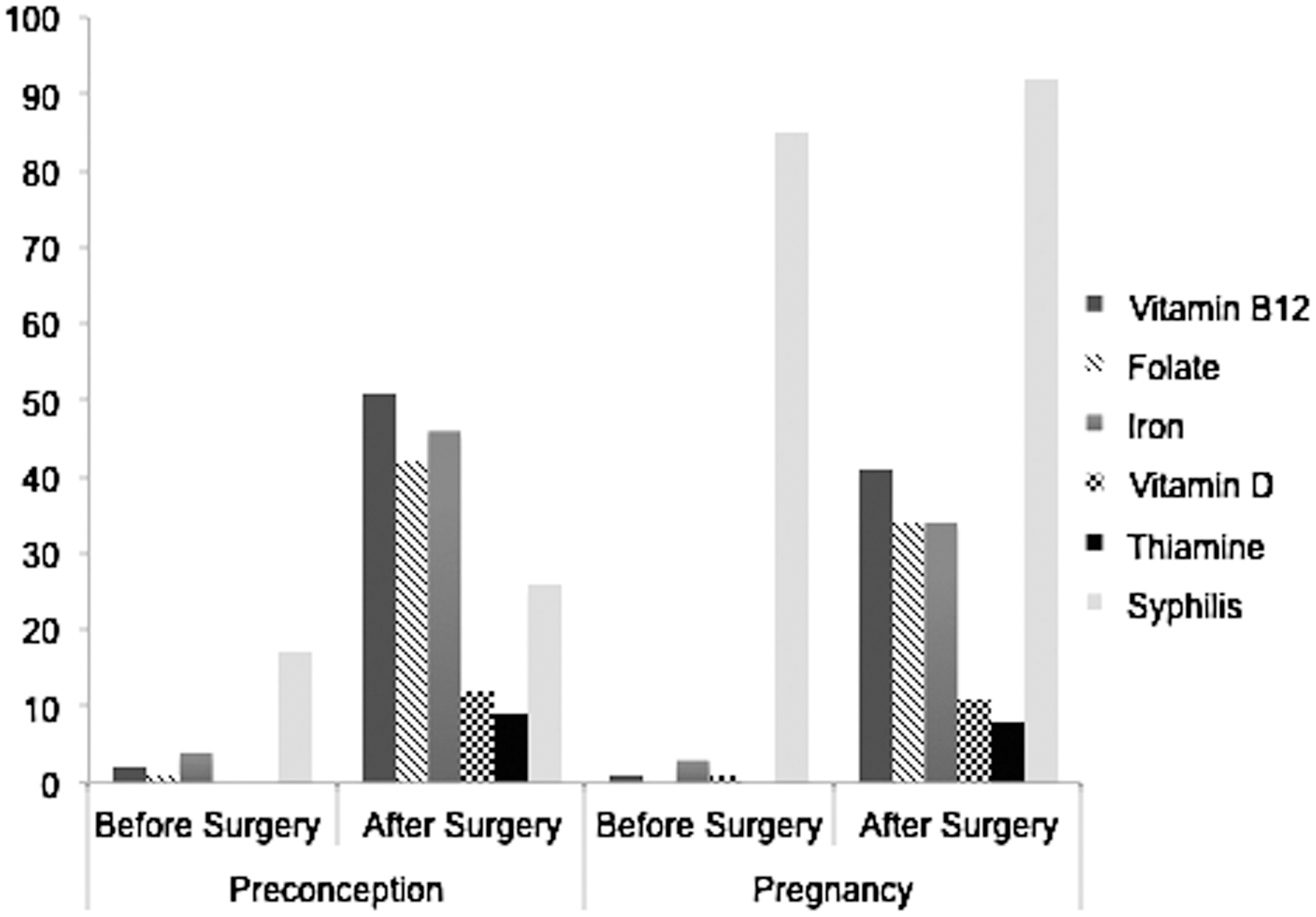
Differences before and after bariatric surgery determined using χ2 test. Syphilis screening during pregnancy is the control measure. All comparisons other than the control measure of prenatal syphilis screening are p<0.001.
Bolded terms represent predictors of micronutrient deficiency with p<0.05.
CI, confidence interval; Determined through logistic regression analyses, OR (95% CI).
The frequency of diagnoses of the deficiencies is presented in Table 5. In general, nutrient deficiencies occurred more often in women with pregnancies after bariatric surgery (p<0.0001 during the preconception period and p<0.006 during pregnancy) and were most frequent for vitamin B12 in both preconception (13%) and pregnancy (12%; p<0.0001). Vitamin D deficiency in preconception was the only exception, with 2% of women with pregnancies after surgery and 1% in those with pregnancies before surgery having vitamin D deficiency.
Micronutrient deficiency defined in Table 1. χ2 tests used to determine p-values.
