
Abstract
Background:
Many barriers to cervical cancer screening for Hispanic women have been documented, but few effective interventions exist. The Community Preventive Services Task Force recommends increasing cervical cancer screening through various methods. Building on this evidence, the Centers for Disease Control and Prevention funded the research and testing phases for an evidence-based and theoretically grounded intervention designed to increase cervical cancer screening among never and rarely screened Hispanic women of Mexican descent. In this article, we describe the development process of the AMIGAS (
Methods:
The AMIGAS team was a collaboration among researchers, promotoras (community health workers), and program administrators. The multiyear, multiphase project was conducted in Houston, Texas; El Paso, Texas; and Yakima, Washington. The team completed several rounds of formative research, designed intervention materials and methodology, conducted a randomized controlled trial, created a guide for program administrators, and developed an intervention dissemination plan.
Results:
Trial results demonstrated that AMIGAS was successful in increasing cervical cancer screening among Hispanic women. Adaptation of AMIGAS showed minimal reduction of outcomes. Dissemination efforts are underway to make AMIGAS available in a downloadable format via the Internet.
Conclusions:
Developing a community-based intervention that is evidence-based and theoretically grounded is challenging, time-intensive, and requires collaboration among multiple disciplines. Inclusion of key stakeholders—in particular program deliverers and administrators—and planning for dissemination and translation to practice are integral components of successful intervention design. By providing explicit directions for adaptation for program deliverers, relevant information for program administrators, and access to the intervention via the Internet, AMIGAS is available to help increase cervical cancer screening among Hispanic women and other women disproportionately affected by cervical cancer.
Introduction
Cervical cancer incidence and death rates have declined since the introduction of the Pap test, yet rates are still higher for Hispanic women than for non-Hispanic white women. 1 Healthy People 2020 has identified targets for cervical cancer incidence (7.1 new cases per 100,000 women) and mortality (2.2 deaths per 100,000 women) 2 that are lower than the current incidence and death rates for Hispanic women—10.9 new cases per 100,000 and 2.9 deaths per 100,000 women, respectively. 1 Cervical cancer can be prevented through consistent use of the Pap test according to guidelines. 3 The most recent guidelines (2012) from the United States Preventative Services Task Force, the American Cancer Society, and the American College of Obstetricians and Gynecologists recommend a Pap test every three years for women 21–30 years; a Pap test and HPV test every 5 years or a Pap test every 3 years for women 30–65 years. 3 –6 Healthy People 2020 has also identified a cervical cancer screening target (93%). 2 Almost 84% of women in the United States report being screened for cervical cancer. 7 However, Hispanic women, particularly those of Mexican origin and those residing in border and rural regions of the United States, are among the least likely to be screened. 7,8
The Centers for Disease Control and Prevention (CDC) has a long-standing commitment to providing cervical cancer screening services to low-income, uninsured women through the National Breast and Cervical Cancer Early Detection Program (NBCCEDP) (
Many barriers to cervical cancer screening for Hispanic women have been documented (Table 1). 13 –18 Still, few evidence- and theory-based interventions have proven effective in increasing Pap testing among Hispanic women. 19 –21 In 2005, the Community Preventive Services Task Force (Task Force) found that small media was an effective way to increase cervical cancer screening. 22 In 2010, the Task Force also found that one-on-one education and client reminders were effective strategies for increasing cervical cancer screening. 22 Notably, few intervention strategies in the Community Guide were designed for Hispanic women or were intended to be delivered by community health workers. Importantly, the literature, outside of the studies included in the systematic reviews, contained few examples of interventions that tested the effectiveness of their components' contribution to the primary outcome, thereby providing limited useful information for implementation and adaptation of the intervention to community demands or context. 23
When desiring an intervention to be used effectively in practice, it is important to build it from the beginning with consideration for extant challenges to implementation. 24,25 Partnering with and being responsive to community stakeholders increases the likelihood that interventions will be appropriate for and meet the needs of the community when disseminated. Decision makers, including program deliverers and program administrators, comprise a particularly important stakeholder group when considering adoption or implementation of an intervention. Using a community participatory paradigm is one method to ensure the perspectives of the ultimate beneficiary, as well as intermediary groups, are continually relevant to the intervention development process. 26
AMIGAS (
CDC is committed to improving the nation's health, and this includes the development, evaluation, and translation of effective research into practice. 30 This article will describe the development of the AMIGAS intervention and highlight the integration of scientific evidence and community-based participatory research principles. These methods provided a foundation that ensured AMIGAS was effective for the intended audience while meeting the needs of program deliverers and administrators. We will also identify emerging opportunities for dissemination, adaptation, and implementation of the intervention.
