
Abstract
This article reviews some of the current challenges for maternal death review in the United States, describes key findings from an assessment of U.S. capacity for conducting maternal death reviews, and introduces a new Maternal Mortality Initiative that aims to develop standardized guidelines for state- or city-based maternal deaths review processes.
Introduction
Early in the 21
Changes in classification of maternal death and differences among states in how they collect and provide information necessary to identify maternal deaths are significant challenges to the accurate and consistent reporting of maternal mortality indicators. Both CDC systems mentioned rely on vital statistics data alone, making it difficult to differentiate changes in measures due to changes in case ascertainment versus changes in the risk of death. 3 State- and urban-based maternal death review processes (MDRPs) use information beyond that provided by vital statistics, positioning them best to comprehensively identify and assess cases, and most importantly, to identify opportunities for effective intervention. It is from MDRPs that we have learned that between 20% and 50% of maternal deaths in the United States are preventable. 6 –9
State- and urban-based maternal death reviews have served a core public health function since the early 1900s. Specifically, maternal death review findings have been used to improve both clinical and nonclinical systems of care for women and families. In this report, we describe a new national maternal mortality initiative and share findings from a capacity assessment for conducting maternal death reviews that has been used to select participating sites.
CDC's Maternal Mortality Initiative
CDC's Division of Reproductive Health developed a new 2-year Maternal Mortality Initiative and invited several national partners and stakeholders with expertise in improving women's health (Association of Maternal and Child Health Programs, AMCHP; American Congress of Obstetricians and Gynecologists, ACOG; and Health Resources and Services Administration's Maternal and Child Health Bureau, HRSA/MCHB) as collaborators. The Association of Maternal and Child Health Programs, in partnership with CDC Division of Reproductive Health, developed an assessment tool that helped to identify the 14 state-based maternal mortality review committees and one urban-based maternal mortality review committee that were invited to participate in the Initiative (Fig. 1). The two selection criteria used to identify maternal mortality review committees to participate in the Maternal Mortality Initiative were (1) maternal deaths are identified by the MDRP using data linkages, and (2) case reviews of maternal deaths are conducted by a multidisciplinary committee.
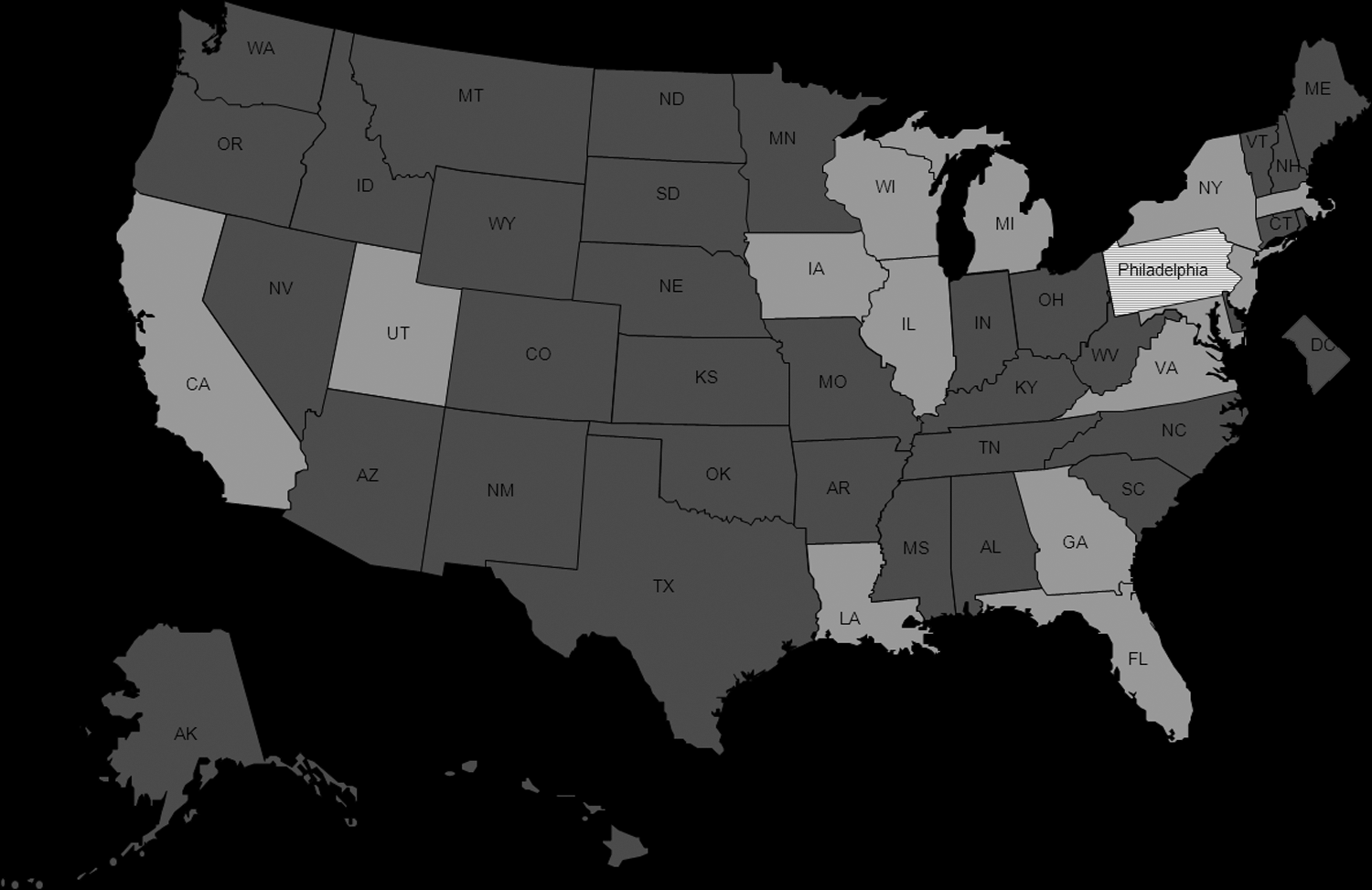
Maternal mortality review committees participating in the Centers for Disease Control and Prevention (CDC) Maternal Mortality Initiative.