Discussion
In our investigation of testing for and diagnosis of micronutrient deficiencies during preconception and pregnancy after bariatric surgery, overall frequency of laboratory testing was low but was significantly higher in those with a pregnancy after surgery. Laboratory testing occurred most often for micronutrient deficiencies that are associated with anemia, iron, folate, and vitamin B12, but it was still only performed in half of those at risk. In women who became pregnant after surgery, deficiencies in folate, iron, thiamine, and vitamin B12 were relatively rare (all<15%) but occurred more commonly during the preconception period, and deficiencies in all micronutrients were seen more often during pregnancy. We also found an association between laboratory testing and more frequent clinical visits prior to and during pregnancy, as well as an association between laboratory testing and the diagnosis of nutritional anemia.
Bariatric surgery is an effective treatment for severe obesity, leading to improvement in obesity-related comorbidities and mortality. 6 The weight loss promoted by bariatric surgery has been shown to improve pregnancy outcomes, including hypertensive disorders of pregnancy, preeclampsia, preterm birth, and gestational diabetes. 6 –9 However, weight loss after surgery is related to decreased caloric consumption and a state of some malabsorption. The type of bariatric surgeries that lead to the highest risk of nutrient deficiencies are extended Roux-en-Y gastric bypass procedures, or bilio-pancreatic diversions. 11 These malabsorptive procedures may cause deficiencies of fat-soluble vitamins, including vitamins A, D, E, and K. 11 Iron is principally absorbed in the duodenum, which is bypassed in a Roux-en-Y gastric bypass procedure. 22 In our investigation, 75% of women with pregnancies after surgery underwent a Roux-en-Y surgical procedure. Only 8% underwent a restrictive procedure, either gastric banding or vertical banded gastroplasty, which carries a lower risk of micronutrient malabsorption postoperatively.
Clinically, the nutritional deficiencies we identified may manifest as anemia in those women who became pregnant after bariatric surgery. In our analysis, nearly one quarter of those with a pregnancy after surgery carried a diagnosis of nutritional anemia, a prevalence that is significantly higher than in those with pregnancy before surgery (13%). Investigations over the past decade suggest that iron deficiency early in pregnancy may result in preterm birth. 15 In a small study of 16 patients who had received Roux-en-Y gastric bypass surgery and were taking daily routine multivitamin supplementation, the frequency of iron deficiency at 3 years was 54%, and the diagnosis of anemia was 63.9%. 23 A recent study of 170 patients assessed anemia and iron deficiency at 36 months after Roux-En-Y gastric bypass surgery and found 33.5% with anemia and 23.5% with iron deficiency as determined by low ferritin concentrations. 24 Nomura and colleagues 25 identified higher need for intravenous iron supplementation or red blood cell transfusion among women who conceived 4 years or more after surgery.
Beyond iron, deficiencies of other essential minerals and fat-soluble vitamins may also impact on fetal and infant health. Low 25(OH) vitamin D levels in pregnancy may contribute to increased placental inflammation and even preeclampsia. 12,26 Maternal folate deficiency is implicated in fetal neural tube defects. 14,21 The effects of vitamin B12 deficiency on pregnancy outcomes have not been well-studied; however, one study showed an association with future insulin resistance in the offspring. 27 Finally, bariatric surgery may increase the risk of small for gestational age infants, perhaps in part due to nutrient deficiencies resulting from malabsoption after surgery. 28
The American College of Obstetrics and Gynecology Practice Bulletin and a clinical practice guideline produced by a consortium of the American Association for Clinical Endocrinologists, The Obesity Society, and the American Society for Metabolic and Bariatric Surgery recommend micronutrient screening in pregnant women after bariatric surgery. 19,20 Based on expert opinion and supplemented by case reports of observed nutrient deficiencies after bariatric surgery, these guidelines recommend testing for relevant micronutrient deficiencies in all individuals every 3–4 months during the first year after bariatric surgery and annually thereafter. 22,29 –31 Our findings show that while women who have a pregnancy after surgery are screened more often than those with a pregnancy before surgery, the occurrence of any laboratory testing still remains far below goal. However, several gaps remain in our knowledge of the clinical relevance and impact of these nutrient deficiencies, such as maternal and fetal outcomes and optimal treatment doses and routes of supplementation. Longitudinal evaluation of the nutritional consequences of bariatric surgery on pregnancy and child health outcomes through well-characterized prospective cohort studies could support evidence-based guideline development. Furthermore, we need to improve overall preconception and pregnancy care for women following bariatric surgery, through care coordination between multiple providers to standardize the process of laboratory testing and capture missed opportunities for treatment for micronutrient deficiency.