Intervention Development Process
AMIGAS emerged as a product of four broad phases: formative research, materials development and testing, intervention trial, and administrator's guide development and testing (Fig. 1). Funded across all phases by CDC, this process was guided by research evidence and theory and used a community-based participatory research framework.
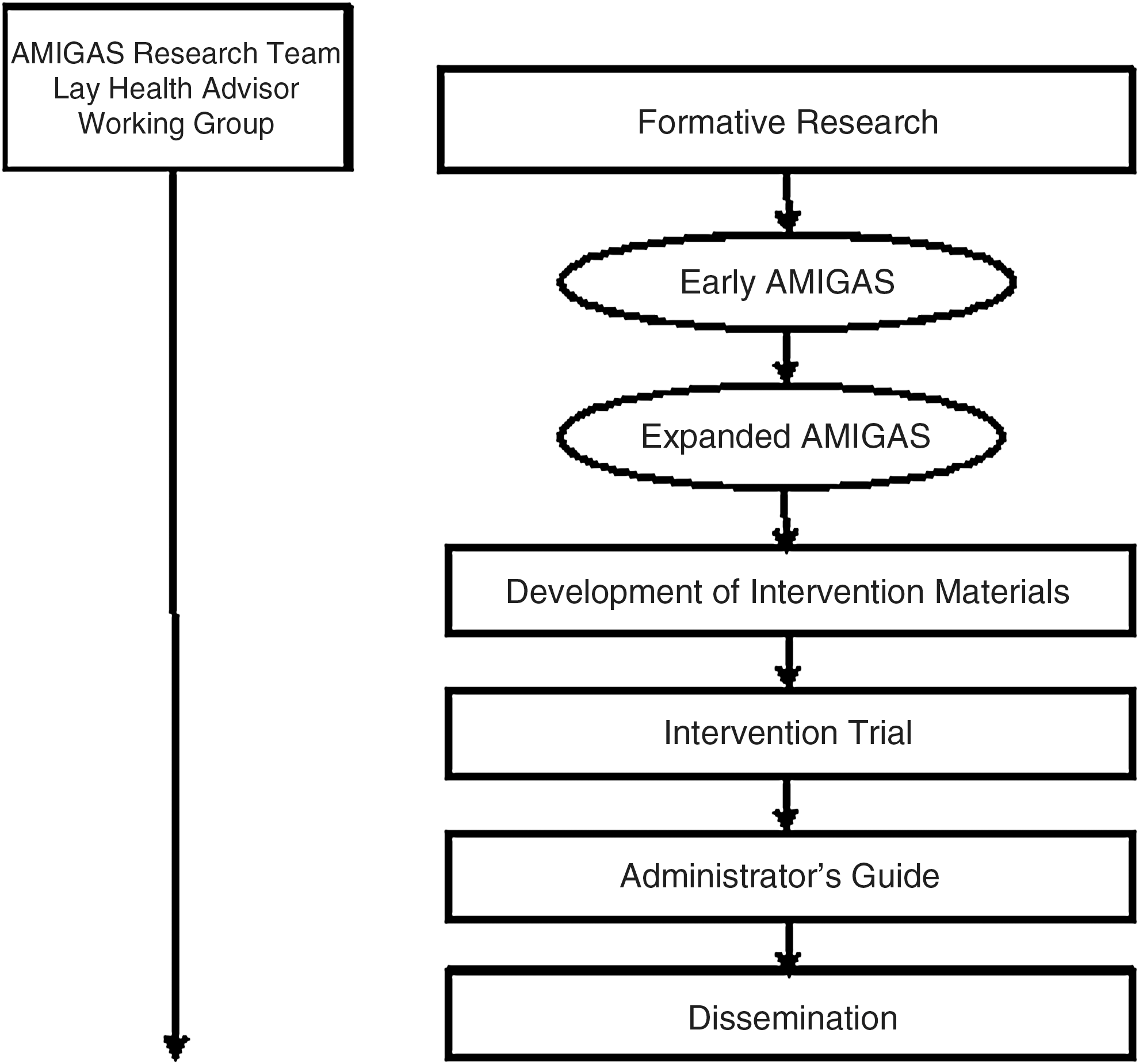
AMIGAS Intervention Development Process.