Assessing capacity for conducting maternal death reviews in the United States
The selection of the participating sites was based on a capacity assessment conducted by AMCHP in January and February 2012 in partnership with the CDC Division of Reproductive Health. The 22 state and two urban communities known to conduct maternal death reviews in 2011 were invited to complete a 33-item online assessment. The assessment was organized into six topic areas related to maternal death reviews: funding and staffing, case identification, data abstraction and review, legislation, challenges, and examples of translating maternal death review findings into action. Nineteen state-based MDRPs and one urban-based MDRP completed the assessment. A brief description of key assessment findings within each of the six topic areas is presented in Table 1.
MDRPs, maternal death review processes.
The Maternal Mortality Initiative in action
The overarching goal of the CDC Division of Reproductive Health Maternal Mortality Initiative is to develop standardized guidelines for state- or city-based MDRPs, including recommendations for clinical and community actions. The specific objectives of the Initiative are to • Provide guidance for case ascertainment, document abstraction, review, and recommendations that could be used by interested states • Document data linkage processes from data access and acquisition to software and algorithm • Assess capacity and challenges for translating maternal death review findings into action and document examples of successful translation.
Through conference calls and in-person meetings, teams representing the 15 selected maternal mortality review committees worked together with scientists from CDC and the other Initiative partners to achieve the Initiative objectives. Each of the 15 selected maternal mortality review committees identified representatives to participate in the first in-person meeting that took place in Atlanta, Georgia, in November 2012. The teams most commonly included a representative of vital registration, a representative of the Title V MCH Block Grant Director, the chair of the maternal mortality review committee, the coordinator of the maternal mortality review committee, and an MCH epidemiologist.
Five teams presented briefly on the processes used by their maternal mortality review committees, confirming that the persistent racial disparities and shifts in cause of maternal death observed nationally are also being observed at state and urban levels. The 15 teams split into three workgroups, with five maternal mortality review committee teams in each work group. Discussed by each workgroup were maternal death case ascertainment, available data sources, and possible data linkages for MDRPs. In March 2013, representatives from the 15 maternal mortality review committees met again in-person to discuss and document case review processes and the effective translation of review findings into action.
Conclusion
With many state- and urban-based MDRPs dependent upon in-kind support, and given the large number of MDRPs operating without authorizing state legislation for convening state- or urban-based maternal death reviews, it may not be surprising that MDRPs transition in and out of operation over time. The assessment of MDRPs revealed that although some MDRPs have been in place for more than 80 years, the median age of assessed MDRPs in early 2012 was only 3 years.
The large proportion of MDRPs supported by Title V Block Grant funding, despite the absence of Title V Block Grant National Performance Measures related to maternal mortality and morbidity, provides evidence of the importance and value placed on these reviews by states. In the presence of multiple challenges, state- and urban-based MDRPs have informed the development of significant actions to improve maternal health outcomes. For example, the California Pregnancy Associated Mortality Review (CA-PAMR), initiated in 2004, identified quality improvement opportunities and compiled toolkits for maternity care improvement. Michigan has had an active review process since 1950 and recently developed a webinar for their state maternal infant health program staff on pregnancy complications, with a special focus on postpartum cardiomyopathy.
The Maternal Mortality Initiative addresses two of the challenges identified in the AMCHP assessment—the lack of standards for review processes and the lack of opportunities for networking with other state- and urban-based MDRPs. Drawing from their diverse experiences, the partnership between state and urban maternal mortality review committees, CDC, AMCHP, ACOG, and HRSA/MCHB began the work of documenting best practices and developing standard recommendations for maternal death reviews. At the conclusion of this 2-year Maternal Mortality Initiative, it is expected that existing maternal mortality review committees will have strengthened their review processes, while new review committees will have a well-developed start-up guide and a catalog of successfully translated review findings to address common challenges experienced by their colleagues in other states and urban areas.
Footnotes
Acknowledgments
The authors would like to acknowledge LCDR Deborah Dee, PhD, MPH, for her review of the assessment tool. The authors also would like to acknowledge the 19 state and one urban MDRPs that participated in the assessment, and the 15 maternal mortality review committees that are contributing to the Maternal Mortality Initiative. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.