Several limitations of this qualitative study should be considered. First, our analysis included the use of insurance claims data rather than data collected from clinical encounters. We relied on definitions for micronutrient deficiencies using ICD-9 and CPT codes entered by physicians, which are subject to errors, overcoding, and undercoding. Given the limitations of claims data, we cannot determine the clinical indications leading to physicians' ordering of laboratory testing. Additionally, claims data may not provide population-based prevalence of micronutrient deficiencies in this population, since not everyone received a screening test and opportunity for diagnosis. However, we believe these prevalences may be more representative of actual clinical practice. For the article's primary outcome of frequency of testing, our methodology using claims data does represent actual testing completion rates. Second, ICD-9 diagnosis codes may have been used as indications to support laboratory testing rather than as reflective of actual clinical diagnoses, thus overestimating the frequency of micronutrient deficiencies we reported, which were overall quite low. Third, our data did not include sociodemographic or other clinical information, such as socioeconomic status or parity, limiting our examination of predictors of receipt of testing. However we were able to include maternal age and insurance plan or region. Fourth, we cannot assess causality using this observational data source. We observed an association between more outpatient clinical visits and increased laboratory testing for micronutrient deficiency, which could reflect confounding by indication since women with pregnancy after bariatric surgery may have required more frequent monitoring because of increased pregnancy risk and therefore were more likely to receive laboratory testing because of their complexity. Thus, the number of outpatient visits may not be a predictor of nutrient deficiency but rather a consequence of surgical or medical complications. Fifth, we found that a diagnosis of nutritional anemia was positively associated with receipt of laboratory testing for iron, folate, and vitamin B12. However, the ordering of the laboratory tests for these micronutrients may have been linked with an ICD-9 code corresponding to anemia, even though the clinical diagnosis of anemia may not have existed. Thus, coding for anemia in women with pregnancy after bariatric surgery may reflect a diagnosis code used for laboratory testing for iron, folate, or vitamin B12, rather than a true diagnosis of nutritional anemia.
The strengths of our study included a large dataset with over 1400 women and continuous enrollment information throughout the periods of preconception and pregnancy. Although our data did not include information on maternal BMI, our comparison of laboratory testing during preconception and pregnancy before and after surgery was designed to compare women who had similar BMI and potential for obesity-related comorbidities. We restricted our analysis to those with continuous coverage during the preconception and pregnancy periods to serve as a proxy for access to care and to minimize loss to follow-up. Syphilis testing occurs with the high frequency among those becoming pregnant before or after surgery, suggesting that women in our study population are receiving other recommended prenatal screening tests regardless of bariatric surgery status.
In conclusion, bariatric surgery and the resulting weight loss prior to conception can benefit maternal and fetal outcomes in pregnancy, but may also result in malabsorption and micronutrient deficiencies that can have a similarly detrimental impact on the health of mother and child. Annual laboratory testing for all those who are more than 1 year out from surgery, conforming to expert recommendations, may reduce the potential risks of essential nutrient deficiencies on maternal and fetal health. Our investigation supports the need for future studies to assess whether guidelines on laboratory testing for micronutrient deficiency are being met in women who become pregnant after bariatric surgery. Promotion of scheduled testing by a designated physician providing care during the preconception period may help to ensure adherence to expert recommendations and translate to improved care.
Footnotes
Acknowledgments
The data set used in this study was originally created for a different research project on patterns of obesity care within selected Blue Cross Blue Shield plans. The previous research project (but not the current study) was funded by unrestricted research grants from Ethicon Endo-Surgery, Inc. (a Johnson & Johnson company), Pfizer, Inc., and GlaxoSmithKline. The data and database development support and guidance were provided by the BCBS Association, BCBS of Tennessee, BCBS of Hawaii, BCBS of Michigan, BCBS of North Carolina, Highmark, Inc. of Pennsylvania, Independence Blue Cross of Pennsylvania, Wellmark BCBS of Iowa, and Wellmark BCBS of South Dakota. We thank the Blue Cross and Blue Shield plans and their staff members. Preliminary findings were shared with the supporting organization, and they were invited to review the manuscript. They did not participate in the design and conduct of the study, data collection, analysis or interpretation, or preparation or submission of the manuscript. M.D.G. was supported by a training grant from the National Institutes of Health (NIH T32HL00718). Creation of the database was funded by Ethicon Endo-Surgery, Inc., GlaxoSmithKline, and Pfizer, Inc. Data and support were provided by Blue Cross Blue Shield of Michigan and Highmark. Support was provided by the Blue Cross Blue Shield Association. The supporting organizations were kept informed of the study's progress and shared their expertise on certain aspects of the study.
Author Disclosure Statement
The authors declare no conflicts of interest.
Appendix A
Appendix B
Delivery
650 (normal delivery), 651 (multiple gestation), V27.0 (mother with single liveborn), V27.1 (mother with single stillborn), V27.2 (mother of twins, liveborn), V27.3 (mother with twins, 1 stillborn), V27.5 (mother with other multiple births, all liveborn), V27.6 (mother with other multiple births, some liveborn).
Gestational Diabetes
Hypertensive Disorders of Pregnancy
Anemia
281.1 (vitamin B12 deficiency anemia), 281.2 (folate deficiency anemia), 281.3 (other specified megaloblastic anemias, not elsewhere classified), 280 and 280.1 and 280.9 (iron deficiency anemia)