The AMIGAS team
The AMIGAS team included researchers, promotoras, and program administrators with years of experience in healthcare system management, plain language writing, community engagement, behavioral science, methods and statistics, economics, health disparities, and cancer prevention and control in the Hispanic community. The Lay Health Advisor Working Group (LHAWG), comprised of promotoras and program administrators, was an integral participant of the AMIGAS team throughout all phases of the project. These community experts were invited to participate in the working group by AMIGAS researchers who knew them from reputation and prior research collaborations across the United States.
Formative research
Formative research for the AMIGAS intervention was both qualitative and quantitative and was carried out over two time periods. Initial work was completed by researchers at the University of Texas-Houston, School of Public Health and funded by CDC. Formative research for the AMIGAS intervention was both qualitative and quantitative and was carried out over two time periods. A survey informed by multiple behavioral science theories (Health Belief Model, 31,32 Theory of Reasoned Action, 33 Social Cognitive Theory, 34 and the Transtheoretical Model 35,36 ) was administered to over 500 Hispanic women in the El Paso area to gather information about risk perception, barriers and facilitators to cancer screening, and group preferences regarding characteristics of interventions. Focus groups addressed several key questions including (1) where women receive healthcare, (2) healthcare experiences, (3) knowledge and experience with cancer, (4) feelings and beliefs about having a Pap test, (5) factors that would make it easier or harder to get a Pap test, and (6) sources of social influence. The resultant intervention was in Spanish only and was designed for use at the US-Mexico border. It contained a simple instruction guide for promotoras, a flipchart, and a video augmented by existing community informational brochures. This initial version of AMIGAS was evaluated in individual educational sessions with a sample of 200 women. 13,14
CDC was interested in developing a cervical cancer screening intervention for Hispanic women, including those residing in rural (nonborder) and urban areas. Formative research funded by CDC and conducted by Battelle in English and Spanish also provided valuable qualitative information about the facilitators and barriers to the receipt of cervical cancer screening, and attitudes and opinions about the Pap test for Hispanic women in these new locations. In addition, the focus group respondents provided key information about intervention design, mode of delivery, messages, and communication strategies.
The early version of AMIGAS was a promising alternative to investing resources into the development of an entirely new intervention. Importantly, CDC identified ways to expand the early version of AMIGAS to be relevant to Hispanic women of Mexican descent living on the U.S.-Mexico border, in rural areas, and in urban centers.
Focus group and survey results validated that the attitudes, opinions, and perceptions of the U.S.-Mexico border participants were consistent with those of the rural and urban participants (unpublished data). Collectively, the formative research findings clearly indicated that an expanded intervention for Hispanic women would have to do the following to succeed: (1) increase knowledge about cervical cancer and Pap testing, (2) encourage positive attitudes about Pap testing, (3) acknowledge feelings and concerns about cervical cancer screening, (4) target important social referents such as daughters and husbands to help encourage Pap testing, (5) reduce system-related barriers by increasing clinic hours and availability of bilingual staff or translators, and 6) inform women about low-cost programs and services to address concerns about access to healthcare. Major modifications included developing an English version of the intervention, revising materials, and developing additional intervention components to facilitate uptake by women, promotoras, and program administrators.
One last formative component of the expanded AMIGAS included assessing the health literacy of a small sample (n=9) of Hispanic women using the Short Test of Functional Health Literacy in Adults (S-TOFHLA) administered in English and Spanish. 37,38 Results from the S-TOFHLA found a range of functional health literacy among our sample from a low of 6 (inadequate) to a high of 36 (adequate) with a mean score of 25 (out of a possible 36 points). a This information was gathered to inform the language used in message design.
Development of intervention materials
The expanded AMIGAS was designed to be delivered by promotoras, provide women with new knowledge and skills, acknowledge and discuss beliefs about cervical cancer and Pap testing, reinforce positive behavior, and provide information on local services. New materials included a promotora instruction guide; a resource sheet; a promise sheet (mi promesa); diagrams of the Pap test procedure and the female reproductive system; and a contact sheet (Table 2). Consistent attention to health literacy, particularly the use of plain language (
All AMIGAS intervention components are in English and Spanish, unless otherwise noted.
Materials were tested in two half-day workshops, in English and Spanish separately, with 17 promotoras in San Diego, California, and Yakima, Washington. Intervention components were assessed for usability, acceptance, and comprehension. Results from these focus groups informed revisions to materials and instructions on some of the intervention components. After revisions were completed, investigators and the LHAWG conducted a final review.
Intervention trial
AMIGAS intervention materials were tested for effectiveness—the validated receipt of Pap testing at 6 months—together as a full intervention, as well as the relative effectiveness of the intervention's small media components (e.g., flipchart and video). The trial, conducted in Houston, Texas (urban); El Paso, Texas (border); and Yakima, Washington (rural), was approved by the University of Texas Health Science Center-Houston Committee for the Protection of Human Subjects and the Fred Hutchinson Cancer Research Center Institutional Review Board. The trial included 613 women who were administered the one-on-one version of AMIGAS by a trained promotora. Results indicated that AMIGAS was successful in increasing the receipt of Pap tests among Hispanic women in a one-on-one setting compared to the control condition (e.g., usual care without intervention materials), and no differences existed among the intervention arms. 29 The magnitude of the effect in the intent-to-treat and the per-protocol analyses was greater than had been reported in previous interventions to increase screening for cervical cancer in Hispanic women. 40,41 The trial also included a cost-effectiveness analysis to assess the cost of conducting the intervention at all study sites. A report on the findings from the cost-effectiveness evaluation is under review.
Administrator's guide
A notable departure from traditional implementation materials is found in the AMIGAS Administrator's Guide. Few interventions include a document to assist program administrators with decisions about the fit, adoption, adaptation, staffing, and management of a selected intervention.
40
Discussions with the program administrators in the LHAWG had highlighted the need to assist health program administrators in decision making and planning related to adoption and implementation of AMIGAS. Components of the AMIGAS Administrator's Guide included an executive summary; intervention purpose, benefits, history and development; and sections to aid in the selection, preparation, initiation, maintenance, and local adaptation of the intervention. The AMIGAS Administrator's Guide also includes handouts, a sample training agenda for promotoras who will deliver the intervention, informational sheets about cervical cancer and Pap testing, and evaluation forms. Nine program administrators provided feedback through a questionnaire about design, format, scope of information, and program planning guidance. Responses indicated that the AMIGAS Administrator's Guide was well designed and included the necessary materials for program administrators to select and implement AMIGAS. Additional advice from the review panel prompted a minor revision of some text, graphics and layout for the final version. We plan to disseminate the AMIGAS Administrator's Guide with the AMIGAS intervention via the Research-tested Intervention Programs (RTIPs) section of Cancer Control P.L.A.N.E.T. (Plan, Link, Act, Network with Evidence-based Tools) (
Conclusions
AMIGAS is a successful intervention developed in partnership with the community and designed to increase cervical cancer screening among never and rarely screened Hispanic women of Mexican descent. Recruitment of traditionally medically underserved populations requires more effort but can be accomplished when activities are undertaken in conjunction with the community. 42,43 The extensive formative research, as well as the incorporation of community-based participatory research principles, highlight the importance of including multiple theoretical and practical components in an intervention designed for implementation in the community. Implementation of evidence-based interventions is one method to expand preventive healthcare use, including cervical cancer screening. Future activities for study investigators, other researchers, and practitioners include revising AMIGAS intervention components for use in other traditionally medically underserved populations, including other U.S. Hispanic subpopulations, African American women in urban and rural areas, and women living in Mexico and Latin America.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of the AMIGAS Lay Health Advisor Working Group, including Bea Barraza and Raquel Corona (Colaborativo SABER), Lorena Sprager (Lorena Sprager and Associates, LLC of the Clear Language Group), and Stella Vasquez and Ana Lucas (Yakima Valley Farm Workers Clinic), for their time, contributions, and commitment to the AMIGAS intervention; and Carolina Mejia (Battelle and University of North Carolina at Chapel Hill) for her assistance on the design of the AMIGAS intervention materials.
Author Disclosure Statement
Research for this publication was supported by Centers for Disease Control and Prevention Cooperative Agreements # S1166-19/21 and U48-DP000057 and Contracts # 200-98-0102, 200-2002-00573, and 200-2008-27956. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
a
TOFHLA, Test of Functional Health Literacy in Adults purchased from Peppercorn Books & Press Inc., P.O. Box 693, Snow Camp, NC 27349. License number 043/04, issued on June 4, 2004.